Download presentation
Presentation is loading. Please wait.

1
Gynecologic malignancies
Kocsis Judit

2
Cancer Statistics – 2010 Estimated New Cases Estimated Deaths
28% Breast 14% Lung and bronchus 10% Colon and rectum 6% Uterine corpus 5% Thyroid 4% Non-Hodgkin lymphoma 4% Melanoma 3% Kidney 3% Ovary 3% Pancreas 207,090 26% Lung and bronchus 15% Breast 9% Colon and rectum 7% Pancreas 5% Ovary 4% Non-Hodgkin lymphoma 3% Leukemia 3% Uterine corpus 2% Liver 2% Brain 39,840 43,470 13,850 7,950 21,880 Jemal, A. et al. CA Cancer J Clin 2010; 60:

3
Estimated New Gynecologic Cancers: 2010
Uterus 43,470 Vulva 3,900 Ovary 21,880 Vagina & Other 2,300 Cervix 12,200 Jemal, A. et al. CA Cancer J Clin 2010; 60:

5
GENERAL OVERVIEW OF GYNECOLOGIC CANCERS
79,480 new cases/yr of female genital system cancers in the U.S. 28,910 deaths in U.S. from genital system cancers in 2005 Diet, exercise and lifestyle choices play important roles in the prevention of cancer Knowledge of family history also increases prevention and early diagnosis rates Regular screening and self-examinations for appropriate cancers early detection early intervention & therapy

6
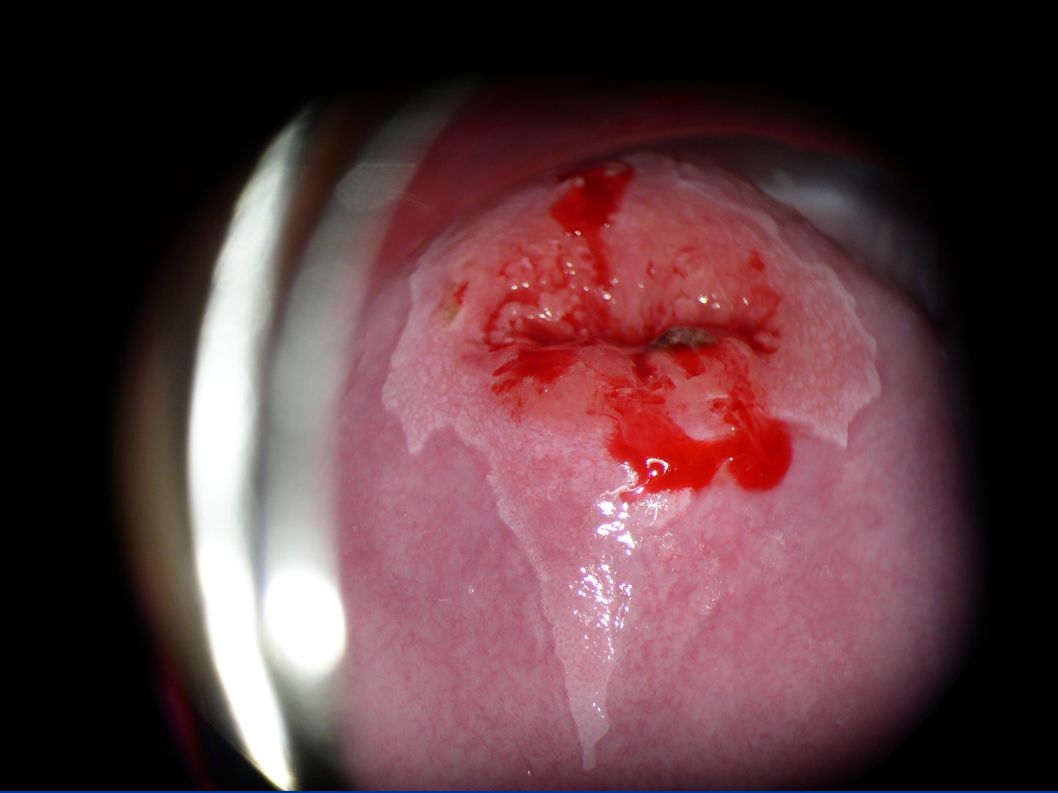
Cervical cancer

7
Cervical Cancer Year Cases Deaths % 2006 9,710 3,700 38 2007 11,150
3,670 33 2008 11,070 3,870 35 2009 11,270 4,070 36 2010 12,200 4,210 Jemal A, et al. CA Cancer J Clin

8
Distribution of Patients
Cervical Carcinoma Stage Distribution of Patients Five-year Survival I 62% 85% II 18% 60% III 11% 35%

9
At risk groups Young (immature TZ)
Early age of first sexual intercourse Multiple partners Smoking Type of contraception Screening history

11
Treatment modalities Surgery Radiotherapy Chemotherapy Radiochemotherapy

12
Treatment Depends on stage of disease
Surgery in early stage Cone biopsy Radical trachylectomy Radical hysterectomy (Wertheim 1898) Exenteration (Brunschwig)
 Exenteration (Brunschwig)")
13
Surgery Wertheim operation
first in 1898 radical hysterectomy today standard procedure in operable cervix cancer (with bilateral pelvic lymphadenectomy) Organ sparing technics (tachylectomy, radical trachylectomy) in young patients, early stage
 Organ sparing technics (tachylectomy, radical trachylectomy) in young patients, early stage.")
14
Chemotherapy Radiotherapy
Chemo-radiation as a primary treatment In stage IB2-IVA-- Neoadjuvant chemotherapy combined with radical surgery- best overall survival Radiotherapy as post operative treatment for poor prognostic disease Chemotherapy or radiotherapy for palliation

15
Chemotherapy for Advanced or Recurrent Cervical Cancer
Combination chemotherapy GOG 76X; Cisplatin + paclitaxel, 46% RR (Rose et al, 1999) GOG 169; cisplatin + paclitaxel vs cisplatin; improved RR not OS (Moore et al 2004) GOG 179; topotecan + cisplatin; improved OS (Long et al, 2005) GOG 204; topotecan, gemcitabine, vinorelbine, paclitaxel Interim analysis: so sig benefit; RR, PFS and OS favors cisplatin + paclitaxel (Monk et al, 2009) Favored regimen: cisplatin + paclitaxel Role of carboplatin + paclitaxel?
 GOG 169; cisplatin + paclitaxel vs cisplatin; improved RR not OS (Moore et al 2004) GOG 179; topotecan + cisplatin; improved OS (Long et al, 2005) GOG 204; topotecan, gemcitabine, vinorelbine, paclitaxel. Interim analysis: so sig benefit; RR, PFS and OS favors cisplatin + paclitaxel (Monk et al, 2009) Favored regimen: cisplatin + paclitaxel. Role of carboplatin + paclitaxel")
16
Cervical cancer Milestones
Surgery vs radiotherapy in early CC NCI consensus statement in 1999 on the role of concurrent chemotherapy and radiation The importance of Hb-level during radiation therapy for CC The potential of hyperthermia

17
Cervical cancer and pregnancy
0,02-0,9% (real: 0,5-5%) Obligatory screening at first pregnancy FU Therapy: Conisation from 2. trimester Treatment time and type of surgery depends on tumor stage and trimester! trimester : maternal life is the priority 3. trimester: foetal life is priority
 Obligatory screening at first pregnancy FU. Therapy: Conisation from 2. trimester. Treatment time and type of surgery depends on tumor stage and trimester! trimester : maternal life is the priority. 3. trimester: foetal life is priority.")
18
Endometrial cancer

19
ENDOMETRIAL CANCER Tumor of the endometrial layer of uterus
Most common gynecologic cc. 40,000 new case/year 7,000 death/year 4. most common female cc. (US) 2. most commmon female cc. (UK) 5. most common female cc.(worldwide) West developed > South East Asia 1970s increase Due to HRT (estrogen) Histology: adenocarcinoma These are the statistics for the US population 19
 2. most commmon female cc. (UK) 5. most common female cc.(worldwide) West developed > South East Asia. 1970s increase. Due to HRT (estrogen) Histology: adenocarcinoma. These are the statistics for the US population. 19.")
20
Uterine Neoplasia Hyperplasia Adenocarcinoma Sarcoma Sporadic
Inherited Lynch syndrome (HNPCC) Cowden’s disease BRCA syndrome? Type I Type II Estrogen-dependent Endometrioid MMR/MSI PTEN, KRAS Estrogen-independent Serous, clear cell TP53, HER-2/neu, p16
 Cowden’s disease. BRCA syndrome Type I. Type II. Estrogen-dependent. Endometrioid. MMR/MSI. PTEN, KRAS. Estrogen-independent. Serous, clear cell. TP53, HER-2/neu, p16.")
21
RISK FACTORS FOR ENDOMETRIAL CANCER
Early menarche (<age 12) Late menopause (>age 52) Infertility or nulliparous Obesity Treatment with tamoxifen for breast cancer Estrogen replacement therapy (ERT) after menopause Diet high in animal fat Diabetes Age greater than 40 Caucasian women Family history of endometrial cancer or hereditary nonpolyposis colon cancer (HNPCC) Personal history of breast or ovarian cancer Prior radiation therapy for pelvic cancer
 Late menopause (>age 52) Infertility or nulliparous. Obesity. Treatment with tamoxifen for breast cancer. Estrogen replacement therapy (ERT) after menopause. Diet high in animal fat. Diabetes. Age greater than 40. Caucasian women. Family history of endometrial cancer or hereditary nonpolyposis colon cancer (HNPCC) Personal history of breast or ovarian cancer. Prior radiation therapy for pelvic cancer.")
22
Protective factors Oral Contraceptives Tobacco Smoking
Combined OC => 50% reduced rate Actual reduction number small because uncommon in women of child bearing age Long term offers protection Reduced risk presumably => progesterone Tobacco Smoking Some evidence that it reduces the rate Smokers have lower levels of estrogen and lower rate of obesity

23
Adipose tissue: Consequences of Obesity on Cancer Development
Obesity has been implicated in the development of Type 2 diabetes Heart disease Stroke Hypertension Gallbladder disease Osteoarthritis Sleep apnea Asthma Psychological disorders or difficulties Some cancers, including ovarian, cervical, breast, and endometrial Dyslipidemia Complications of pregnancy Hirsuitism Menstrual abnormalities Stress incontinence Increased surgical risk

24
Endometrial Cancer and Lifestyle
24

25
Important Definitions
Obesity: having a very high amount of body fat in relation to lean body mass, or Body Mass Index (BMI) of 30 or higher for adults. Body Mass Index (BMI): a measure of weight in relation to height, specifically weight in kilograms divided by the square of his or her height in meters. Morbid Obesity-100 pounds above ideal weight or BMI over 40 (indication for bariatric surgery) Bariatric surgery is the term for operations to help promote weight loss.
 of 30 or higher for adults. Body Mass Index (BMI): a measure of weight in relation to height, specifically weight in kilograms divided by the square of his or her height in meters. Morbid Obesity-100 pounds above ideal weight or BMI over 40 (indication for bariatric surgery) Bariatric surgery is the term for operations to help promote weight loss.")
26
Endometrial Carcinoma
Etiology Unnoposed estrogen hypothesis: exposure to unopposed estrogens Pathology Spreads through uterus, fallopian tubes, ovaries and out into peritoneal cavity Metastasizes via blood and lymphatic system Unopposed estrogen hypothesis is the theoretical framework used to explain the relationship between endogenous steroid hormones and endometrial cancer risk. This hypothesis proposes that that endometrial cancer may develop as a result of the mitogenic effects of estrogens, when these are insufficiently counterbalanced by progesterone. In etiological terms, any factor that increases exposure to unopposed estrogens (such as estrogen therapy obesity, and irregular menstrual cycles) tends to increase the risk of the disease, while factors that decrease exposure to estrogens or increase progesterone levels (such as oral contraceptives or smoking) tend to be protective. 26
 tends to increase the risk of the disease, while factors that decrease exposure to estrogens or increase progesterone levels (such as oral contraceptives or smoking) tend to be protective. 26.")
27
SYMPTOMS OF ENDOMETRIAL CANCER
Non-menstrual bleeding or discharge Especially post-menopausal bleeding Heavy bleeding Dysuria Pain during intercourse Pain and/or mass in pelvic area Weight loss Back pain

28
ENDOMETRIAL CANCER Treatment Diagnosis Surgery-standard th
Pelvic examination Pap smear (detect cancer spread to cervix) Endometrial biopsy Dilation and curettage Transvaginal ultrasound Treatment Surgery-standard th Hysterectomy Salpingo-oophorectomy Pelvic lymph node dissection Laparoscopic lymph node sampling Radiation therapy Chemotherapy Hormone therapy Progesterone Tamoxifen
 Endometrial biopsy. Dilation and curettage. Transvaginal ultrasound. Treatment. Surgery-standard th. Hysterectomy. Salpingo-oophorectomy. Pelvic lymph node dissection. Laparoscopic lymph node sampling. Radiation therapy. Chemotherapy. Hormone therapy. Progesterone. Tamoxifen.")
29
Adjuvant Treatment Summary
Low Risk Inter-mediate Risk High Risk Stage/ Grade IA G1/2 IA (G3) IB (all grades) IIA IIB Stage III Stage IV UPSC (all stages) CCC (all stages) Undiff (all stages) Post-operative (complete surgical staging) None Vaginal Cuff Brachy Therapy or Observation (*exception is in stage IIB) Chemotherapy consider RT (Vaginal Cuff Brachy Therapy vs. whole pelvic)
 IB (all grades) IIA. IIB. Stage III. Stage IV. UPSC (all stages) CCC (all stages) Undiff (all stages) Post-operative. (complete. surgical. staging) None. Vaginal Cuff Brachy Therapy or Observation. (*exception is in stage IIB) Chemotherapy consider RT (Vaginal Cuff Brachy Therapy vs. whole pelvic)")
30
Ovarian cancer

31
Risk Factors Family history (primarily 2 or more first degree relatives) Age (besides family history, this is the most important risk factor) Nulliparity Early menarche, late menopause Late childbirth (age <35) Environmental factors not yet defined
 Environmental factors not yet defined.")
32
Risk Reduction OCP’s Breast Feeding Tubal ligation
Several Case-controlled studies have documented that OCP users have a 30-60% smaller chance of developing EOC than non-users WHO study documented a RR 0.75 Greater reduction in risk with nulliparous women and increased duration of use Breast Feeding Tubal ligation Risk reducing oophorectomy

33
Hereditary Ovarian Cancer
Account for 10% of EOC BRCA1, BRCA2 (Hereditary Breast and Ovarian Cancer –HBOC) Estimated 1/300 to 1/800 individuals carry a BRCA 1 or 2 mutation Estimated 1/40 Ashkenazi Jews carry a BRCA 1 or 2 mutation Hereditary Nonpolyposis Colorectal Cancer (HNPCC), Lynch II Colorectal Cancer before age 50 Endometrial cancer before age 50 2 or more “Lynch” family members: colorectal, endometrial, ovarian, ureter/renal pelvis, gastric, biliary tract, small bowel, pancreatic, brain and sebaceous adenoma
 Estimated 1/300 to 1/800 individuals carry a BRCA 1 or 2 mutation. Estimated 1/40 Ashkenazi Jews carry a BRCA 1 or 2 mutation. Hereditary Nonpolyposis Colorectal Cancer (HNPCC), Lynch II. Colorectal Cancer before age 50. Endometrial cancer before age or more Lynch family members: colorectal, endometrial, ovarian, ureter/renal pelvis, gastric, biliary tract, small bowel, pancreatic, brain and sebaceous adenoma.")
34
Hereditary Ovarian Cancer
Risk relative to family history Overall risk (OR) for women with a single first degree relative is 3.1 (5% lifetime risk) OR with 2 or 3 relatives is 4.6 (7.2% lifetime risk)
 for women with a single first degree relative is 3.1 (5% lifetime risk) OR with 2 or 3 relatives is 4.6 (7.2% lifetime risk)")
35
Hereditary Ovarian Cancer
BRCA 1 Germline Mutations Tumor suppressor gene on 17q21 (long arm) Autosomal dominant 65 to 74% Breast Cancer risk 39-46% Ovarian Cancer risk For women with Breast Cancer, the 10-year actuarial risk of developing Ovarian Cancer is 12% Predominately high grade, serous or endometrioid adenocarcinoma ACOG Practice Bulletin #103, 2009.
 Autosomal dominant. 65 to 74% Breast Cancer risk % Ovarian Cancer risk. For women with Breast Cancer, the 10-year actuarial risk of developing Ovarian Cancer is 12% Predominately high grade, serous or endometrioid adenocarcinoma. ACOG Practice Bulletin #103,")
36
Hereditary Ovarian Cancer
BRCA2 Germline Mutations Tumor suppressor gene on chromosome 13q12 65-74% Breast Cancer risk 12-20% Ovary Cancer risk For women with Breast Cancer the 10-year actuarial risk of developing Ovarian Cancer is 6% Predominately high grade, serous or endometrioid adenocarcinoma

37
Lancaster et al. Gynecol Oncol 2007; 107: 159-62.
Genetic Counseling Patients with a >20-25% chance of having an inherited predisposition to breast or ovarian cancer and for whom genetic risk assessment is recommended Women with a personal history of both breast and ovarian cancer Women with ovarian cancer and a close relative with breast cancer at ≤50 or ovarian cancer at any age Women with ovarian cancer at any age who are an Ashkenazi Jew Women with breast cancer at ≤50 and a close relative with ovarian cancer or a male breast cancer Women who are an Ashkenazi Jew and breast cancer ≤40 Women with a 1st or 2nd degree relative with a BRCA 1 or 2 mutation Lancaster et al. Gynecol Oncol 2007; 107:

38
Lancaster et al. Gynecol Oncol 2007; 107: 159-62.
Genetic Counseling Patients with a >5-10% chance of having an inherited predisposition to breast or ovarian cancer and for whom genetic risk assessment may be helpful Women with breast cancer at ≤40 Women with bilateral breast cancer (particularly if breast cancer was at ≤50 years) Women of Ashkenazi Jewish ancestry with breast cancer at ≤50 years Women with breast or ovarian cancer at any age with two or more close relatives with breast cancer at any age (particularly if at least 1 breast cancer was at ≤50 years) Unaffected women with a 1st or 2nd degree relative that meets one of the above criteria Lancaster et al. Gynecol Oncol 2007; 107:
 Women of Ashkenazi Jewish ancestry with breast cancer at ≤50 years. Women with breast or ovarian cancer at any age with two or more close relatives with breast cancer at any age (particularly if at least 1 breast cancer was at ≤50 years) Unaffected women with a 1st or 2nd degree relative that meets one of the above criteria. Lancaster et al. Gynecol Oncol 2007; 107:")
39
Hereditary Ovarian Cancer
HNPCC Autosomal dominant 80% risk of developing colon cancer 60% risk of developing endometrial cancer 10-15% risk of developing ovarian cancer Mismatch repair gene defects MSH2, MSH6, PMS2 and MLH1 (chromosome 3)
")
40
Risk-reducing Salpingo-oophorectomy (RRSO)
Estimated 1000 cases of ovarian cancer could be prevented if elective SO was performed in all women undergoing hysterectomy at 40 years or older 5-10% of women with ovarian cancer have had a previous hysterectomy at age 40 or older Obtain a family history for BRCA and HNPCC ACOG Practice Bulletin #89, 2008

41
Screening for Ovarian Cancer
There is no evidence that screening for Ovarian Cancer leads to earlier detection or improved survival… Nonetheless, the following have been or are being used TVS CA125 Multimodal Symptoms Biomarkers

42
EOC

43
Histology Histology Incidence Serous (high and low grade) 40-50%
Most common Endometrioid 15-25% 2nd most common Mucinous 6-16% Clear Cell 5-11% Other

44
Symptoms of Ovarian Cancer
Largely non-specific Increase in abdominal girth (ascites) Bloating Fatigue Abdominal pain Early satiety Indigestion Constipation Weight loss, unexplained New onset of urinary frequency or incontinence
 Bloating. Fatigue. Abdominal pain. Early satiety. Indigestion. Constipation. Weight loss, unexplained. New onset of urinary frequency or incontinence.")
45
FIGO Staging Stage I IA Tumor confined to a single ovary, negative washings, capsule intact, surface of ovary uninvolved IB Tumor found in both ovaries, negative washings, capsule intact, surface of ovary uninvolved IC Tumor on one or both ovaries, ruptured capsule, positive cytology or ovarian surface involvement Stage II IIA Extension or metastasis to uterus and/or tubes IIB Extension to other pelvic structures IIC Tumor on one or both ovaries, ruptured capsule, positive cytology or ovarian surface involvement Stage III IIIA Tumor on one or both ovaries with microscopic spread to abdominal peritoneal surface (ex. Liver serosa) IIIB Tumor implant <2cm to abdominal peritoneal surface IIIC Tumor implant >2cm to abdominal peritoneal surface and/or positive retroperitoneal or inguinal lymph nodes Stage IV Distant metastasis Pleural effusion with positive cytology Parenchymal liver metastasis
 IIIB Tumor implant <2cm to abdominal peritoneal surface. IIIC Tumor implant >2cm to abdominal peritoneal surface and/or positive retroperitoneal or inguinal lymph nodes. Stage IV. Distant metastasis. Pleural effusion with positive cytology. Parenchymal liver metastasis.")
46
5-year Survival Rates Stage I 76-93% Stage II 60-74% Stage III
IIIA 41% IIIB 25% IIIC 20% Stage IV 11%

47
Principles of Ovarian Cancer Surgery
Purpose of Surgery Staging of disease Prognosis and treatment depend upon surgical findings and subsequent stage Debulking (cytoreduction) Overall reduction of tumor burden to less than 1 cm (preferably no gross residual disease) improves survival Palliation of symptoms Goldie-Coldman Hypothesis Resistance to chemotherapy will develop in fraction of remaining viable cells
 Overall reduction of tumor burden to less than 1 cm (preferably no gross residual disease) improves survival. Palliation of symptoms. Goldie-Coldman Hypothesis. Resistance to chemotherapy will develop in fraction of remaining viable cells.")
48
Primary Debulking Aggressive surgical procedures
Multiple or extensive bowel resection Rectosigmoid resection Resection of ureteral/bladder segment Diaphragm stripping Resection of liver, spleen, kidney, diaphragm

49
Primary Debulking optimal primary debulking (residual disease <1 cm) is an independent prognostic factor Even in patients with unresectable liver metastasis, optimal debulking of extrahepatic disease is associated with a significant survival advantage

50
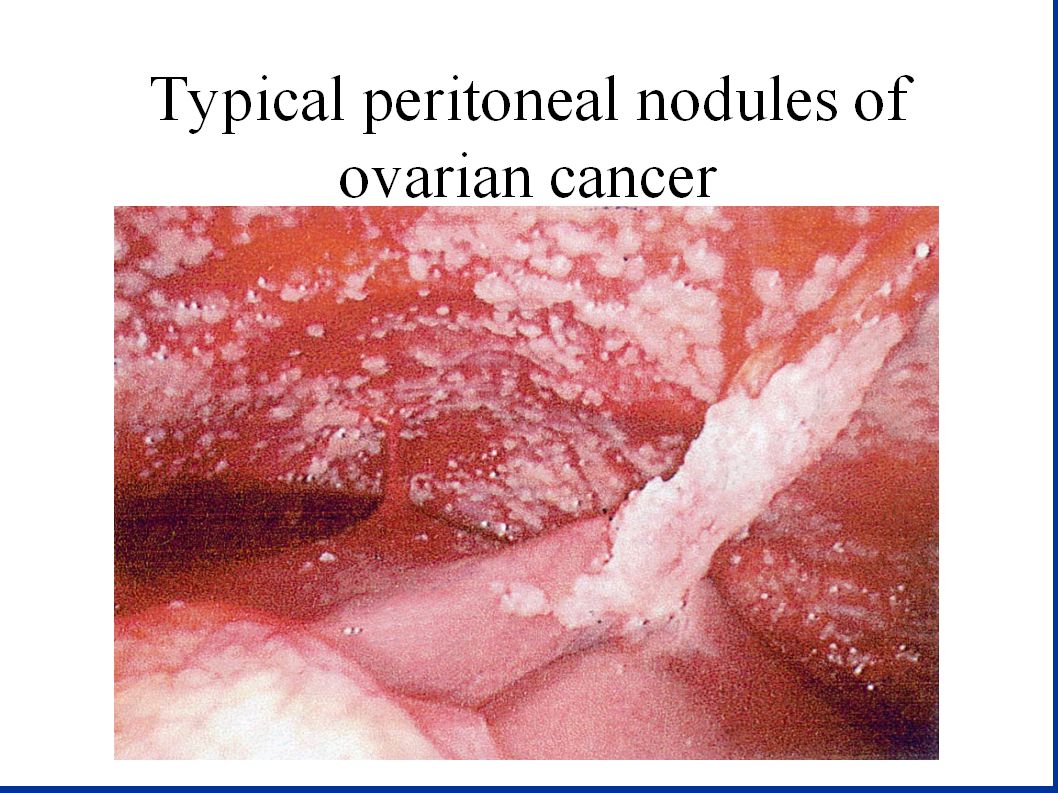
Patterns of spread Direct extension Exfoliation of clonogenic cells
Lymphatic spread

51
Assessment of extent of disease Optimal tumor reduction
Ovarian Cancer Surgical Debulking and Staging Exploration Biopsies (Staging) TAH/ BSO Goals (Debulking) Assessment of extent of disease Optimal tumor reduction Washings/ Ascites (Staging) TAH = total abdominal hysterectomy BSO = bilateral salphingo-oophorectomy 51
 TAH/ BSO. Goals (Debulking) Assessment of extent of disease. Optimal tumor reduction. Washings/ Ascites. (Staging) TAH = total abdominal hysterectomy. BSO = bilateral salphingo-oophorectomy. 51.")
52
First-line Therapy – Standard Treatment Options
Surgery with maximum cytoreduction effort <1cm residual disease Surgery is usually the first step in the care of patients. Every effort should be made to leave behind minimal residual disease. Most patients with ovarian cancer will receive chemotherapy as part of their primary treatment. Drugs: carboplatin (Paraplatin®) paclitaxel (Onxol®, Taxol®) Platinum + Taxane Chemotherapy (Carboplatin + Paclitaxel) 52
 paclitaxel (Onxol®, Taxol®) Platinum + Taxane Chemotherapy (Carboplatin + Paclitaxel) 52.")
53
Systemic therapy for EOC
Highly chemosensitive tumor (esp. histology subtype: high grade serosus, endometrioid) Basic drugs: platinum compounds with paclitaxel First line therapy: carboplatin + TAX New biologic therapy: bevacizumab (addition of bev. to standard KT and maintance bevacizumab prolongs PFS) Relapse: platina reinduction (in platinum sensitive cases, >12 month DFS) or second line treatment with other agents (topothecan, L-ADM, gemcitabine, weekly TAX, etoposid, cyclophosphamid) or clinical trial
 Basic drugs: platinum compounds with paclitaxel. First line therapy: carboplatin + TAX. New biologic therapy: bevacizumab (addition of bev. to standard KT and maintance bevacizumab prolongs PFS) Relapse: platina reinduction (in platinum sensitive cases, >12 month DFS) or second line treatment with other agents (topothecan, L-ADM, gemcitabine, weekly TAX, etoposid, cyclophosphamid) or clinical trial.")
55
Secondary Cytoreduction
Kidney Resected Liver Diaphragm Vena Cava Tumor Mass Renal Vein Secondary Cytoreduction Controversial Inconsistent definitions Benefit appears confined to patients likely to respond to additional chemo: >12 month PFI Isolated site of recurrence Disease completely resectable PFI = progression-free interval 55 55

56
History of Intraperitoneal Chemotherapy Ovarian Cancer
1970’s : IPCT used for its cytotoxic properties High concentrations, large volumes 1978 : Landmark paper by Dedrick et al. A sound pharmacokinetic rationale for IPCT 1991 : IP therapy: time’s up (Ozols) Time’s not up (Muggia, Alberts) 1996 : Survival benefit for IPCT (Alberts et al.) 2004 : IPCT not widely adopted (GCIG OCCC) 2006 : NCI Clinical Announcement / Survival benefit with IP therapy
 Time’s not up (Muggia, Alberts) 1996 : Survival benefit for IPCT (Alberts et al.) 2004 : IPCT not widely adopted (GCIG OCCC) 2006 : NCI Clinical Announcement / Survival benefit with IP therapy.")
57
How to improve outcome? Better screening (OVA test etc?) Surgical treatment in selected centers by well trained gynecologyc oncologist Better systemic therapy: addition of biologic agents to KT, weekly TAX protocolls, intraperitoneal chemotherapy
 Surgical treatment in selected centers by well trained gynecologyc oncologist Better systemic therapy: addition of biologic agents to KT, weekly TAX protocolls, intraperitoneal chemotherapy")
58
Potential targets in the future
Angiogenesis PARP inhibitors Folate receptor antagonists PI3kinase inhibition RAS/RAF Etc.

59
IPCT vs IVCT in Advanced Ovarian Cancer Overall survival
Investigators No. of Overall survival (mo) year published pts Control arm Exp. Arm Alberts et al, Polyzos et al, Gadducci et al, Markman et al, Yen et al, Armstrong et al, 1 p = 0.02; 2 p = 0.05; 3 p = 0.03
 year published pts Control arm Exp. Arm. Alberts et al, Polyzos et al, Gadducci et al, Markman et al, Yen et al, Armstrong et al, p = 0.02; 2 p = 0.05; 3 p =")
60
Conclusions on IPCT Combined use of IV and IP chemotherapy leads to a significant survival benefit in women with optimally debulked EOC (median + 12 mo). Based on the most recent trials, strong consideration should be given to a regimen with IP cisplatin (100 mg/m²) and a taxane (whether IV or IP). Toxicities, inconvenience and costs of IP therapy are justified by the improved survival.
. Based on the most recent trials, strong consideration should be given to a regimen with IP cisplatin (100 mg/m²) and a taxane (whether IV or IP). Toxicities, inconvenience and costs of IP therapy are justified by the improved survival.")
61
Intraperitoneal Chemotherapy
Conclusions IP chemotherapy had a significantly better PFS and OS for women with optimally cytoreduced Stage III EOC Significant toxicity with IP chemotherapy (only 40% of women completed 6 cycles) Most patients had abdominal port/catheter issues that resulted in conversion to IV carboplatin rather than IP chemotherapy Opponents of IP chemotherapy argue that the IP regimen is not being compared to the current standard of care (Carboplatin and Taxol) Proponents argue that Cisplatin and Taxol is equally effective as Carboplatin and Taxol (GOG #158)
 Most patients had abdominal port/catheter issues that resulted in conversion to IV carboplatin rather than IP chemotherapy. Opponents of IP chemotherapy argue that the IP regimen is not being compared to the current standard of care (Carboplatin and Taxol) Proponents argue that Cisplatin and Taxol is equally effective as Carboplatin and Taxol (GOG #158)")
Similar presentations