Download presentation
Presentation is loading. Please wait.

1
Complications Of Vena Cava Filters Amr Fares MD,FRCS Assistant prof. of surgery,Weill cornell college of medicine Vascular surgery consultant Doha –Qatar

2
Types Short-term complications :associated with the placement procedure Long term complications :arise from the effect of the filter locally or in the proximal veins

3
It is difficult to understand the true incidence and importance of many of these complications due to the significant variation in patient populations, filter types, co-morbid disease burden, and variability in follow-up intensity and duration.

4
Other factors Filter material and design. Route and technique of placement. Indication for placement. Category of filter. Timing of removal of retrievable filters

5
As opposed to open procedures where recovery can usually be accomplished via standard methods, there are limited “rescue” options for endovascular procedures.

6
Misplacement A cavagram is essential for identifying key landmarks Failure to perform an adequate cavagram or misinterpreting it. Jugular approach may lead to cannulation of the hepatic veins and into the portal system.

7
Misplacement (cont.) If a sheath is being used for the cavagram and the landmarks cannot be visualized, placing a multi-side hole catheter (pigtail catheter) and using the power injector can often provide excellent imaging. If performing the procedure under transabdominal US or with IVUS, one must be familiar with these techniques

8
Pulmonary Embolus VCFs do not provide complete protection from subsequent PE. Could be due to primary failure of the filter, embolization of filter thrombus, or embolization from UL. The reported mortality with a recurrent PE in the Venatech filter is up to 50% and with the Bird’s Nest Filter is 90%.

9
In PREPIC trial, there was a documented incidence of 6.2% for recurrent PE in the group with filters in place. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prevention du Risque d’Embolie Pulmonaire Par Interruption Cave Study Group. N Engl J Med 1998;338:409-15.

10
The decision about when to remove the VCF is highly subjective PE in this situation can result from dislodgment of clot during the removal procedure or from embolization of a new or existing DVT after the protective filter has been removed.

11
Perforation Filter angulation or tilting is often the cause of perforation and is commonly due to undersizing the IVC. Duodenal perforations as well as aortic perforation have been documented with perforation of the IVC.

12
Duodeno-caval fistula is a late complication of IVC filters but can present with life-threatening bleeding. Penetration into the aortic wall may lead to pseudo-aneurysm formation and can also lead to mural thrombus formation with distal embolisation.

13
Caval Thrombosis The reported incidence of caval thrombosis is less than 10% with the newer devices There is continued debate about whether it is related to the presence of a foreign body and obstruction to flow, thus representing a complication of the filter, or due to the accumulation of emboli caught by the filter, and thus filter success.

15
It can cause significant morbidity including lower extremity swelling, renal failure (suprarenal thrombosis), and pulmonary embolisation.
, and pulmonary embolisation.")
16
Migration Filters that are not sized appropriately are the cause of migrations. It can migrate to the right atrium and ventricle as well as the PA. The Greenfield filter, was found to have a migration rate of 3 mm or more in 8% of patients

17
If component fracture occurs, a filter may migrate many years after placement. Migration of the filter to the cardiac or pulmonary systems requires immediate intervention to remove the device Done by an endovascular approach but may require an open thoracotomy or sternotomy.

18
Postthrombotic Syndrome Patients with a VCF have roughly double the incidence of DVT compared with patients without VCF. Incidence of edema of 43% and chronic skin changes 12%. Fox MA, Kahn SR. Postthrombotic syndrome in relation to vena cava filter placement: a systematic review. J Vasc Interv Radiol 2008;19:981-5.

19
Access Site Thrombosis The incidence of insertion site thrombosis occurs in 10% of cases. Treatment should be standard anticoagulation if possible and most of these occlusions can be expected to re- cannalise and resolve.

20
Renal Vein Occlusion In patients with known hyper-coagulable states (such as cancer), preexisting renal dysfunction, or prior renal vein thrombosis. If the patient has a solitary functioning kidney, then a suprarenal filter is not appropriate.

21
Other Complications Guidewire entrapment in the filter These may be impossible to remove and may require repeat endovascular or open procedures for retrieval. Mechanical problems with the filter can include strut fracture Infection is an extremely rare event with IVC filters

24
A rare complication Snare-Filter entrapment as a rare complication during Celect inferior vena cava filter retrieval Snare-Filter entrapment as a rare complication during Celect inferior vena cava filter retrieval A 45 year-old female patient presented with bilateral extensive ileofemoral DVT A 45 year-old female patient presented with bilateral extensive ileofemoral DVT Patient was started on anticoagulant treatment Patient was started on anticoagulant treatment

25
The patient developed headache and left sided weakness. A Head CT scan was done and revealed right intracranial hemorrhage The patient developed headache and left sided weakness. A Head CT scan was done and revealed right intracranial hemorrhage Anticoagulant therapy stopped»»» IVCF placement Anticoagulant therapy stopped»»» IVCF placement

26
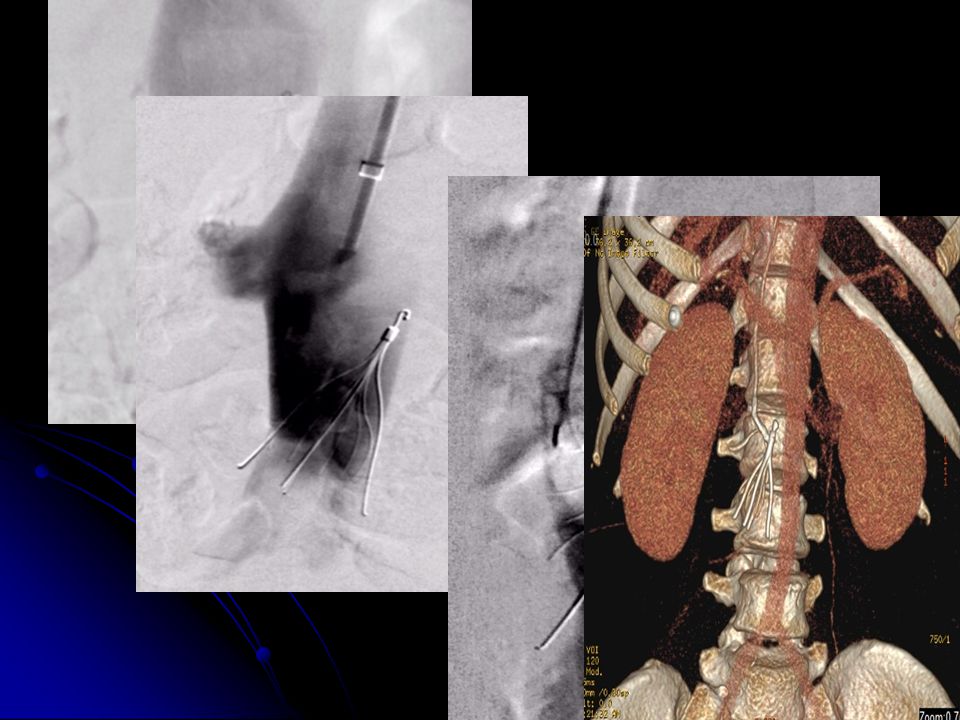
Two months later, in the absence of any indication to retain the rIVCF, the patient was referred to the interventional radiology unit for filter retrieval. Two months later, in the absence of any indication to retain the rIVCF, the patient was referred to the interventional radiology unit for filter retrieval. Cavogram showed that the filter had tilted which caused the hook to become embedded in the left side of IVC wall and penetration of one of the major struts of the filter through the right side of IVC wall. Cavogram showed that the filter had tilted which caused the hook to become embedded in the left side of IVC wall and penetration of one of the major struts of the filter through the right side of IVC wall.

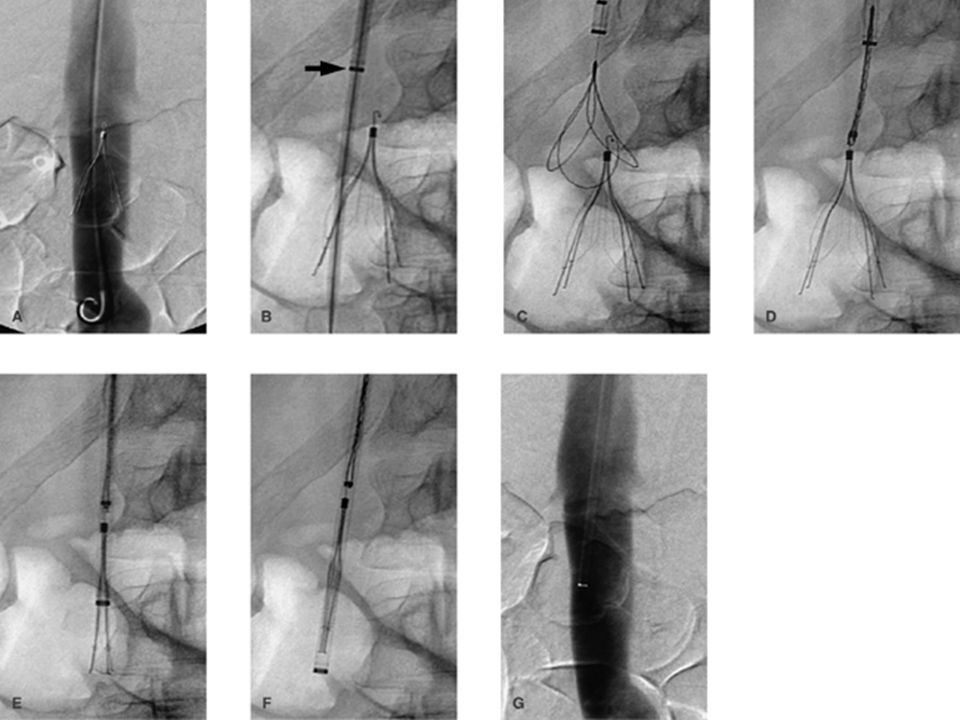
27
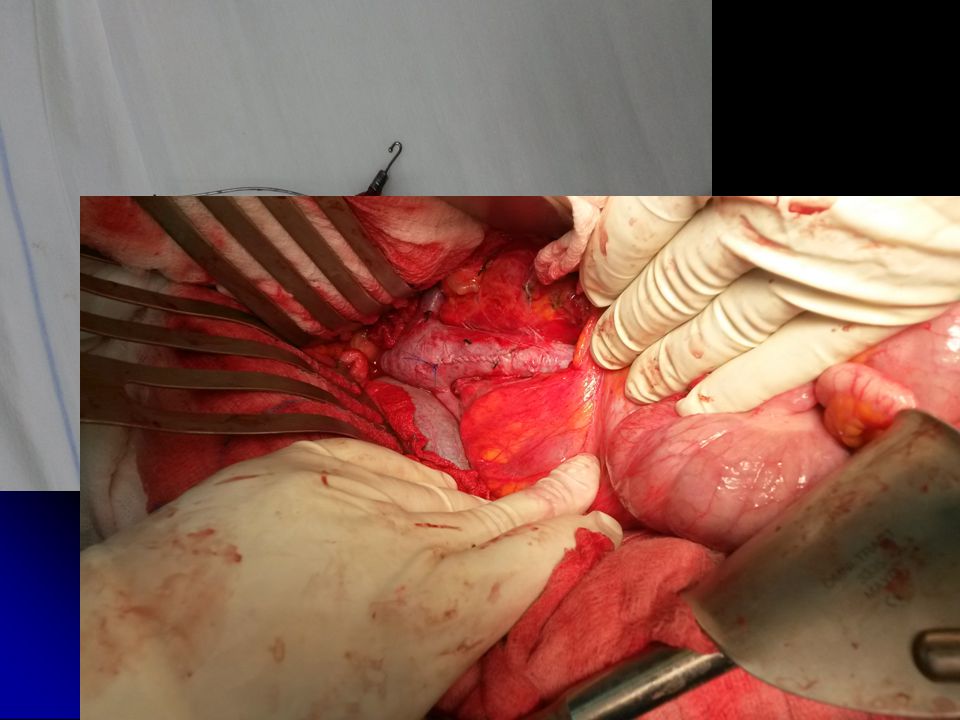
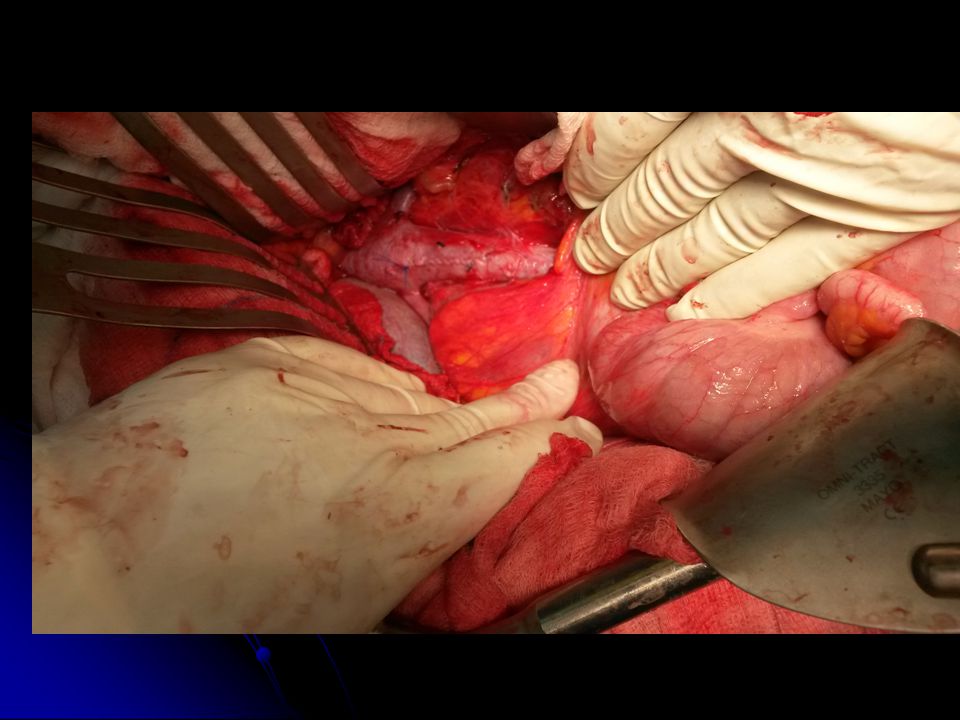
The standard filter retrieval technique was performed using Gunther Tulip Vena Cava Filter Retrieval Set (Cook, Bloomington, IN) The standard filter retrieval technique was performed using Gunther Tulip Vena Cava Filter Retrieval Set (Cook, Bloomington, IN) After several retrieval attempts by standard techniques, the snare over guidewire loop technique was attempted which was complicated by entrapment of the snare with two of the minor struts of the filter with subsequent failure of dis- engagement. After several retrieval attempts by standard techniques, the snare over guidewire loop technique was attempted which was complicated by entrapment of the snare with two of the minor struts of the filter with subsequent failure of dis- engagement.

33
THANK YOU

Similar presentations










 ASDIN Coding University 1.>")





>")






