Download presentation
Presentation is loading. Please wait.

1
Wound Care Suzana Tsao, DO

2
Why do we care?

3
Layers of the Skin Closure at the dermal level
Subcutaneous adds little strength Complex wounds in/below fascial layer need multi-layer closure

4
Healing Initially edges retract and tissue contracts
Platelet aggregation and clotting cascade activated Initial epithelialization h Peak collagen synthesis 5-7d Strength of wound 5% at 2 weeks 35% at one month

5
Initial Evaluation Always start with the ABCD’s Airway Breathing
Circulation Disability

6
Wound Evaluation Location Active bleeding Exposed tissue/bone/organs
Check for peripheral pulses

7
History Where When How Location, location, location Golden period
Mechanism Potential for foreign body

8
Where Anatomic location Special Consideration Mouth Ear Joints
periorbital Head injuries bleed less chance of infection Hand and feet more prone to infection

9
When Golden Hour of Wounds Infectious inoculum 105 per gram
Need 3-5 hours for proliferation of bacteria Extremities 6 hours Face and scalp 24 hours But wait ….

10
When to close Studies show can close as late as 19 hours on extremities ACEP clinical policy supports 8-12 hours Depends on the clinical scenario Consider other types of closure Primary closure Delayed primary closure Healing by secondary intention

11
How Mechanism Assess concern for foreign body Clean wound Dirty wound
Contaminated wound

12
High Risk Mechanisms Open fractures Intraoral wounds Mamillian bites
Crush injuries/devascularized tissue High pressure injuries Jagged edges/stellate shape/deeper than subcutaneous layer Foreign body Visible contamination Mamillian bites have 6% risk of infection

13
PMH/SocHx Co-Morbid Conditions Hand dominance Occupation
Last tetanus booster

14
Tetanus < 3 doses in primary series Primary 3 series completed
Clean/minor Tetanus toxoid All other Toxoid and immunoglobulin Primary 3 series completed < 5 years None needed > 5 years but < 10 years Clean minor All others Give toxoid > 10 years

15
Pertussis Give Tdap regardless of last Td to update pertussis if not updated as an adult Replaces one of the 10 year Td booster doses Boostrix when feasible for > 65 y/o Tdap during each pregnancy b/w 27 and 36 weeks CDC link summary.htm

16
Co-Morbid Conditions Age (very young/very old) Diabetes Renal Failure
Malnutrition Obesity Immunocompromised

17
Physical Exam Type of wound Superficial/deep Length/shape
Bleeding/revascularization Associated injuries Retained foreign body Complete neurovascular exam 2 point discrimination most accurate for sensory function in extremities

18
Active Bleeding Direct pressure BP cuff 2 hours max Figure of 8 stitch

19
Associated Injuries Assess for tendon injuries
90% lacerated tendon can still maintain normal neuro function Assess for joint involvement May need to inject joint Assess for underlying fracture X-ray if suspected before manipulating the area

20
Retained Foreign Body Direct visualization X-ray Ultrasound CT/MRI?
May need anesthesia to fully evaluate X-ray 80-90% can be detected Does not visualize organic material Ultrasound CT/MRI? RFB 5th leading cause of malpractice claims against em physicians

21
Indications for FB removal
Reactive materials Wood Vegetative material Contaminated materials Clothes Most fb in foot Impingement on neurovascular structures Impairment of function Easy to remove

22
Indications for consultation
Nerve injury Vascular injury Tendon or joint involvement Difficult to remove foreign body High pressure injection injury

23
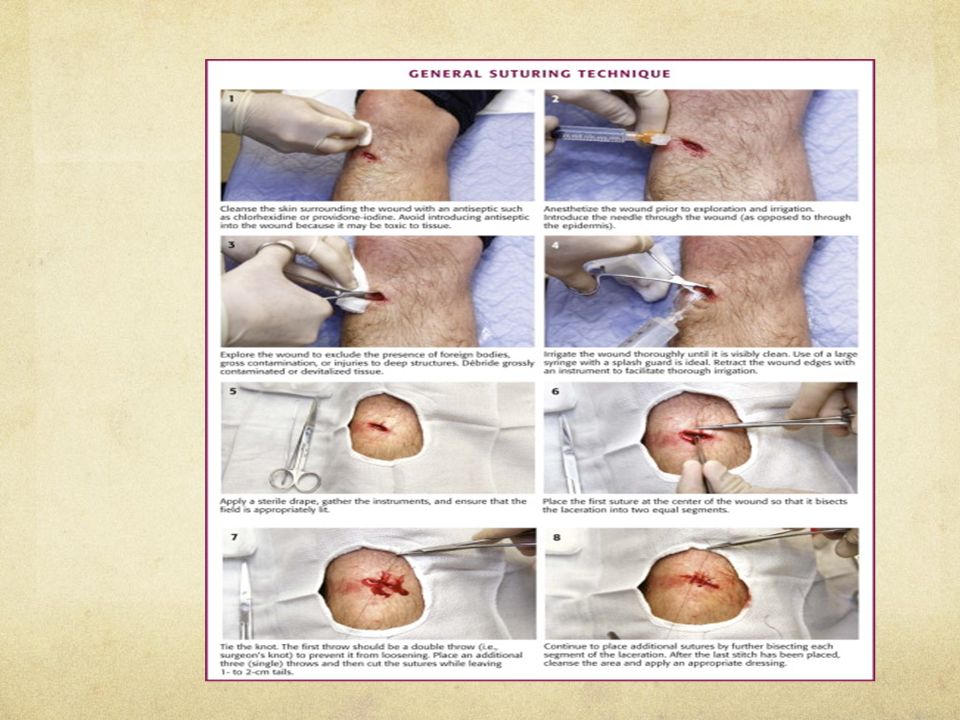
Irrigation Dilution is the solution to the pollution Amount
High pressure (5-8 psi) 30-60 cc syringe with 19 gauge angiocath or splash shield Amount Min 250ml 50-100ml/cm of laceration Type of fluid Tap water just as good as normal saline NEVER, EVER, NEVER Betadine or peroxide 1% Betadine may be ok, but no increased benefit
 cc syringe with 19 gauge angiocath or splash shield. Amount. Min 250ml ml/cm of laceration. Type of fluid. Tap water just as good as normal saline. NEVER, EVER, NEVER. Betadine or peroxide. 1% Betadine may be ok, but no increased benefit.")
25
Debridement Remove necrotic tissue
May need to debride for better approximation and cosmetic results

26
Sterile Gloves Several trials showed no difference if final outcome
Dealer’s choice

27
Anesthesia Topical pretreatment Consider procedural sedation Allergies
Most are from preservative Consider using cardiac lidocaine 1% Benadryl

28
Local vs. Regional Block
Large areas When needed to avoid tissue distortion Areas where infiltration is painful Plantar surface of foot

29
Anesthesia Amides Esters Lidocaine Procaine Lidocaine with epinephrine
Max 4.5mg/kg Duration 1-2 h Lidocaine with epinephrine Max 7mg/kg Duration 2-4 h No epi in fingers/toes, ear, nose, penis Bupivacaine Max 2mg/kg 0.25% Duration 4-8 h Esters Procaine Max 7mg/kg Duration min

30
Types of Repair Primary closure Delayed primary closure
Closure of the wound at the time of the ED visit Delayed primary closure Closure of wound 3-4 days after injury Healing by secondary intention Allow wound to heal without closure through scarring

31
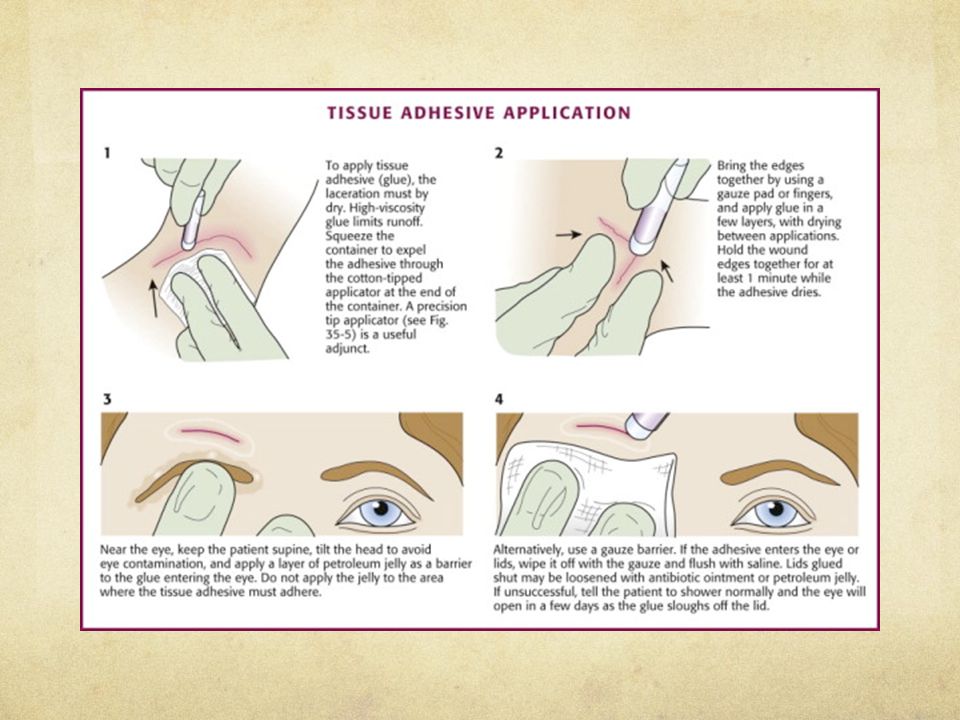
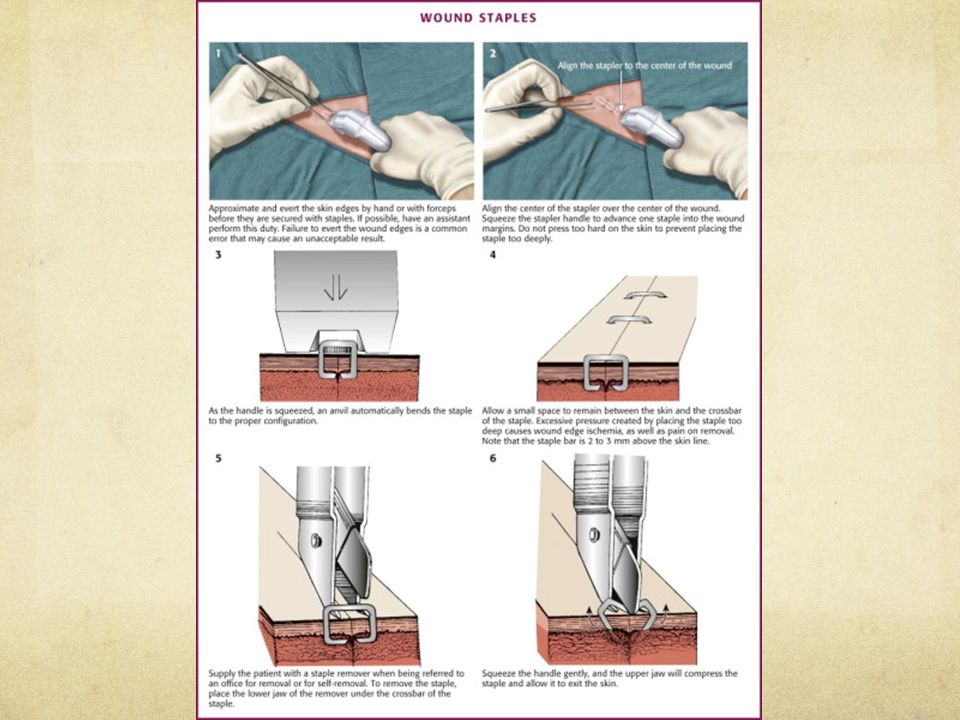
Methods of Closure Tape Skin Adhesives Staples Sutures
Superficial, straight, under little tension Skin Adhesives Does not involve deep layers Little tension Staples Linear on trunk, extremities, scalp Sutures

35
Types of Sutures Absorbable Nonabsorbable Gut PDS (polypropylene)
Maxon (polyglyconate) Dexon (polyglycolic acid) Coated Vicryl (polyglactin) Nonabsorbable Dermalon or ethilon Prolene or surgilene (polypropylene) Silk steel
 Dexon (polyglycolic acid) Coated Vicryl (polyglactin) Nonabsorbable. Dermalon or ethilon. Prolene or surgilene (polypropylene) Silk. steel.")
37
Suture size by location
Face 5-0 to 6-0 Scalp/Chest/Back/Abdomen 3-0 to 5-0 Extremities 4-0 to 5-0 Oral 3-0 to 5-0 (absorbable)
")
38
Indications for antibiotics
Prosthetic device Endocarditis prophylaxis Open joints and/or fractures Mamillian bites Intraoral lesions Immunocompromised patients Heavily contaminated wounds

39
Discharge instructions
Signs and symptoms of infection Fever, discharge, red lines from wound, erythema, swelling Elevation +/- splinting When to do wound checks at one or two days Suture removal instructions Face 3-5 days Scalp 5 days Extremities 7-10 days, high tension days Washing - showering - avoid long baths, pools, ocean Triple antibiotic ointment

40
Pearls No such thing as absolute golden hour
Tap water is as good and normal saline Do not soak in betadine Nonsterile gloves ok Hand wounds less than 2cm -> big, bulky dressing as good as sutures

41
Pitfalls Always remember ABC’s Look for associated injuries
Bone, vascular, nerve Don’t dismiss high pressure injuries Always assess for foreign body Antibiotics vs. delayed primary closure for high risk wound and/or co-morbid conditions Remember special locations Ear, nose, vermillion border Fight bites do not close

Similar presentations



 jeopardizes the ability to walk.>")
















