Download presentation
Presentation is loading. Please wait.

1
Kamal Akl MD Associate Professor of Pediatrics/Nephrology Jordan University Hospital

2
To review the various genetic etiologies of the hereditary nephropathies Emphasis on genetic nephrotic syndrome The new taxonomy of the podocytopathies

3
Clinical Presentation GBM diseases Hematuria Podocyte diseases Proteinuria

4
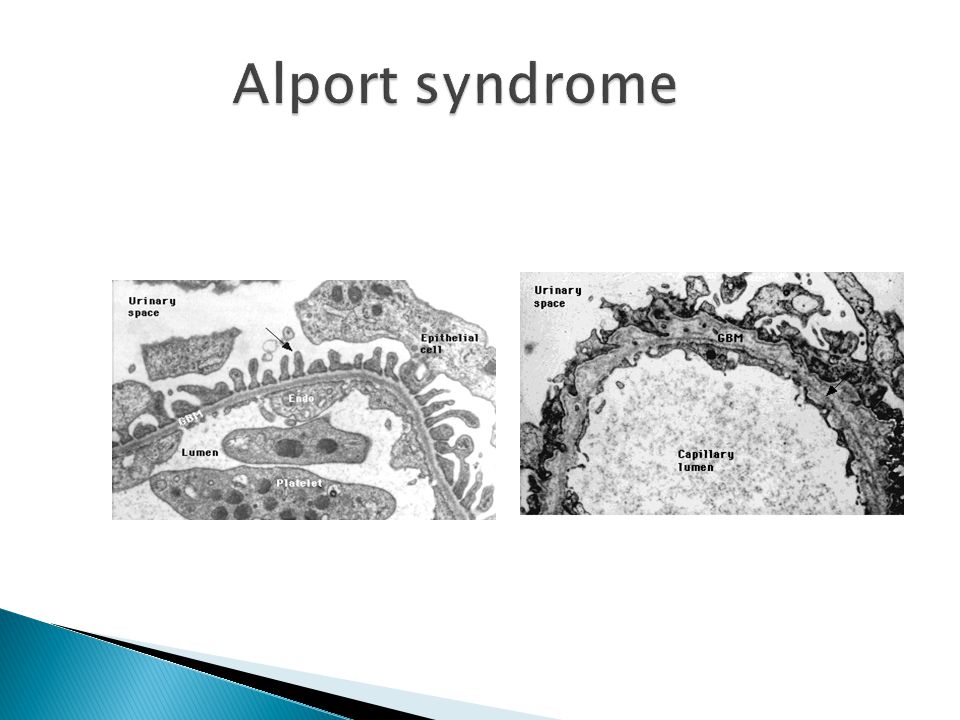
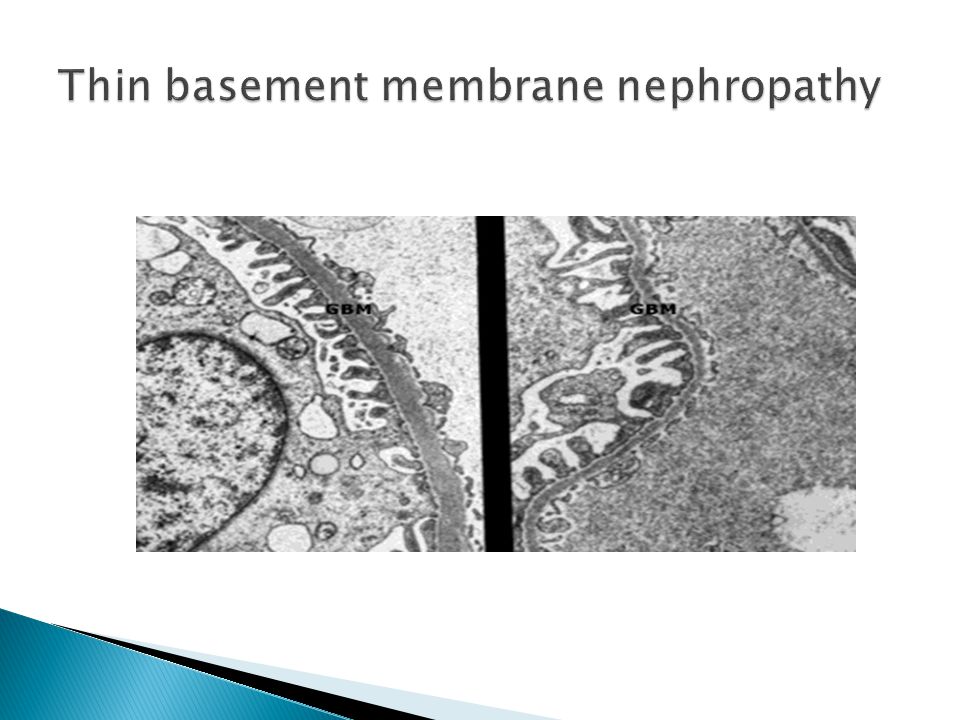
Type IV collagen ( hematuric diseases) a) Alport syndrome b) TBMN c) Familial hematuria with retinal arteriolar tortuosity & contractures Laminin β2 Pierson syndrome Gubler MC Nat Genet Clin Practice Nephrology 2008
 a) Alport syndrome b) TBMN c) Familial hematuria with retinal arteriolar tortuosity & contractures Laminin β2 Pierson syndrome Gubler MC Nat Genet Clin Practice Nephrology 2008")
5
X – linked dominant : 85% Autosomal recessive : 10-15% Autosomal dominant

8
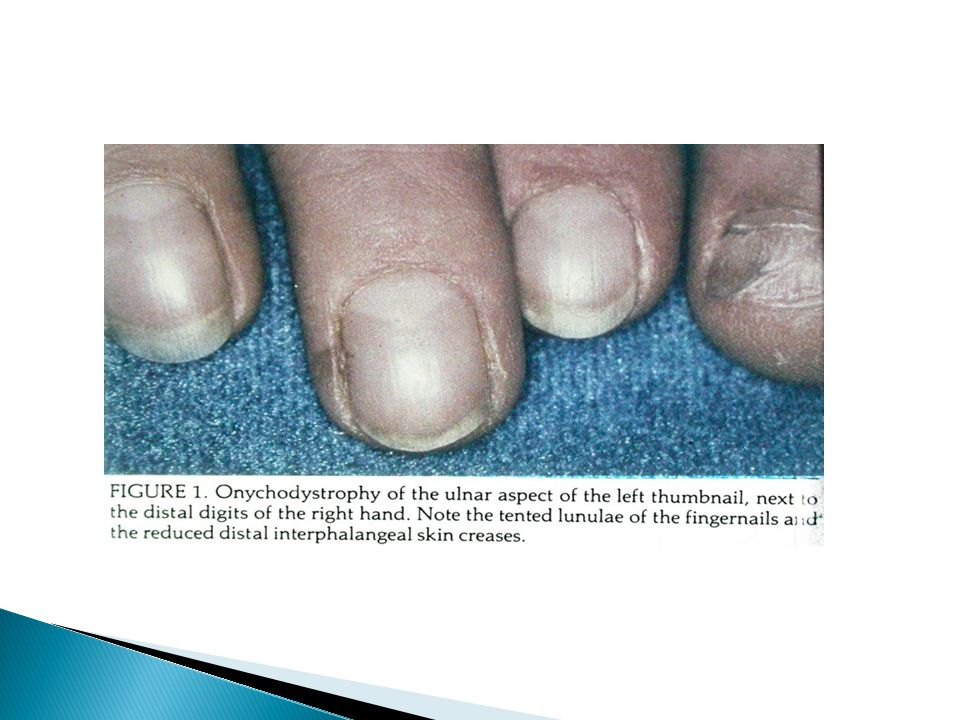
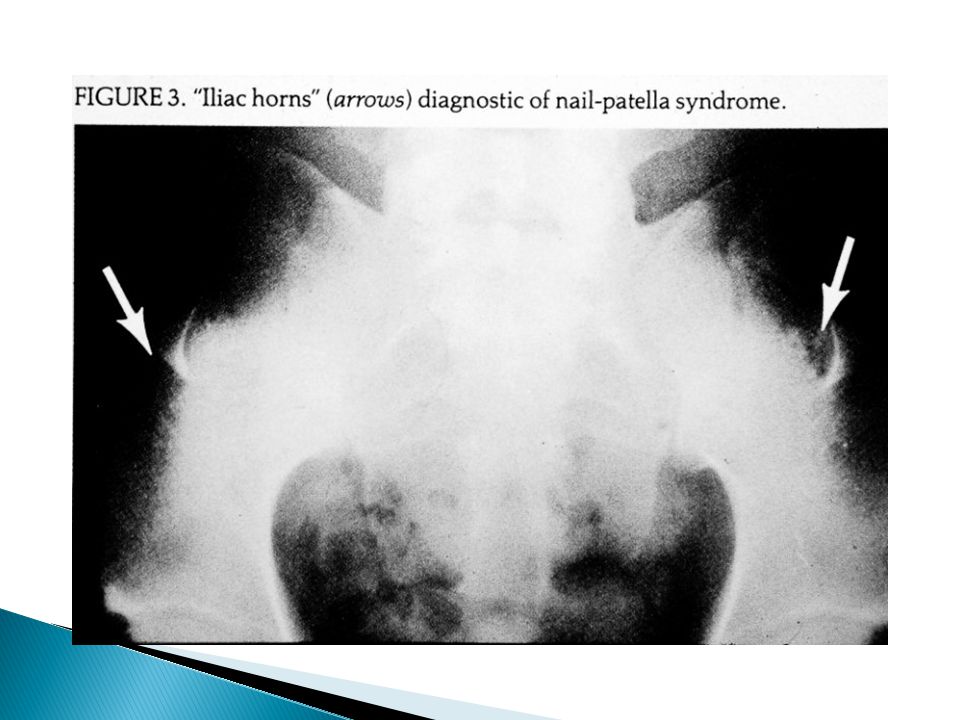
Type III collagen a) Nail patella syndrome b) Idiopathic collagen type III glomerulopathy Fibronectin Fibronectin glomerulopathy
 Nail patella syndrome b) Idiopathic collagen type III glomerulopathy Fibronectin Fibronectin glomerulopathy")
9
Dominant mutation of LMX1B gene Hypoplastic nails Absent patellae Renal dysplasia Chen et al Nat Genet 1998

14
Disorders of early glomerular development -> manifesting antenatally, perinatally, or in early infancy Disorders with late onset NS -> manifesting as FSGS in adulthood

16
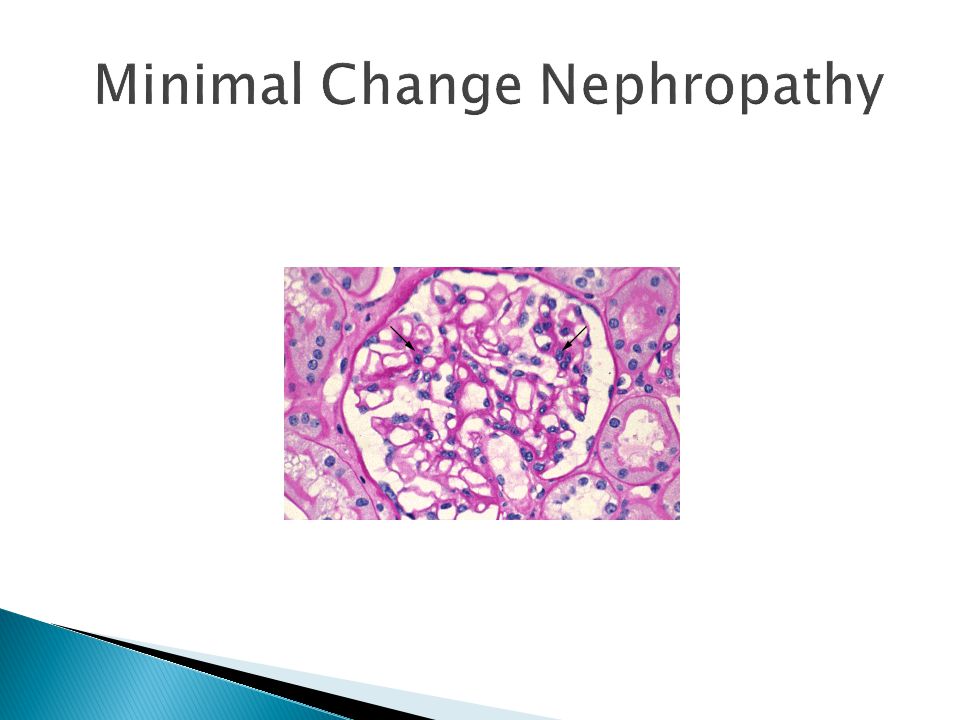
EM

19
Proteinuria Proteinuria

20
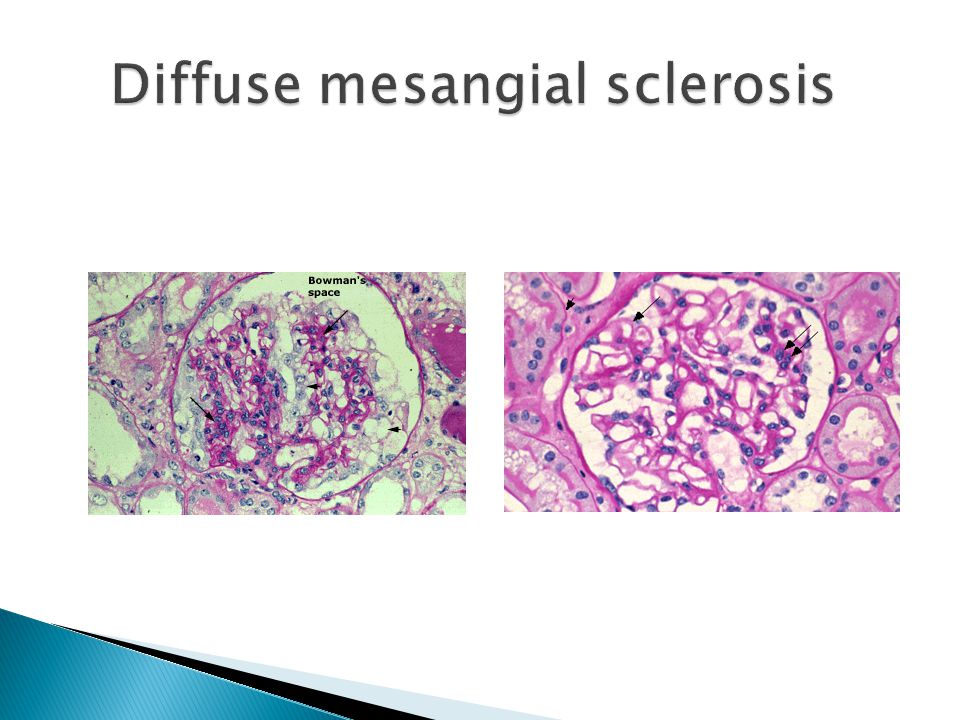
(1) No change in podocyte number-> MCN (2) Podocyte detachment/death -> FSGS (3) Podocyte proliferation : (a) Low -> DMS (b) High -> CG Barisoni L, et al Clin J Am Soc Nephrol 2007
 No change in podocyte number-> MCN (2) Podocyte detachment/death -> FSGS (3) Podocyte proliferation : (a) Low -> DMS (b) High -> CG Barisoni L, et al Clin J Am Soc Nephrol 2007")
22
LM -> segmental solidification of the tuft with accumulation of extracellular matrix synechiae from between the tuft and bowmans capsule. Podocytes are lost in the area of sclerosis

24
LM-> The characteristic features of CG include wrinkling and folding of the glomerular basement membranes (collapse) and proliferation of overlying podocytes forming pseudocrescents.
 and proliferation of overlying podocytes forming pseudocrescents.")
25
. Albaqumi M, Barisoni L JASN 2008;19:1276-1281 ©2008 by American Society of Nephrology

26
Nonsyndromic : (1) NPHS2 -> SRMCN (AR) (2) AD FSGS or MCN ( chromosome 19q) Syndromic DYSF ( limb- girdle muscular dystrophy 2B ) Vats A et al Kidney Int 2000 Winn MP et al Science 2005 Izzedine H et al Am J Kidney Dis 2006
 NPHS2 -> SRMCN (AR) (2) AD FSGS or MCN ( chromosome 19q) Syndromic DYSF ( limb- girdle muscular dystrophy 2B ) Vats A et al Kidney Int 2000 Winn MP et al Science 2005 Izzedine H et al Am J Kidney Dis 2006")
27
Nonsyndromic NPHS1+NPHS2 NPHS2 ACTN4 CD 2 AP TRPC6 WT1 mt DNA t RNA leu Tryggvason K et al N Engl J Med 2006

28
Syndromic WT1 ( Frasier) mDNA t RNA leu (MELAS) Guery B et al J Am Soc Nephrolk 2003 PAX2 ( renal – coloboma syndrome with oligomeganephronia LMX1B ( Nail-patella ) BongersEM et al Europ J Hum Genet 2005 ITGB4 COL4A3,A4,A5 (Alport) ( Churg J et al Arch Pathol 1973) GLA(Fabry) ( Branton MH et al Medicine (Baltimore) 2002 )
 mDNA t RNA leu (MELAS) Guery B et al J Am Soc Nephrolk 2003 PAX2 ( renal – coloboma syndrome with oligomeganephronia LMX1B ( Nail-patella ) BongersEM et al Europ J Hum Genet 2005 ITGB4 COL4A3,A4,A5 (Alport) ( Churg J et al Arch Pathol 1973) GLA(Fabry) ( Branton MH et al Medicine (Baltimore) 2002 )")
29
NPHS2 AR Homozygous or compound heterozygous mutations Caridi G et al J Am Soc Nephrol 2003 Onset : childhood---4 th decade Tsukaguchi H et al J Clin Invest 2002

30
Morphologic presentations : (1) MCN (2) Diffuse mesangial hypercellularity (3) FSGS Importance of genetic testing Ruf RG et al J Am Soc Nephrol 2004
 MCN (2) Diffuse mesangial hypercellularity (3) FSGS Importance of genetic testing Ruf RG et al J Am Soc Nephrol 2004")
31
AD : Present in adulthood : (1)ACTN4 ( Kaplan JM et al Nat Genet 2000 ) (2)Unidentified gene near same location (Winn MP et al Kidney Int 1999 ) (3)TRPC6 ( Izzedine H et al Am J Kidney Dis 2006 )
ACTN4 ( Kaplan JM et al Nat Genet 2000 ) (2)Unidentified gene near same location (Winn MP et al Kidney Int 1999 ) (3)TRPC6 ( Izzedine H et al Am J Kidney Dis 2006 )")
32
Chromosome 19q13 mutations present with morphologic heterogeneity (=NPHS2 mutations) : (a) SR MCN (b) Mesangial hypercellularity (3) FSGS Vats A et al Kidney Int 2000 Winn MP et al Kidney Int 1999
 : (a) SR MCN (b) Mesangial hypercellularity (3) FSGS Vats A et al Kidney Int 2000 Winn MP et al Kidney Int 1999")
33
Nonsyndromic (1) NPHS1 (2) WT1 (3) NPHS2 (4) PLCE1
 NPHS1 (2) WT1 (3) NPHS2 (4) PLCE1")
34
Syndromic : (1) LAMB2 (Pierson) (2) WT1 ( Deny- Drash)
 LAMB2 (Pierson) (2) WT1 ( Deny- Drash)")
35
Columbia classification D, Agati VD Am J Kidney Dis 2004

36
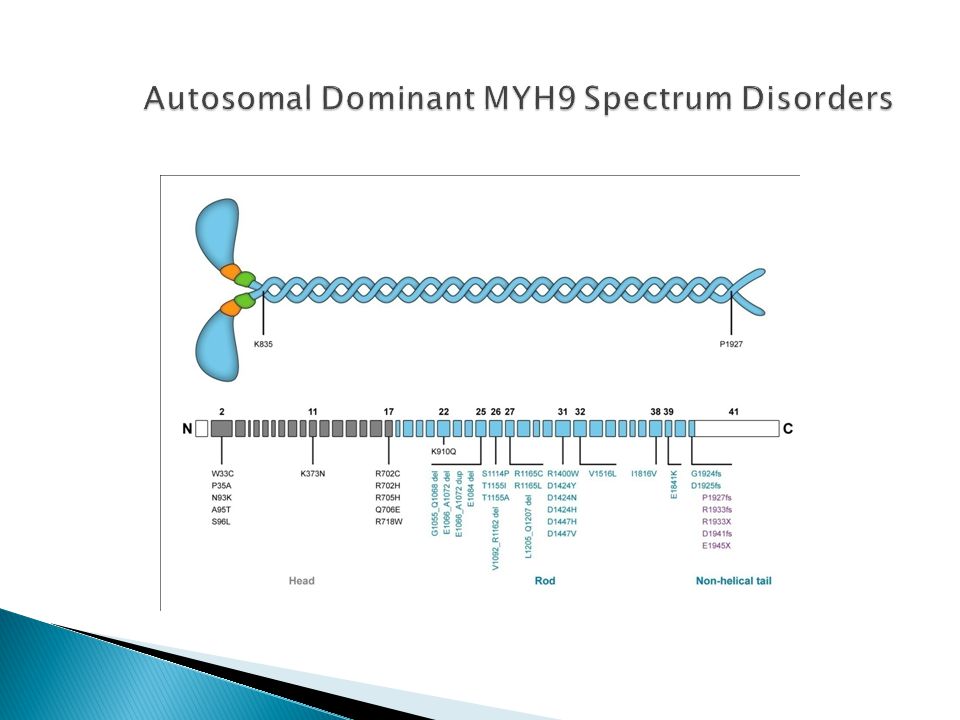
May-Hegglin anomaly Sebastian syndrome Fechtner syndrome Epstein syndrome Isolated sensorineural deafness

37
R 702 mutations in MHY9 chain encoding non muscle myosin IIA heavy chain Sekine T et al. Kidney Int 2010.

39
Giant platelets

40
FSGS at an early stage of CKD ? Primary podocyte injury rather than postadaptive FSGS consequent to decreased number of functioning nephrons

41
MYH9 kidney risk variants: HIV associated CG FSGS Hypertension-attributed ESKD among african descent population Kopp JB et al. Nat Genet 2008

42
Different from Fechtner & Epstein syndromes Autosomal recessive rather than dominant ? New mutation of a known disease ? A new syndrome

43
Hereditary glomerular diseases were reviewed Clinical classification alone is not suffient Histopathologic classication alone is not adequate Best is : genetic +clinical + histopathologic

44
Limitations in classifying the podocytopathies Different morphologic presentations for a particular genetic mutation Various histopathologic of a particular disease vs progression from one disease to another Multiple glomerular morphologies on one renal biopsy (Meyrier A Semin Nephrol 2003

45
Thank you

Similar presentations