Download presentation
Presentation is loading. Please wait.

1
HEAPHY 1 & 2 DIAGNOSTIC Deborah McKELLAR Fri 30 th Aug 2013 Session 2 / Talk 2 11:05 – 11:22 ABSTRACT This presentation will give a brief outline of the reasons SLT’s perform VFSS and what we aim to achieve. We will explore the clinical view required and some of the barriers to achieving this. Case studies will be presented.

2
Videofluoroscopy Study of Swallowing (VFSS) Deborah McKellar Clinical Leader Speech Language Therapy Waikato Hospital
 Deborah McKellar Clinical Leader Speech Language Therapy Waikato Hospital")
3
What do SLT’s do? Communication Swallowing –Assessment –Advice/recommendations –Rehabilitation

4
Swallowing Assessments “Bedside” assessment –Silent aspiration risk Objective assessment –FEES (fiberoptic endoscopic evaluation of swallowing) –VFSS (videofluoroscopic study of swallowing)
 –VFSS (videofluoroscopic study of swallowing)")
5
FEES

6
Videofluoroscopic Study of Swallowing Sometimes referred to as Modified Barium Swallow

7
VFSS

8
VFSS vs Barium Swallow VFSS –Focus on anatomy and physiology of oral, pharyngeal, laryngeal and upper oesophageal parameters. –Uses a variety of foods, fluids and strategies. –Performed by radiologist and/or SLT. Barium swallow –Examines the upper gastrointestinal tract focusing on esophagus and stomach. –Identifies motility issues or structural abnormalities in the oesophagus. –Performed by radiologist.

9
Why do we do VFSS? Investigate cause/physiology of dysphagia To guide dysphagia rehabilitation Assess for aspiration risk – silent aspiration Where clinical condition does not match the clinical swallowing evaluation Not everyone with dysphagia needs a VFSS

10
What we do? Trial a variety of consistencies of food/fluid Trial strategies e.g. chin tuck, head turn Trial different delivery methods Assess fatigue effects

11
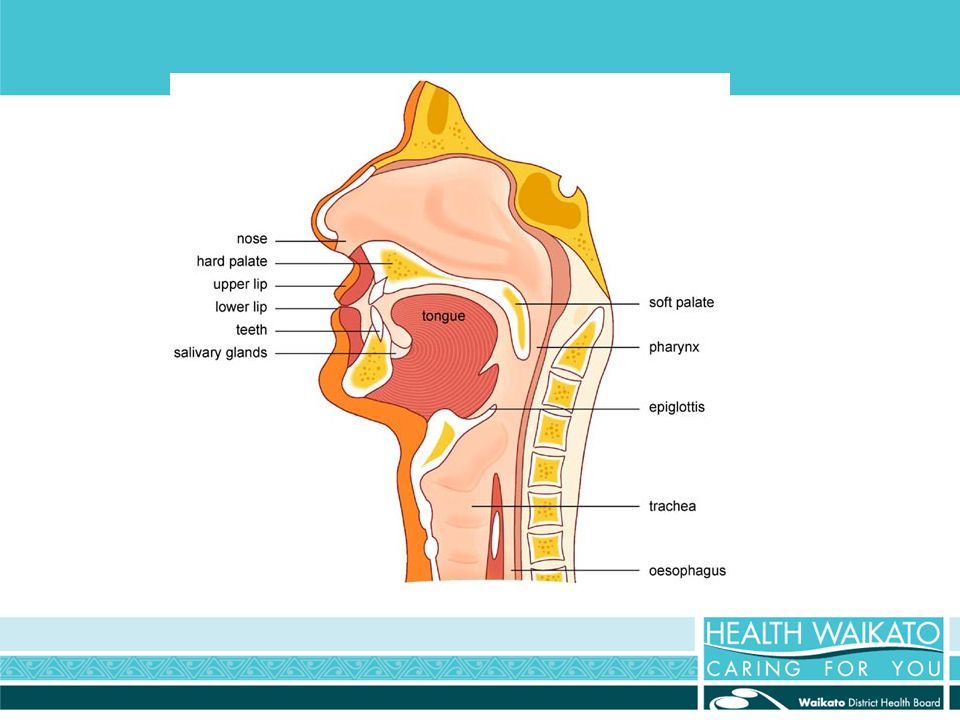
What are we looking at? Oral parameters Oral transit parameters Pharyngeal parameters Crico-oesophogeal parameters Laryngeal parameters

13
A normal swallow

14
What do we look for? Aspiration – before, during or after the swallow Difficulty controlling food/fluid in the mouth Difficulty initiating the swallow Residue after the swallow – unable to clear pharynx

15
Aspiration Not an automatic reason to stop the procedure “a degree of aspiration may be necessary in order to gain a clear assessment of swallow physiology” May need to trial other strategies and consistencies

16
What do we need to see? Need to view mouth, pharynx, laryngx and upper oesophagus Need to see the start of the swallow Often will need to keep screening after the swallow AP view is often required – symmetry Oesophageal screen

17
Limitations Patient mobility/sitting balance Patient co-operation Equipment logistics Shoulders

18
NZSTA recommendations Must have a swallowing/feeding evaluation before the VFSS SLTs should have access to high quality images and slow motion playback SLTs are not qualified to make medical diagnosis or identify structural deviations

19
Videopalatogram Looks at palate movement (velopharyngeal closure) during speech Small amount of barium squirted into patient’s nose to coat structures Synched speech and video required Aids in decisions regarding palate surgery (surgery vs speech therapy)
 during speech Small amount of barium squirted into patient’s nose to coat structures Synched speech and video required Aids in decisions regarding palate surgery (surgery vs speech therapy)")
20
NZSTA Clinical Practice Guideline on Videofluoroscopic Study of Swallowing (VFSS) April 2011 The Dynamic Swallow DVD
 April 2011 The Dynamic Swallow DVD")
Similar presentations







 833-2090 www. med-speech.com.>")











; PGD (BIOETHICS)>")