Download presentation
Presentation is loading. Please wait.

1
INIBITORI DELL’AROMATASI
FRANCESCO BOCCARDO INIBITORI DELL’AROMATASI (back from San Antonio) Professore Ordinario di Oncologia Medica, Università di Genova Direttore Oncologia Medica B IST .Genova Presidente Nazionale Associazione Italiana Oncologia Medica
 Professore Ordinario di Oncologia Medica, Università di Genova. Direttore Oncologia Medica B IST .Genova. Presidente Nazionale Associazione Italiana Oncologia Medica.")
2
? ? ? ? ? ? Decision Points 1 4 3 2 3 4 Tamoxifen Aromatase inhibitor
Initial diagnosis 2-3 years after Tam or AI 5 years after Tam or AI Beyond 10 years? Tamoxifen Aromatase inhibitor 1 ? 4 ? 3 ? AI, aromatase inhibitor; Tam, tamoxifen Several distinct patient populations can benefit from hormonal therapy; this slide highlights some of the nodal decision points regarding current thinking about the treatment of these various groups of women. Some women who are newly diagnosed with breast cancer must choose between upfront therapy with an AI vs upfront therapy with tamoxifen, followed by a planned crossover or sequence of treatment including an AI. Women who have been on tamoxifen for 2 or 3 years must decide whether to remain on tamoxifen therapy or switch to an AI. Similarly, women who are finishing approximately 5 years of tamoxifen need to decide whether to transition to an AI. Remaining questions include how to treat a woman who has completed 5 years of AI therapy, but who may not have received tamoxifen, and determination of whether she should continue to receive an AI long-term. Similarly, it remains unclear how long to treat women who have received several years of tamoxifen followed by several years of an AI. These are practical and important questions because we are already faced with such patients in clinical practice. 2 3 ? ? ? 4 5 years total 10 years total > 10 years 2

3
Decision Points:after 2-3 yrs of Tam
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI More IES ABCSG8/ARNO95 ITA 1 ? Tamoxifen ABCSG8, Austrian Breast and Colorectal Study Group trial 8; AI, aromatase inhibitor; ARNO95, Arimidex-Nolvadex 95 trial; ATAC, Arimidex, Tamoxifen, Alone or in Combination; BIG, Breast International Group; IES, Intergroup Exemestane Study; NSABP; National Surgical Adjuvant Breast and Bowel Project; Tam, tamoxifen. All 3 approved aromatase inhibitors – anastrozole, exemestane, and letrozole -- have been studied in large, definitive trials designed to evaluate the potential of aromatase inhibitors to improve the results over that seen with tamoxifen alone. The ATAC and BIG 1-98 studies challenged the primacy of tamoxifen as initial therapy. The IES and ABCSG8/ARNO95 studies evaluated the potential benefit of early switching from tamoxifen to aromatase inhibitors. Finally, NCIC MA.17 has provided important information on the issue of long‑term hormonal therapy after completion of 5 years of tamoxifen. ? Aromatase inhibitor 5 years total 10 years total > 10 years 3

4
The Lancet 9561:533-5, 2007

5
The Lancet 9561:533-5, 2007

6
The Lancet 9561:533-5, 2007

7
AIOG Metanalysis

11
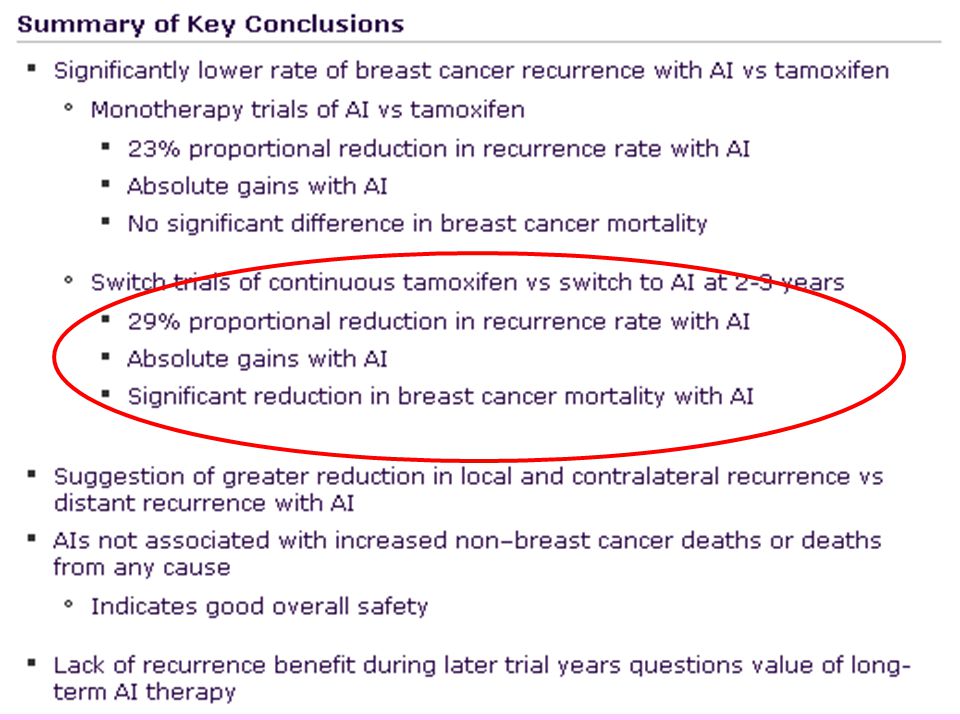
……….back from San Antonio 2008: take home #1
“There is a clear benefit (including a S benefit) in switching women already on treatment with Tam to an AI (anastrozole,exemestane) unless AI therapy is contraindicated”
 in switching women already on treatment with Tam to an AI (anastrozole,exemestane) unless AI therapy is contraindicated")
12
Decision Points: Initial choice
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI Beyond 10 years? Tamoxifen Aromatase inhibitor ? ? 2 ATAC BIG 1-98 monotherapy TEAM 2.75 yr ? ? ? 5 years total 10 years total > 10 years

14
ATAC:100 mos median follow-up , Lancet Oncology 2007

15
AIOG Metanalysis

19
: TEAM trial

23
……….back from San Antonio 2008: take home #2
“Three drugs now available as front line treatment: Which drug or which patients?”

24
ATAC:100 mos median follow-up , Lancet Oncology 2007

25
Predicting the benefit and the risks. Tamoxifen vs Ais:
Tumor Profile Patient Profile ERPgR HER2 Recurrence Score Cyclin E uPA/uPAI-1 Bcl-2 ER-beta Osteoporosis Hypercholesterolemia CV risk factors Endometrial pathologies DVT & TE risk factors SSRI use CYP 19 Genotype CYP2D6 Genotype

26
TRANSACT

29
ABCSG 8

33
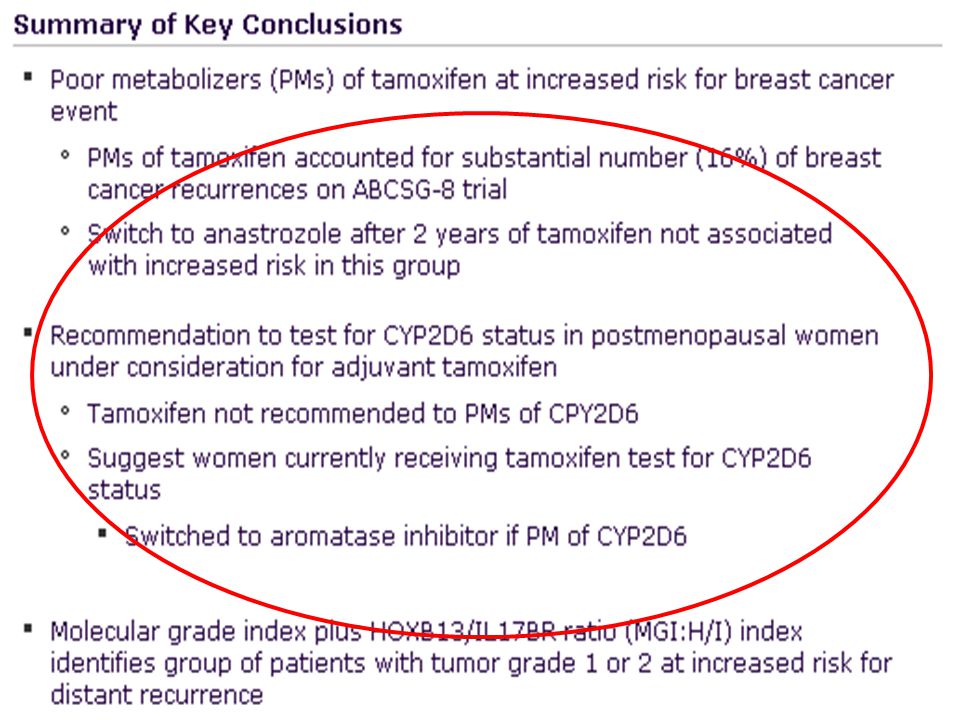
……….back from San Antonio 2008: take home #3
“Starting with an Ai is a reasonable choice especially in certain patient subsets (i.e. PgRneg,HER2 pos,HRScore Node neg,poor metabolizers of CYP2D6….!):however: 1) no major mortality advantge 2) No over rate in selecting patients “
:however: 1) no major mortality advantge. 2) No over rate in selecting patients")
34
Decision Points:sequencing
Initial diagnosis 2-3 years after Tam or AI 5 years after Tam or AI Beyond 10 years? Tamoxifen Aromatase inhibitor 1 ? 4 ? 3 ABCSG8 TEAM 5-yr: n.a. yet ? AI, aromatase inhibitor; Tam, tamoxifen Several distinct patient populations can benefit from hormonal therapy; this slide highlights some of the nodal decision points regarding current thinking about the treatment of these various groups of women. Some women who are newly diagnosed with breast cancer must choose between upfront therapy with an AI vs upfront therapy with tamoxifen, followed by a planned crossover or sequence of treatment including an AI. Women who have been on tamoxifen for 2 or 3 years must decide whether to remain on tamoxifen therapy or switch to an AI. Similarly, women who are finishing approximately 5 years of tamoxifen need to decide whether to transition to an AI. Remaining questions include how to treat a woman who has completed 5 years of AI therapy, but who may not have received tamoxifen, and determination of whether she should continue to receive an AI long-term. Similarly, it remains unclear how long to treat women who have received several years of tamoxifen followed by several years of an AI. These are practical and important questions because we are already faced with such patients in clinical practice. 2 3 BIG-1-98 ? ? ? 4 5 years total 10 years total > 10 years 34

35
ABCSG Trial 8 Sequencing versus TAM Switch point Switching period
Tamoxifen (2 years) Tamoxifen (3 years) Randomi ze Primary surgery ABCSG, Austrian Breast Cancer Study Group. The ABCSG trial 8 is unique among the switching trials in that patients were randomized before initiation of 2 years of tamoxifen. Thus, ABSCG trial 8 provides some overall information on how patients respond, including the patients who relapse early on tamoxifen. This has been a key question in ascertaining whether it is better to initiate aromatase inhibitor therapy at the start of hormonal therapy or use the sequencing approach. Tamoxifen (2 years) Anastrozole (3 years) Switching period Sequencing period Jakesz R, et al. Lancet. 2005;366: 35
 Tamoxifen (3 years) Randomi ze. Primary surgery. ABCSG, Austrian Breast Cancer Study Group. The ABCSG trial 8 is unique among the switching trials in that patients were randomized before initiation of 2 years of tamoxifen. Thus, ABSCG trial 8 provides some overall information on how patients respond, including the patients who relapse early on tamoxifen. This has been a key question in ascertaining whether it is better to initiate aromatase inhibitor therapy at the start of hormonal therapy or use the sequencing approach. Tamoxifen (2 years) Anastrozole (3 years) Switching period. Sequencing period. Jakesz R, et al. Lancet. 2005;366:")
36
Time Since Surgery (Months)
ABCSG 8 seq:Event-Free Survival following surgery (n = 2926) 100 94.4% 95 90 92.9% EFS (%) 85 Events T 101 T A 79 HR 0.76 P Value .068 A, anastrozole; EFS, event-free survival; HR, hazard ratio; T, tamoxifen. In looking at the 5‑year event-free survival from initiation of hormonal therapy, the switch from tamoxifen to anastrozole improved rates from 92.9% to 94.4%, respectively. This corresponded to a hazard ratio of 0.76 (P = .068). 80 T 75 T A 12 24 36 48 60 72 Time Since Surgery (Months) Jakesz R, et al SABCS. Abstract 13 36
 % % EFS (%) 85. Events. T T A. 79. HR P Value A, anastrozole; EFS, event-free survival; HR, hazard ratio; T, tamoxifen. In looking at the 5‑year event-free survival from initiation of hormonal therapy, the switch from tamoxifen to anastrozole improved rates from 92.9% to 94.4%, respectively. This corresponded to a hazard ratio of 0.76 (P = .068). 80. T. 75. T A Time Since Surgery (Months) Jakesz R, et al SABCS. Abstract")
37
Sequencing versus LTZ

42
Take home #3

43
DOUBLE TRIAL Switch point Switching period Sequencing period LTZ/ANA
(2 years) Examestane (3 years) Randomi ze Primary surgery ABCSG, Austrian Breast Cancer Study Group. The ABCSG trial 8 is unique among the switching trials in that patients were randomized before initiation of 2 years of tamoxifen. Thus, ABSCG trial 8 provides some overall information on how patients respond, including the patients who relapse early on tamoxifen. This has been a key question in ascertaining whether it is better to initiate aromatase inhibitor therapy at the start of hormonal therapy or use the sequencing approach. LTZ/ANA (2 years) LTZ/ANA (3 years) Switching period Sequencing period 43
 Examestane (3 years) Randomi ze. Primary surgery. ABCSG, Austrian Breast Cancer Study Group. The ABCSG trial 8 is unique among the switching trials in that patients were randomized before initiation of 2 years of tamoxifen. Thus, ABSCG trial 8 provides some overall information on how patients respond, including the patients who relapse early on tamoxifen. This has been a key question in ascertaining whether it is better to initiate aromatase inhibitor therapy at the start of hormonal therapy or use the sequencing approach. LTZ/ANA (2 years) LTZ/ANA (3 years) Switching period. Sequencing period. 43.")
44
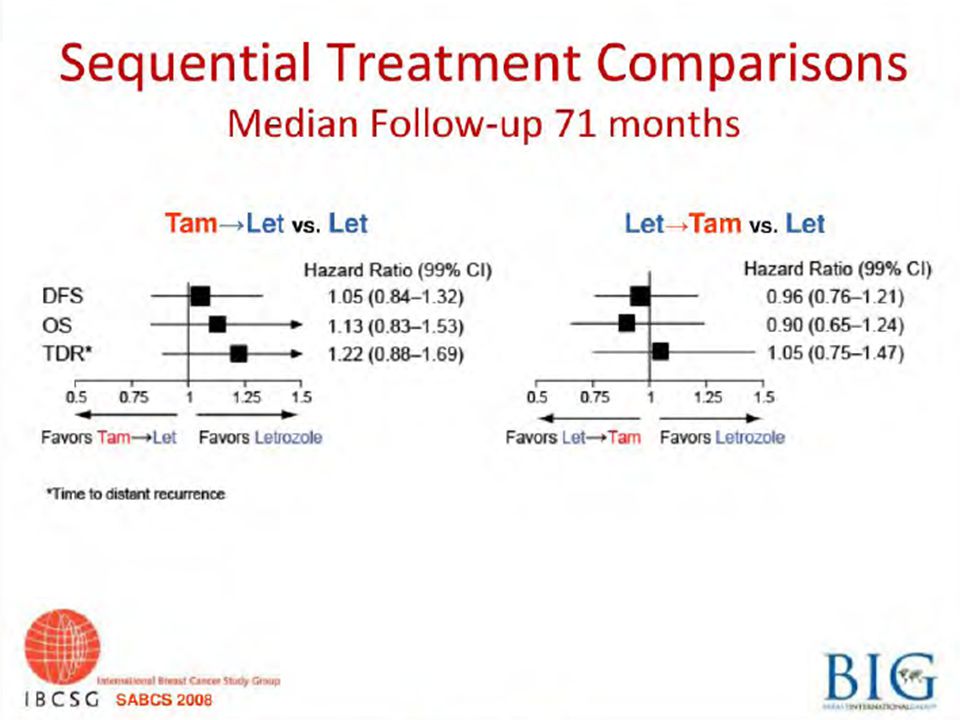
……….back from S. Antonio 2008: Take home #4
“sequencing TAM with an Ai is probably better than TAM alone,but does not offer major advantages vs Ai alone; switching from an Ai to TAM is possible if required… “

45
Decision Points:after 5 yrs of Tam
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI More NSABP B-14 ? MA.17 ABCSG6a Tamoxifen ? ABCSG8, Austrian Breast and Colorectal Study Group trial 8; AI, aromatase inhibitor; ARNO95, Arimidex-Nolvadex 95 trial; ATAC, Arimidex, Tamoxifen, Alone or in Combination; BIG, Breast International Group; IES, Intergroup Exemestane Study; NSABP; National Surgical Adjuvant Breast and Bowel Project; Tam, tamoxifen. All 3 approved aromatase inhibitors – anastrozole, exemestane, and letrozole -- have been studied in large, definitive trials designed to evaluate the potential of aromatase inhibitors to improve the results over that seen with tamoxifen alone. The ATAC and BIG 1-98 studies challenged the primacy of tamoxifen as initial therapy. The IES and ABCSG8/ARNO95 studies evaluated the potential benefit of early switching from tamoxifen to aromatase inhibitors. Finally, NCIC MA.17 has provided important information on the issue of long‑term hormonal therapy after completion of 5 years of tamoxifen. Aromatase inhibitor NSABP B-42 5 years total 10 years total > 10 years

46
NSABP B-14: No Benefit of Extending Tamoxifen Beyond 5 Years
DFS OS 100 100 94% 90 90 91% 82% P = .07 80 P = .03 80 Percentage of Patients 78% Percentage of Patients 70 Placebo Tamoxifen 70 Placebo Tamoxifen 60 60 DFS, disease-free survival; OS, overall survival. At 7 years of follow‑up following rerandomization, patients continuing tamoxifen had a lower disease‑free survival of 78% compared with 82% in those receiving placebo (P = .03). There was also a 3% difference in overall survival favoring placebo, which did not quite reach statistical significance at (P = .07). Although the study clearly demonstrated discontinuation of tamoxifen after 5 years of therapy was appropriate for these node-negative, hormone receptor–positive patients, it is important to note that 18% of the placebo arms had subsequent events in the 7 years after completion of standard tamoxifen therapy. 50 50 1 2 3 4 5 6 7 1 2 3 4 5 6 7 Years Years Tamoxifen demonstrated higher rates of endometrial cancer, and more deaths from ischemic heart disease and cerebrovascular disease Fisher B, et al. J Natl Cancer Inst. 2001;93:
. There was also a 3% difference in overall survival favoring placebo, which did not quite reach statistical significance at (P = .07). Although the study clearly demonstrated discontinuation of tamoxifen after 5 years of therapy was appropriate for these node-negative, hormone receptor–positive patients, it is important to note that 18% of the placebo arms had subsequent events in the 7 years after completion of standard tamoxifen therapy Years. Years. Tamoxifen demonstrated higher rates of endometrial cancer, and more deaths from ischemic heart disease and cerebrovascular disease. Fisher B, et al. J Natl Cancer Inst. 2001;93:")
47
MA.17: Key Endpoints in Nodal Subgroups
Preplanned analysis (n = 5187) HR: 0.45 ( ) HR: 0.63 ( ) HR: 1.52 ( ) Node* neg Node neg Node neg Distant* DFS HR: 0.82 ( ) DFS* OS DFS, disease-free survival; HR, hazard ratio; neg, negative; OS, overall survival; pos, positive. The sample size allowed for a planned analysis of benefit by nodal status. The hazard ratio for disease‑free survival was similar for both node-negative and node-positive patients and reached statistical significance. For distant disease-free survival, the hazard rates were again similar, although significance was only noted in the higher event node-positive group. Interestingly, survival was improved in node-positive patients, but no benefit was apparent among node-negative patients and the hazard ratio was actually greater than 1, although the confidence interval ranged from HR: 0.58 ( ) HR: 0.61 Node* pos Node* pos Node* pos HR: 0.61 ( ) HR: 0.53 ( ) HR: 0.61 ( ) *non statistically significant Goss PE, et al. J Natl Cancer Inst. 2005;97:
 HR: ( ) HR: ( ) HR: ( ) Node* neg. Node neg. Node neg. Distant* DFS. HR: ( ) DFS* OS. DFS, disease-free survival; HR, hazard ratio; neg, negative; OS, overall survival; pos, positive. The sample size allowed for a planned analysis of benefit by nodal status. The hazard ratio for disease‑free survival was similar for both node-negative and node-positive patients and reached statistical significance. For distant disease-free survival, the hazard rates were again similar, although significance was only noted in the higher event node-positive group. Interestingly, survival was improved in node-positive patients, but no benefit was apparent among node-negative patients and the hazard ratio was actually greater than 1, although the confidence interval ranged from HR: ( ) HR: Node* pos. Node* pos. Node* pos. HR: ( ) HR: ( ) HR: ( ) *non statistically significant. Goss PE, et al. J Natl Cancer Inst. 2005;97:")
48
Adjusted HR (PLAC-LET to PLAC) for Efficacy Outcomes :postumblinding
Disease-free survival Distant disease-free survival Overall survival Contralateral breast cancer 0.6 0.53 0.5 p=0.05 P = .05 0.4 Hazard Ratio 0.31 0.28 0.3 HR, hazard ratio; LET, letrozole; PLAC, placebo. In fact, the hazard ratios for disease‑free survival, distant disease‑free survival, and contralateral breast cancer were strikingly low at 0.31, 0.28, and 0.23, respectively. The overall survival hazard ratio was also a remarkable 0.53. p<0.0001 0.23 P < .0001 p=0.002 P = .002 0.2 p=0.012 P = .012 0.1 PLAC-LET to PLAC Goss PE, et al. SABCS Abstract 16.

49
………back from S.Antonio 2008: Take home #5
“ Late switching after 5 yrs of TAM: no news “

50
Decision Points:after 5 yrs of AIs
Initial diagnosis 2-3 years after Tam 5 years after Tam or AI More NSABP B-14 ? MA.17 Tamoxifen ? ABCSG8, Austrian Breast and Colorectal Study Group trial 8; AI, aromatase inhibitor; ARNO95, Arimidex-Nolvadex 95 trial; ATAC, Arimidex, Tamoxifen, Alone or in Combination; BIG, Breast International Group; IES, Intergroup Exemestane Study; NSABP; National Surgical Adjuvant Breast and Bowel Project; Tam, tamoxifen. All 3 approved aromatase inhibitors – anastrozole, exemestane, and letrozole -- have been studied in large, definitive trials designed to evaluate the potential of aromatase inhibitors to improve the results over that seen with tamoxifen alone. The ATAC and BIG 1-98 studies challenged the primacy of tamoxifen as initial therapy. The IES and ABCSG8/ARNO95 studies evaluated the potential benefit of early switching from tamoxifen to aromatase inhibitors. Finally, NCIC MA.17 has provided important information on the issue of long‑term hormonal therapy after completion of 5 years of tamoxifen. Aromatase inhibitor NSABP B-42 MA.17-R 5 years total 10 years total > 10 years

51
NSABP B-42: Study Design Letrozole x 5 yrs AI x 5 yrs Tam x 2-3 yrs
Letrozole vs placebo after 5 years; not yet enrolling Letrozole x 5 yrs AI x 5 yrs Tam x 2-3 yrs AI x 3-2 yrs Placebo x 5 yrs NSABP, National Surgical Adjuvant Breast and Bowel Project; AI, aromatase inhibitor; Tam, tamoxifen The National Surgical Adjuvant Breast and Bowel Project (NSABP) has initiated trial B-42, a study which is still being formulated but which will hopefully begin accruing patients soon. B-42 will evaluate women who have had either 5 years of an AI as their primary adjuvant endocrine treatment or primary treatment consisting of 2-3 years of tamoxifen followed by 2-3 years of an AI. Obviously, these women will still be free of cancer recurrence and would then be eligible for treatment with either letrozole or a placebo. The goal here is to clarify the duration of AI therapy in women who have already been cancer free for at least 5 years.
 has initiated trial B-42, a study which is still being formulated but which will hopefully begin accruing patients soon. B-42 will evaluate women who have had either 5 years of an AI as their primary adjuvant endocrine treatment or primary treatment consisting of 2-3 years of tamoxifen followed by 2-3 years of an AI. Obviously, these women will still be free of cancer recurrence and would then be eligible for treatment with either letrozole or a placebo. The goal here is to clarify the duration of AI therapy in women who have already been cancer free for at least 5 years.")
52
MA.17R: Design 5 years’ early adjuvant 5 years’ extended adjuvant
Rerandomization (Disease-free) Letrozole 2.5 mg qd Letrozole Placebo qd 5 years’ early adjuvant 5 years’ extended adjuvant DFS, disease-free survival; OS, overall survival; qd, once daily; QoL, quality of life The MA.17R trial is attempting to determine the optimal duration of endocrine therapy for women with early‑stage breast cancer. Interestingly, lifelong estrogen deprivation as a potential treatment option for women with a history of breast cancer is being considered. However, it is unclear whether lifelong therapy is better than endocrine therapy of finite duration. Ongoing side effects of estrogen deprivation include menopausal symptoms, osteoporosis, vaginal dryness, and hypercholesterolemia. Moreover, the long-term risks are unclear. Thus, MA.17‑R stands as a seminal study beginning to define these questions of treatment duration. [What does the * after Disease-free refer to? (GK)] okay to delete … we moved the “disease-free” up. AHW [Added apostrophes after years, as in slide 23. (GK)] Primary endpoint: DFS Secondary endpoints: OS, incidence of contralateral breast cancer, long-term clinical and laboratory safety, overall QoL, menopausal QoL
 Letrozole 2.5 mg qd. Letrozole. Placebo qd. 5 years’ early adjuvant. 5 years’ extended adjuvant. DFS, disease-free survival; OS, overall survival; qd, once daily; QoL, quality of life. The MA.17R trial is attempting to determine the optimal duration of endocrine therapy for women with early‑stage breast cancer. Interestingly, lifelong estrogen deprivation as a potential treatment option for women with a history of breast cancer is being considered. However, it is unclear whether lifelong therapy is better than endocrine therapy of finite duration. Ongoing side effects of estrogen deprivation include menopausal symptoms, osteoporosis, vaginal dryness, and hypercholesterolemia. Moreover, the long-term risks are unclear. Thus, MA.17‑R stands as a seminal study beginning to define these questions of treatment duration. [What does the * after Disease-free refer to (GK)] okay to delete … we moved the disease-free up. AHW. [Added apostrophes after years, as in slide 23. (GK)] Primary endpoint: DFS. Secondary endpoints: OS, incidence of contralateral breast cancer, long-term clinical and laboratory safety, overall QoL, menopausal QoL.")
53
…….back from S. Antonio 2008: Take home #6
“ are trials concerning Ai optimal duration still justified? “

54
ZO-FAST

56
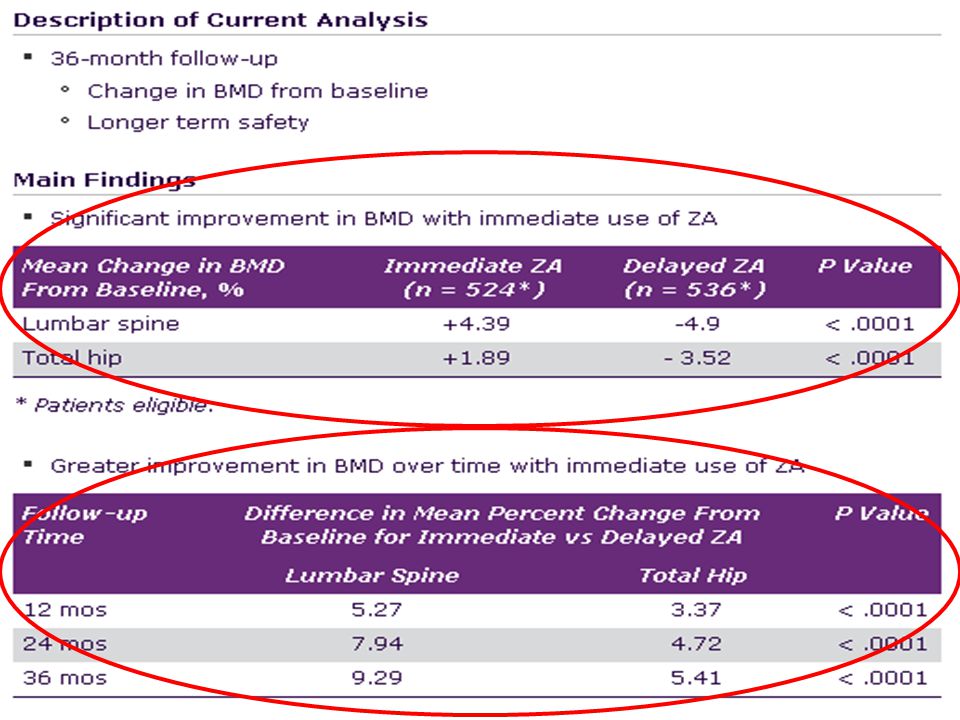
Immediate Therapy With Zoledronic Acid Prevents Bone Loss and Improves DFS in Women With Early Breast Cancer Receiving Letrozole Zometa-Femara Adjuvant Synergy Trial (ZO-FAST): 36-month follow-up results of multicenter, randomized phase III trial[1]
: 36-month follow-up results of multicenter, randomized phase III trial[1]")
57
…….back from S. Antonio 2008: Take home #7
“ the seed and soil theory likely to work: data from ABCSG 12 confirmed!”

58
AIs IN THE ADJUVANT SETTING,back from San Antonio 2008:
EARLY SWITCHING : 1) the new standard for the patients already on treatment with TAM from 2 or 3 yrs 2) switching from LTZ to TAM after 2-3 yrs possible if required LATE SWITCHING : a reasonable option for patients at the completion of 5 yrs of TAM, namely for N pos (no news from San Antonio) UPFRONT : the choice for the patients who have contraindications to the use of TAM. A reasonable choice for the patients at higher risk of relapse (HR score) or for whom a suboptimal response to TAM might be predicted (CYPD26) : cost/benefit to be defined in the individual patient (no S advantage on the average) SEQUENCING : 1) no better /no worse than LTZ 2) no evidence yet in respect to TAM
 the new standard for the patients already on treatment with. TAM from 2 or 3 yrs. 2) switching from LTZ to TAM after 2-3 yrs possible if required. LATE. SWITCHING : a reasonable option for patients at the completion of 5 yrs of. TAM, namely for N pos (no news from San Antonio) UPFRONT : the choice for the patients who have contraindications to the. use of TAM. A reasonable choice for the patients at higher risk. of relapse (HR score) or for whom a suboptimal response to. TAM might be predicted (CYPD26) : cost/benefit to be defined. in the individual patient (no S advantage on the average) SEQUENCING : 1) no better /no worse than LTZ. 2) no evidence yet in respect to TAM.")
59
………back from S.Antonio 2008: Take home #8
“ THANK YOU! ”

Similar presentations



















 on the Efficacy.>")


 Cumulative incidence of distant metastases (ITT) Adapted from Jones et al. SABCS 2008, abstract 15. 486826/477169/465253/454771/4406110/4146.>")


:>")








 on Aromatase Inhibitor-Associated Bone Loss in Postmenopausal Women with Early Breast Cancer Receiving Adjuvant Letrozole:>")
