Download presentation
Presentation is loading. Please wait.

1
Angiographic V/s Functional Severity of Cor A Stenoses in the FAME Study FFR v/s CAG in Multivessel Evaluation JAmCollCardiol2010;55:2816–21 Tonino, Fearon et al. Frijo Jose A

2
Objectives To investigate the relationship between angiographic and functional severity of cor A stenoses in the FAME study

3
Background CAG may result in both underestimation & overestimation of a lesion’s severity & is often inaccurate in predicting which lesions cause ischemia

4
Principle FFR valueof 90%

5
Fractional flow reserve – During maximum vasodilation – Mean cor pressure/mean Ao pressure – Unaffected by alteration in resting flow – Can immediately assess importance of a lesion for guiding intervention – Considerable prognostic information – FFR more than 0.8- excellent outcome with deferred rather than prophylactic intervention – Most direct way to assess physiological significance of a lesion

6
Clinical uses of FFR 1. Determining the hemodynamic significance of CAG intermediate lesions: Pijls et al - cutoff 0.75 detected ischemia – sensitivity- 88%, specificity- 100%, diagnostic accuracy- 93% DEFER - moderate CAD + FFR>0.75 - PCI v/s medical – PCI event rate > medical event rate

7
Clinical uses of FFR 2. Determining success of PCI: Multicenter registry - FFR determined immediately after stenting – most signi independent variable related to future events

8
Clinical uses of FFR 3. Determining significance of LMCA lesions: Bech et al- 54pts (29/12)- equivocal LMCA Medical - 24 pts with FFRs >0.75 CABG - 30 pts with FFR <0.75 Survival – medical- 100%, CABG- 97%
- equivocal LMCA Medical - 24 pts with FFRs >0.75 CABG - 30 pts with FFR <0.75 Survival – medical- 100%, CABG- 97%.")
9
Clinical uses of FFR 4. Determining the significance of multiple stenoses in the same coronary artery: FFR can be used to “map” the hemodynamic effects of multiple stenoses in the same vessel FAME

10
Recommendations for Use of Fractional Flow Reserve Class IIa Can be useful to determine whether PCI of a specific cor lesion is warranted Can be useful as an alternative to performing noninvasive functional testing (eg, when the functional study is absent or ambiguous) to determine whether an intervention is warranted In the assessment of the effects of intermediate cor stenoses (30% to 70% luminal narrowing) in pts with anginal symptoms
 to determine whether an intervention is warranted In the assessment of the effects of intermediate cor stenoses (30% to 70% luminal narrowing) in pts with anginal symptoms")
11
Inclusion Mul-tivessel CAD, defined as cor A stenoses of ≥50% of vessel diameter in ≥2 of 3 major epicardial cor A, & if PCI was indicated

12
Exclusion Left main coronary disease Previous CABG Recent STEMI(<5days) Recent N-STEMI( 1000IU Cardiogenic shock Extremely tortuous/calcified cor Lifeexpectancy <2y Pregnancy Contraindication for DES placement
 Recent N-STEMI( 1000IU Cardiogenic shock Extremely tortuous/calcified cor Lifeexpectancy <2y Pregnancy Contraindication for DES placement")
15
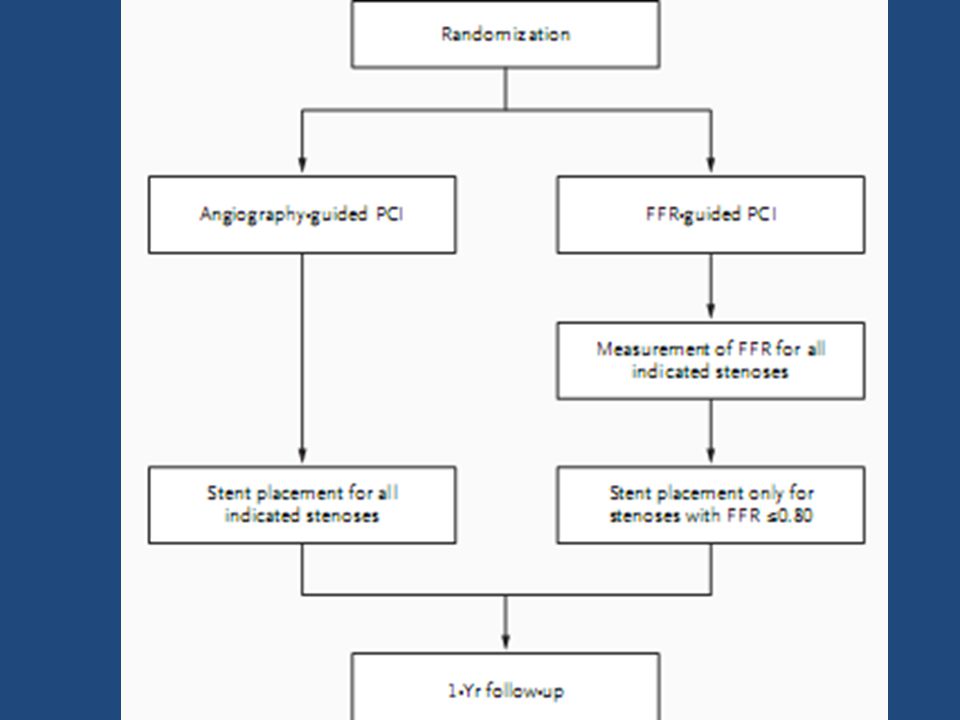
In this subanalysis of the FAME study, the relationship between CAG & FFR in all pts in the FFR-guided arm ( 509) was analyzed 1,005 pts with multi vessel disease were randomly assigned to CAG –guided PCI ( 496) or FFR-guided PCI ( 509)
 was analyzed 1,005 pts with multi vessel disease were randomly assigned to CAG –guided PCI ( 496) or FFR-guided PCI ( 509)")
16
Categorized the lesions according to visual CAG stenosis severity into 50%to70%, 71%to90%, & 91%to100% diameter stenosis In those randomized to FFR guidance, if the FFR of a particular stenosis was >0.80, -was considered as functionally nonsignificant & no stent was placed The definition of functional 0-,1-,2-,or3-VD was made on basis of no of main arteries with an FFR <0.80 So, a pt with CAG 3- VD could be classified as having functional 0-,1-,2-,or3-VD, after FFR

17
Serial stenoses Stenting is only performed if FFR beyond all narrowings is≤0.80 Investigator then stents the narrowing that appears most signi or is responsible for largest P gradient during pullback of P sensor After stenting 1 st lesion, FFR is measured again & any residual narrowing causing an FFR ≤0.80 is stented IV adenosine as opposed to intra-coronary adenosine because IV adenosine provides prolonged hyperemia, which allows adequate time to perform a pullback of the pressure wire and localize pressure gradients

18
In all FFR-guided pts, investigator is encouraged to measure a final FFR aft PCI Although the final FFR measurement can be quite useful for assessing PCI result, it is not mandated in protocol in an attempt to keep the procedure as simple as possible

19
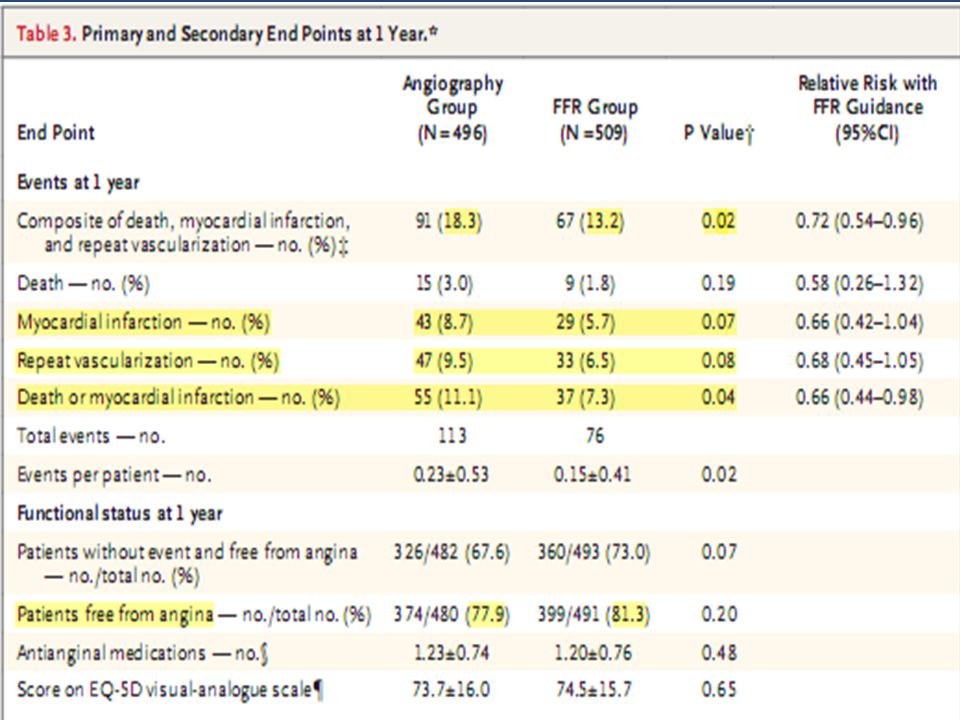
primary end point (1yr) Rate of death Nonfatal myocardial infarction Repeat revascularization
 Rate of death Nonfatal myocardial infarction Repeat revascularization")
20
In pts presenting with a NSTEMI & ↑CK-MB before PCI, if peak CK-MB has not occurred, a periprocedural MI will be defined as – Recurrent chest pain lasting for ≥30 m OR new ECG changes consistent with a 2 nd MI – & an ↑ in CK-MB by ≥50% of the preprocedure CK-MB level If the pre-PCI CK-MB is falling or already N, then a periprocedural MI will be defined as a CK-MB ↑ ≥3 times upperlimit of N & a 50% ↑from pre-PCI CK-MB level

21
Results FFR-guided arm of the FAME study -509 pts 1,414 lesions –indicated before randomization –FFR was measured successfully in 1,329(94%) of the 1,414 lesions 620(47%) - 50%to70%category 513(39%) - 71%to90%category 196(15%) - 91%to99%category
 of the 1,414 lesions 620(47%) - 50%to70%category 513(39%) - 71%to90%category 196(15%) - 91%to99%category")
22
Of all 1,329 lesions, 816(61%) were below ischemic threshold (FFR ≤0.80) Of 50%to70% category, in 402(65%), FFR was >0.80 and in 218(35%), FFR was ≤0.80 Of 71%to90% category, in104(20%), FFR was >0.80 and in 409(80%), FFR was ≤0.80 In 91%to99% category,7(4%) FFR >0.80 and 189(96%) had FFR ≤0.80
 were below ischemic threshold (FFR ≤0.80) Of 50%to70% category, in 402(65%), FFR was >0.80 and in 218(35%), FFR was ≤0.80 Of 71%to90% category, in104(20%), FFR was >0.80 and in 409(80%), FFR was ≤0.80 In 91%to99% category,7(4%) FFR >0.80 and 189(96%) had FFR ≤0.80")
25
Discussion All stenoses with CAG severity 50%to70%, 65% - functionally nonsigni & 35% - functionally signi by FFR In more severe stenoses 71%-90% CAG severity- 20% did not induce reversible myo ischemia as established by FFR

27
In pts with multivessel CAD, routine measurement of FFR during PCI, as compared with the standard strategy of PCI guided by CAG, signi ↓ rate of 1˚composite end point of death, MI, & repeat revasc at 1 year The combined of death & MI was also signi ↓ Without prolonging the procedure, the FFR- guided strategy ↓the no of stents used, ↓ the amount of contrast agent used

30
Diabetic Atherosclerosis Prevention by Cilostazol (DAPC) Study Katakami, Young-SeolKim et al. Circulation.2010;121:2584-2591

31
Background Anti-platelet drugs are effective in preventing recurrence of atherosclerosis in T2 DM. However, the efficacy & usefulness of 2 different antiplatelet drugs, aspirin and cilostazol, in the progression of carotid intima- media thickening are unknown.

32
Aim To compare cilostazol and aspirin in prevention of progression of atherosclerosis

33
T2-DM aged 40-85years at the time of enrollment who were suspected of having PAD on the basis of an ABI of <1.0, poor pulsation bilaterally or substantially weaker pulsation on either side in the case of the popliteal artery or dorsalis pedis artery, and/or clinical symptoms of PAD

34
329 type2 DM suspected of PAD were allocated to either Aspirin-treated(81to100mg/d)group - 152 Cilostazol-treated(100to200mg/d)gp-145 The changes in intima-media thickness of the common carotid artery during a 2-year observation period were examined as the primary endpoint
group Cilostazol-treated(100to200mg/d)gp-145 The changes in intima-media thickness of the common carotid artery during a 2-year observation period were examined as the primary endpoint")
35
Results In pts in cilostazol gp, there was signi improvement in max & mean left CCA-IMT during treatment compared with baseline; max & mean right CCA-IMT also exhibited a tendency toward improvement In pts in the aspirin gp- there was signi ↑in max left, max right, and mean right CCA-IMT from baseline

36
Conclusions Compared with ASA, cilostazol potently inhibited progression of carotid IMT, an established surrogate marker of CV events, in pts with type2 DM

38
Effects of Intensive BP Control in T-2 DM ACCORD-BP Cushman, Evans et al. N Engl J Med 2010;362:1575-85.

39
Background There is no evidence from randomized trials to support a strategy of lowering SBP <135 to 140 mm Hg in persons with T2DM

40
Aim Whether therapy targeting normal SBP (i.e., <120 mm Hg) ↓ major cardiovascular events in participants with type 2 diabetes at high risk for cardiovascular events
 ↓ major cardiovascular events in participants with type 2 diabetes at high risk for cardiovascular events")
41
4733 type 2 DM Intensive therapy- SBP-< 120 mm Hg Standard therapy- SBP-< 140 mm Hg

42
The ACCORD BP trial was a study of a treatment strategy to achieve specific SBP goals, rather than an evaluation of any specific drug regimen

43
Type 2 diabetes mellitus and a glycated hemoglobin level of 7.5% or more And were ≥40 yrs with CV disease or ≥55 yrs with anatomical evidence of a substantial amount of atherosclerosis, albuminuria, LVH, or at least two additional risk factors for CVD (DLP, HTN, smoking, or obesity)
")
44
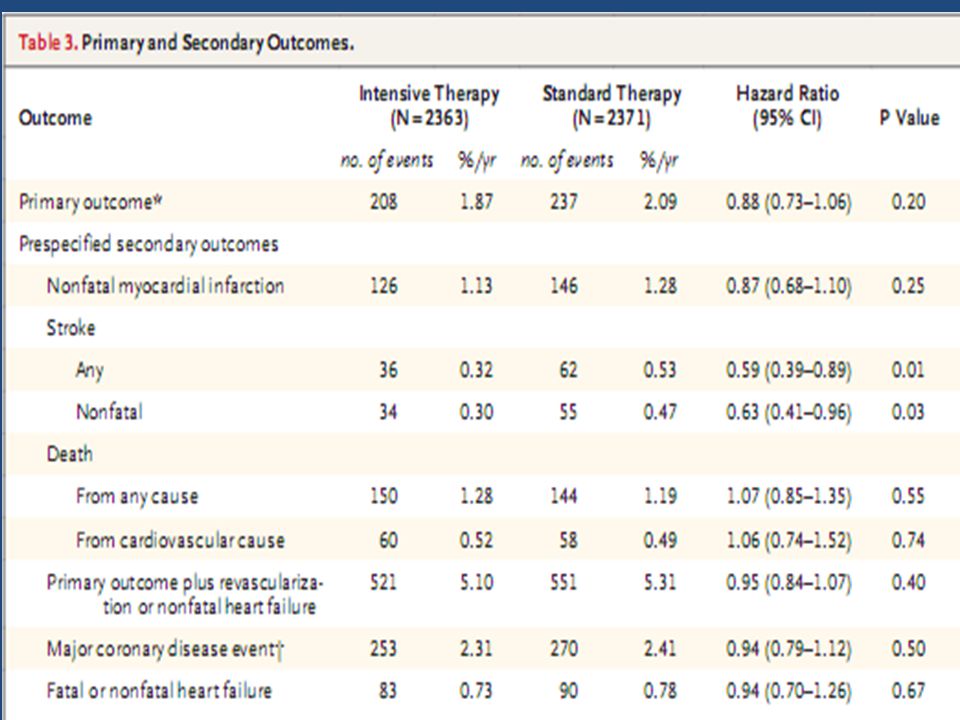
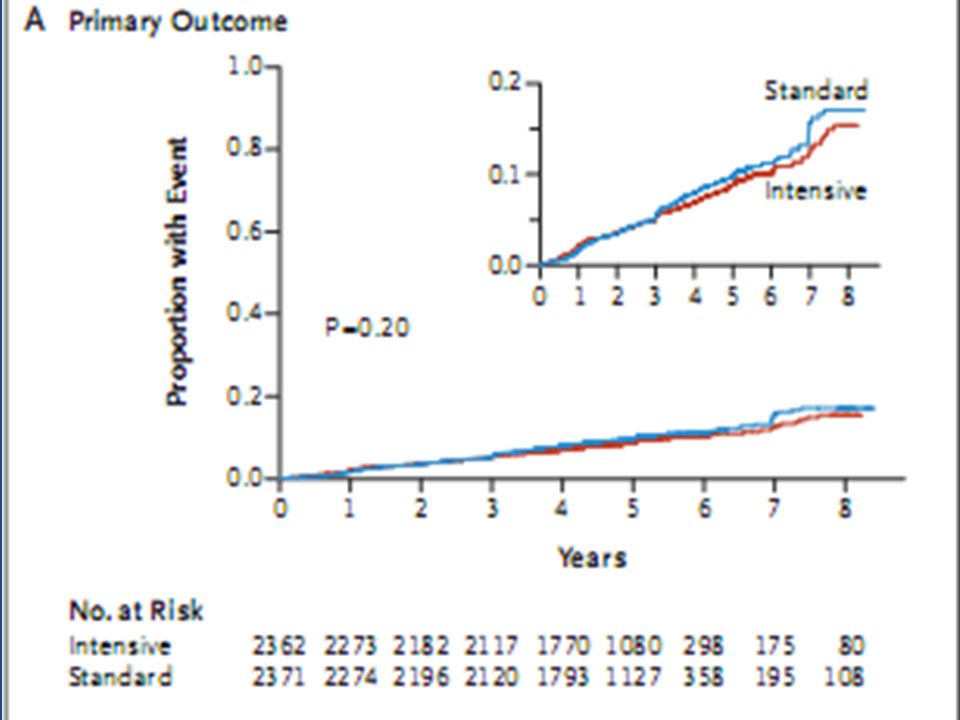
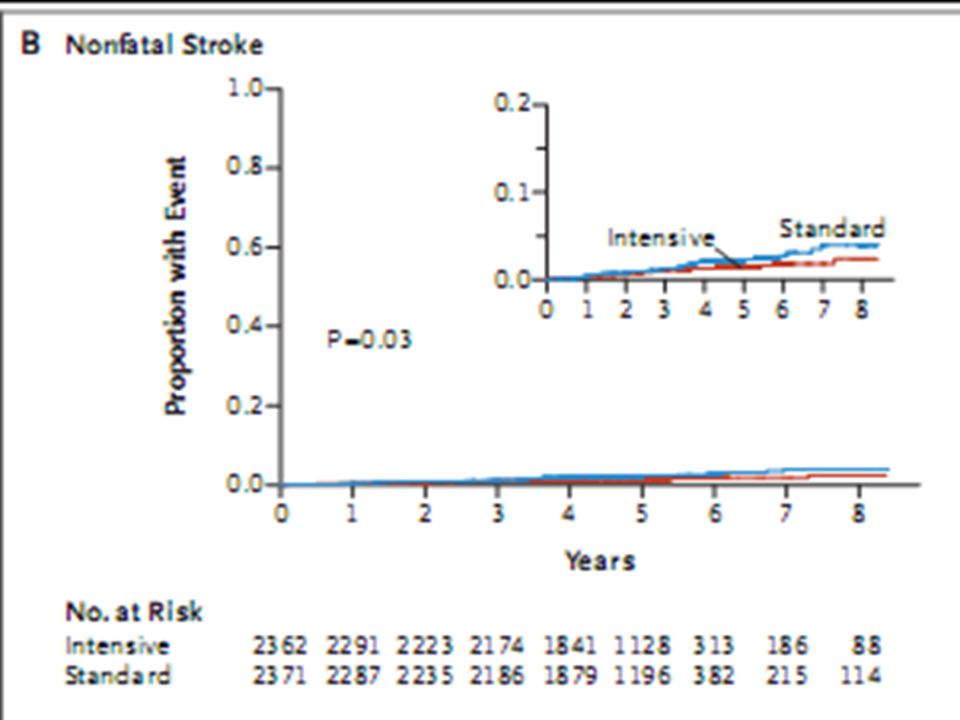
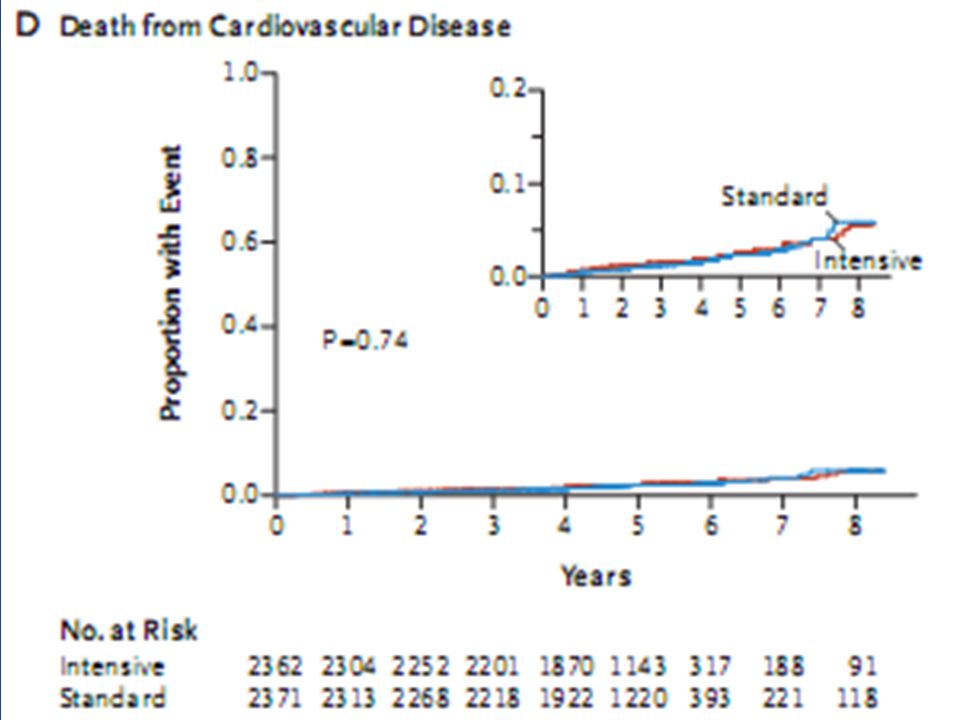
Primary composite outcome nonfatal MI, nonfatal stroke, or death from CV causes The mean follow-up - 4.7 years

45
Results Mean SBP- 119.3 mm Hg intensive & 133.5 mm Hg standard Annual rate of primary outcome - 1.87% (intensive) & 2.09% (standard), P = 0.20) Annual rates of death from any cause -1.28% and 1.19% ; P = 0.55 Annual rates of stroke- 0.32% and 0.53% ; P = 0.01 Serious adverse events attributed to anti-HTN treatment -77 of 2362 (intensive-3.3%) and 30 of 2371 (standard-1.3%)- P<0.001
 & 2.09% (standard), P = 0.20) Annual rates of death from any cause -1.28% and 1.19% ; P = 0.55 Annual rates of stroke- 0.32% and 0.53% ; P = 0.01 Serious adverse events attributed to anti-HTN treatment -77 of 2362 (intensive-3.3%) and 30 of 2371 (standard-1.3%)- P<0.001")
52
Conclusions In pts with T2 DM at high risk for CV events, targeting a SBP of <120 mm Hg, as compared with <140 mm Hg, did not reduce rate of a composite outcome of fatal & nonfatal major cardio-vascular events.

Similar presentations












>")











 Trial Basel Stent Cost-effectiveness Trial-Late Thrombotic Events (BASKET LATE)>")
>")


