Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2010 年 11 月 25 日 8:30-8:55 8階 医局 Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H, Vincent J, Pocock SJ, Pitt B; the EMPHASIS-HF Study Group. Eplerenone in Patients with Systolic Heart Failure and Mild Symptoms. N Engl J Med. 2010 Nov 14. [Epub ahead of print] 10.1056/nejmoa1009492 Brad P. Barnett, Yousang Hwang, Martin S. Taylor, Henriette Kirchner, Paul T. Pfluger, Vincent Bernard, Yu-yi Lin, Erin M. Bowers, Chandrani Mukherjee, Woo- Jin Song, Patti A. Longo, Daniel J. Leahy, Mehboob A. Hussain, Matthias H. Tschöp, Jef D. Boeke, Philip A. Cole Glucose and Weight Control in Mice with a Designed Ghrelin O-Acyltransferase Inhibitor 10.1126/science.1196154

2
Rates of Hyperkalemia ( >5.5 mEq/L) in EPHESUS by Proteinuria and History of Diabetes* Eplerenone (N=508) n (%) Placebo (N=363) n (%) ** Diabetes assessed as positive medical history at baseline; proteinuria assessed by positive dipstick urinalysis at baseline. Rates of Hyperkalemia ( >5.5 mEq/L) in EPHESUS by Proteinuria and History of Diabetes**
 in EPHESUS by Proteinuria and History of Diabetes**.")
3
INSERM, Centre d’Investigation Clinique 9501 and Unite 961, Centre Hospitalier Universitaire, and the Department of Cardiology, Nancy University, Nancy, France (F.Z.); the British Heart Foundation Cardiovascular Research Centre, University of Glasgow, Glasgow, United Kingdom ( J.J.V.M.); the Department of Epidemiology and Preventive Medicine, Centre of Cardiovascular Research and Education in Therapeutics, Monash University, Melbourne, VIC, Australia (H.K.); the Department of Cardiology, Thorax Center, University Medical Center, Groningen, the Netherlands (D.J.V.); the Department of Emergency and Cardiovascular Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden (K.S.); Pfizer, New York (H.S., J.V.); the Department of Medical Statistics, London School of Hygiene and Tropical Medicine, London (S.J.P.); and University of Michigan School of Medicine, Ann Arbor (B.P.). 10.1056/nejmoa1009492 nejm.orgN Engl J Med 2010.

4
Mineralocorticoid antagonists improve survival among patients with chronic, severe systolic heart failure and heart failure after myocardial infarction. We evaluated the effects of eplerenone in patients with chronic systolic heart failure and mild symptoms. BACKGROUND

5
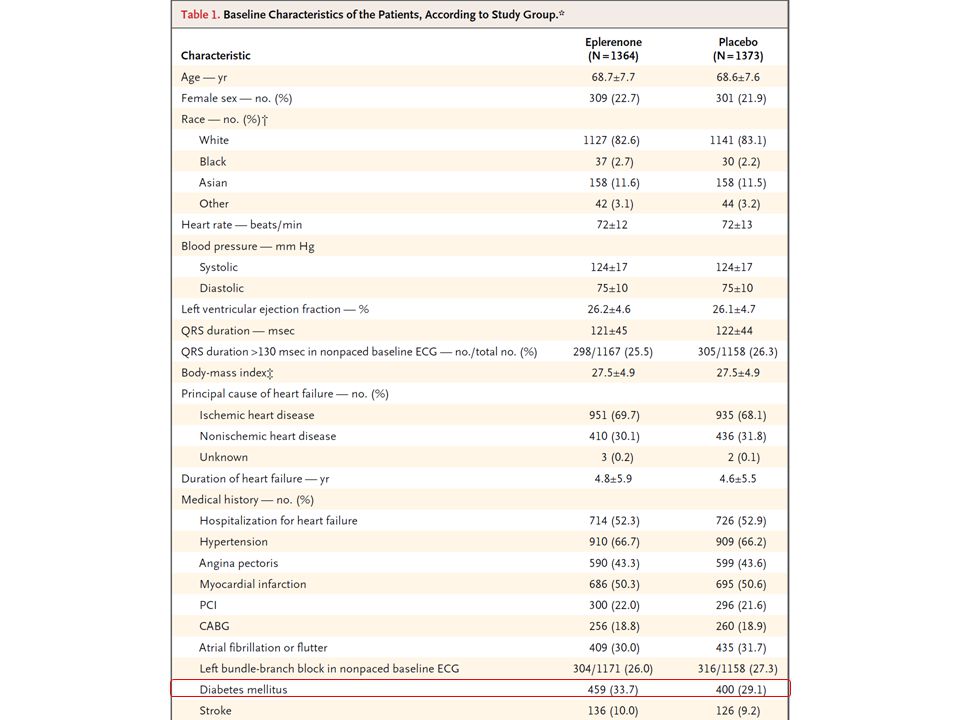
In this randomized, double-blind trial, we randomly assigned 2737 patients with New York Heart Association class II heart failure (mild symptoms) and an ejection fraction of no more than 35% to receive eplerenone (up to 50 mg daily) or placebo, in addition to recommended therapy. The primary outcome was a composite of death from cardiovascular causes or hospitalization for heart failure. METHODS

7
We attempted to minimize the risk of hyperkalemia by excluding patients with a baseline serum potassium level above 5.0 mmol per liter and a baseline estimated GFR below 30 ml per minute per 1.73 m 2. Eplerenone was started at a dose of 25 mg once daily and was increased after 4 weeks to 50 mg once daily (or started at 25 mg on alternate days, and increased to 25 mg daily.

10
Figure 2. Hazard Ratios for Hospitalization for Heart Failure or Death from Cardiovascular Causes (the Primary Outcome) with Eplerenone versus Placebo, According to Prespecified Subgroups. The subgroups are based on baseline demographic and clinical characteristics. The size of the square corresponds to the number of patients with an event. Data are missing for some patients in some subgroups. ACE denotes angiotensin- converting enzyme, ARB angiotensin- receptor blocker, BNP B-type natriuretic peptide, CRT cardiac-resynchronization therapy, GFR glomerular filtration rate, ICD implantable cardioverter–defibrillator, and LVEF left ventricular ejection fraction.
 with Eplerenone versus Placebo, According to Prespecified Subgroups. The subgroups are based on baseline demographic and clinical characteristics. The size of the square corresponds to the number of patients with an event. Data are missing for some patients in some subgroups. ACE denotes angiotensin- converting enzyme, ARB angiotensin- receptor blocker, BNP B-type natriuretic peptide, CRT cardiac-resynchronization therapy, GFR glomerular filtration rate, ICD implantable cardioverter–defibrillator, and LVEF left ventricular ejection fraction..")
12
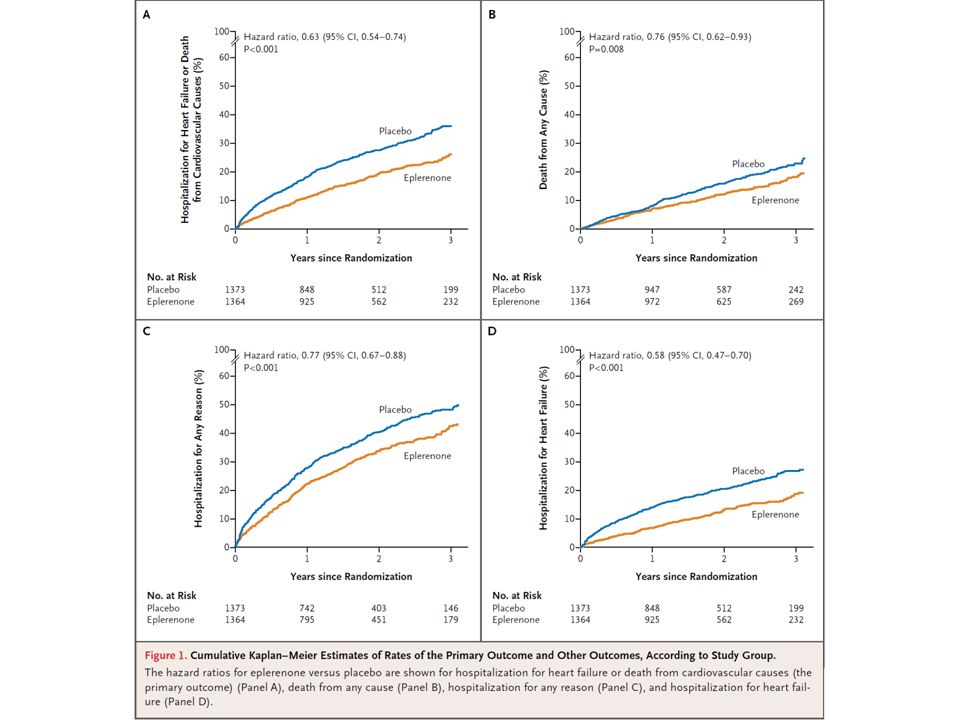
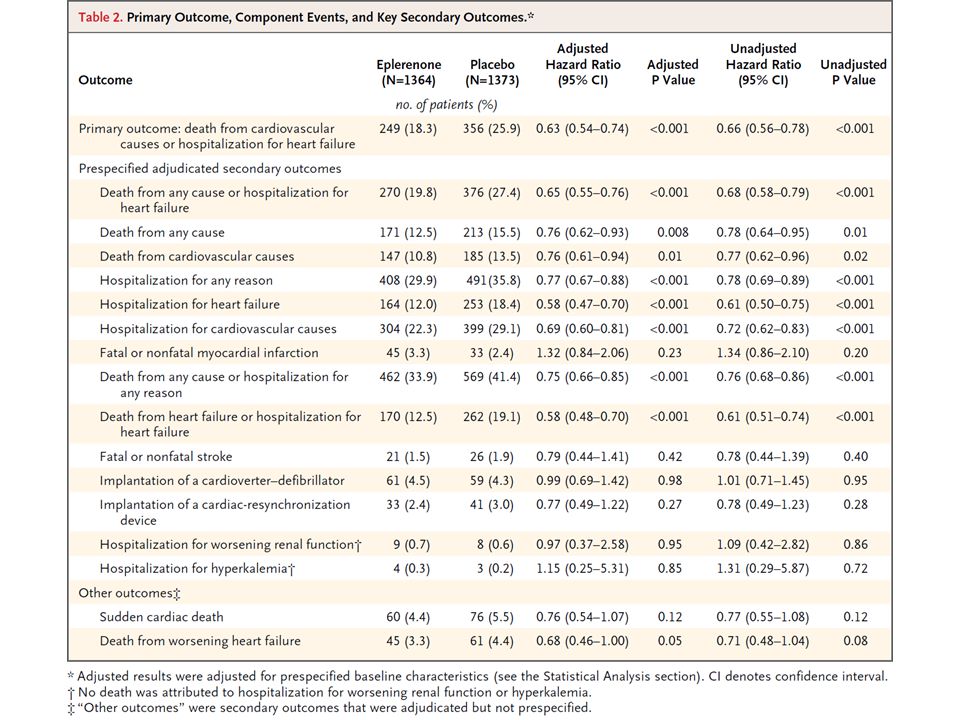
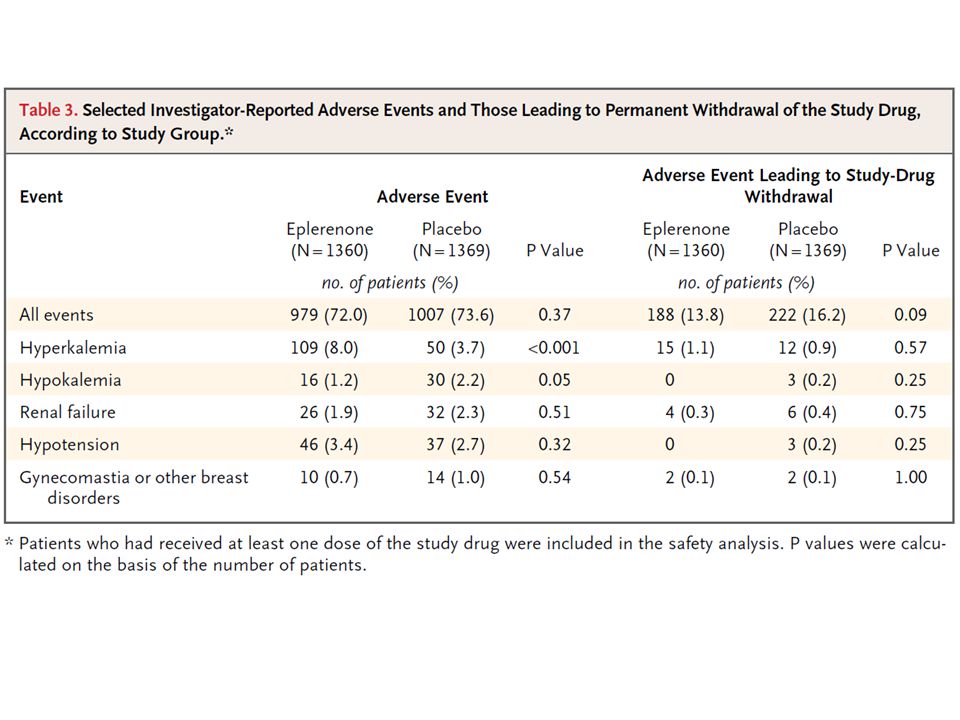
The trial was stopped prematurely, according to prespecified rules, after a median follow-up period of 21 months. The primary outcome occurred in 18.3% of patients in the eplerenone group as compared with 25.9% in the placebo group (hazard ratio, 0.63; 95% confidence interval [CI], 0.54 to 0.74; P<0.001). A total of 12.5% of patients receiving eplerenone and 15.5% of those receiving placebo died (hazard ratio, 0.76; 95% CI, 0.62 to 0.93; P = 0.008); 10.8% and 13.5%, respectively, died of cardiovascular causes (hazard ratio, 0.76; 95% CI, 0.61 to 0.94; P = 0.01). Hospitalizations for heart failure and for any cause were also reduced with eplerenone. A serum potassium level exceeding 5.5 mmol per liter occurred in 11.8% of patients in the eplerenone group and 7.2% of those in the placebo group (P<0.001). RESULTS
. A total of 12.5% of patients receiving eplerenone and 15.5% of those receiving placebo died (hazard ratio, 0.76; 95% CI, 0.62 to 0.93; P = 0.008); 10.8% and 13.5%, respectively, died of cardiovascular causes (hazard ratio, 0.76; 95% CI, 0.61 to 0.94; P = 0.01). Hospitalizations for heart failure and for any cause were also reduced with eplerenone. A serum potassium level exceeding 5.5 mmol per liter occurred in 11.8% of patients in the eplerenone group and 7.2% of those in the placebo group (P<0.001). RESULTS.")
13
CONCLUSIONS Eplerenone, as compared with placebo, reduced both the risk of death and the risk of hospitalization among patients with systolic heart failure and mild symptoms. (Funded by Pfizer; ClinicalTrials.gov number, NCT00232180.)
.")
14
Message/Comments 糖尿病では高カリウム血症という副作用で 使いにくいが心不全にはよい薬物。(アク トスとの併用?)
")
16
www.sciencexpress.org / 18 November 2010 / Page 1 / 10.1126/science.1196154

17
Background: Ghrelin is a gastric peptide hormone that stimulates weight gain in vertebrates. The biological activities of ghrelin require octanoylation of the peptide on Ser3, an unusual post-translational modification that is catalyzed by the enzyme ghrelin O-acyltransferase (GOAT).
..")
18
Methods: Here, we describe the design, synthesis, and characterization of GO-CoA-Tat, a peptide-based bisubstrate analog that antagonizes GOAT. GO-CoA-Tat potently inhibits GOAT in vitro, in cultured cells, and in mice.

19
Fig. 1. GO-CoA-Tat is a bisubstrate inhibitor that inhibits GOAT, lowering acyl ghrelin levels. (A) Mechanism-based design strategy. Lipid-enzyme interaction, not shown, may also be important. (B) Structure of GO-CoA-Tat and synthetic scheme for bisubstrate inhibitors that consist of three components: coenzyme A, octanoylated ghrelin peptide and a Tat peptide; Ahx-aminohexanoate. (C) Temporal inhibition of acyl but not desacyl ghrelin production by 6 μM GO-CoA- Tat in GOAT/preproghrelin- transfected HeLa cells. (D) Dose-response reduction of acyl but not desacyl ghrelin levels by GO-CoA-Tat in GOAT/preproghrelin- transfected HeLa cells after 24 h incubation.
 Mechanism-based design strategy. Lipid-enzyme interaction, not shown, may also be important. (B) Structure of GO-CoA-Tat and synthetic scheme for bisubstrate inhibitors that consist of three components: coenzyme A, octanoylated ghrelin peptide and a Tat peptide; Ahx-aminohexanoate. (C) Temporal inhibition of acyl but not desacyl ghrelin production by 6 μM GO-CoA- Tat in GOAT/preproghrelin- transfected HeLa cells. (D) Dose-response reduction of acyl but not desacyl ghrelin levels by GO-CoA-Tat in GOAT/preproghrelin- transfected HeLa cells after 24 h incubation..")
20
Fig. 2. GO-CoA-Tat targets GOAT directly in vitro and in a structure specific manner. (A) Structure of GO-CoA-Tat analogs (1–6). (B) Acyl and desacyl ghrelin levels after treatment with 6 μM GO-CoA-Tat (1) and analogs (2–6) from GOAT/preproghrelin- transfected HeLa cells after 24 h. (C) In vitro acyltransferase inhibition assay (5 min reaction) with microsomal recombinant GOAT. (D) UV crosslinking of solubilized GOAT by biotin- tagged, benzophenylalanine analogs of GO-CoA-Tat (L5BP, F4BP) (5 μM). Competitor is GO-CoA-Tat at 100 μM. Immunoblots of cross-linked GOAT were visualized with streptavidin, loading was checked with anti-FLAG.
 Structure of GO-CoA-Tat analogs (1–6). (B) Acyl and desacyl ghrelin levels after treatment with 6 μM GO-CoA-Tat (1) and analogs (2–6) from GOAT/preproghrelin- transfected HeLa cells after 24 h. (C) In vitro acyltransferase inhibition assay (5 min reaction) with microsomal recombinant GOAT. (D) UV crosslinking of solubilized GOAT by biotin- tagged, benzophenylalanine analogs of GO-CoA-Tat (L5BP, F4BP) (5 μM). Competitor is GO-CoA-Tat at 100 μM. Immunoblots of cross-linked GOAT were visualized with streptavidin, loading was checked with anti-FLAG..")
21
Fig. 3. Effects of GO-CoA-Tat on blood ghrelin and body weight in mice. (A) Serum acyl ghrelin levels in WT C57BL6 mice on an MCT diet treated intraperitoneally with 11 μmol/kg GO-CoA-Tat vs. D4- Tat control (n = 5) after 6, 12, and 24 h. (*P 0.2), nor reproducible in other experiments. (B) Serum desacyl ghrelin levels for experiment in Fig. 3A. (C) Percent acyl ghrelin for experiment in Fig. 3A.
 Serum acyl ghrelin levels in WT C57BL6 mice on an MCT diet treated intraperitoneally with 11 μmol/kg GO-CoA-Tat vs. D4- Tat control (n = 5) after 6, 12, and 24 h. (*P 0.2), nor reproducible in other experiments. (B) Serum desacyl ghrelin levels for experiment in Fig. 3A. (C) Percent acyl ghrelin for experiment in Fig. 3A..")
22
Fig. 3. Effects of GO-CoA-Tat on blood ghrelin and body weight in mice. (D) Body weights in wt C57BL6 mice on an MCT diet treated with 11 μmmol/kg GO- CoA-Tat (red, n = 5) or vehicle (black, n = 6) for 1 mo (*P < 0.05; conventional ** and *** omitted for clarity, standard errors shown). (E) Fat mass in wt mice measured by QMR for experiment in 3D. (F) Body weights in ghrelin knockout C57BL6 mice on an MCT diet treated with 11 μmol/kg GOCoA- Tat (red, n = 5) or vehicle (black, n = 5) for 1 mo (standard errors shown). The larger error bars compared to data in Fig. 3D likely represent the broader distribution of starting weights. Also note that the scales differ in the two panels, contributing to the larger error bars seen here. (G) Fat mass in ghrelin knockout mice measured by QMR for experiment in Fig. 3F.
 Body weights in wt C57BL6 mice on an MCT diet treated with 11 μmmol/kg GO- CoA-Tat (red, n = 5) or vehicle (black, n = 6) for 1 mo (*P < 0.05; conventional ** and *** omitted for clarity, standard errors shown). (E) Fat mass in wt mice measured by QMR for experiment in 3D. (F) Body weights in ghrelin knockout C57BL6 mice on an MCT diet treated with 11 μmol/kg GOCoA- Tat (red, n = 5) or vehicle (black, n = 5) for 1 mo (standard errors shown). The larger error bars compared to data in Fig. 3D likely represent the broader distribution of starting weights. Also note that the scales differ in the two panels, contributing to the larger error bars seen here. (G) Fat mass in ghrelin knockout mice measured by QMR for experiment in Fig. 3F..")
23
Fig. 4. GO-CoA-Tat increases insulin, decreases glucose levels, and down-regulates islet cell UCP2 mRNA. (A) C57BL6 wt mice raised on normal mouse chow and treated with 8 μmol/kg GO-CoA-Tat (n = 4) experienced a statistically significant increase in insulin secretion and (B) a statistically significant decrease in blood glucose as compared to control mice (treated with D4-Tat (n = 4)) when compound was administered 24 h prior to IP glucose challenge (2.5g/kg) (*P < 0.05, **P < 0.01, std. errors shown).
 C57BL6 wt mice raised on normal mouse chow and treated with 8 μmol/kg GO-CoA-Tat (n = 4) experienced a statistically significant increase in insulin secretion and (B) a statistically significant decrease in blood glucose as compared to control mice (treated with D4-Tat (n = 4)) when compound was administered 24 h prior to IP glucose challenge (2.5g/kg) (*P < 0.05, **P < 0.01, std. errors shown)..")
24
Fig. 4. GO-CoA-Tat increases insulin, decreases glucose levels, and down-regulates islet cell UCP2 mRNA. (C) Immunohistochemical staining of mouse islets. Left panel – insulin (green) ghrelin receptor (GHSR) (red) and cell nuclei stained with DAPI (blue). Middle panel – staining of islet for ghrelin (white) and insulin (green) demonstrates dual staining and ghrelin positive and insulin negative cells. Right panel – closeup of unmerged images in boxed area of middle panel. (D) QRT-PCR of islets and (E) gastric fundus isolated from mice treated with inhibitor 24 h prior to isolation and mRNA expression relative to control (n = 3).
 Immunohistochemical staining of mouse islets. Left panel – insulin (green) ghrelin receptor (GHSR) (red) and cell nuclei stained with DAPI (blue). Middle panel – staining of islet for ghrelin (white) and insulin (green) demonstrates dual staining and ghrelin positive and insulin negative cells. Right panel – closeup of unmerged images in boxed area of middle panel. (D) QRT-PCR of islets and (E) gastric fundus isolated from mice treated with inhibitor 24 h prior to isolation and mRNA expression relative to control (n = 3)..")
26
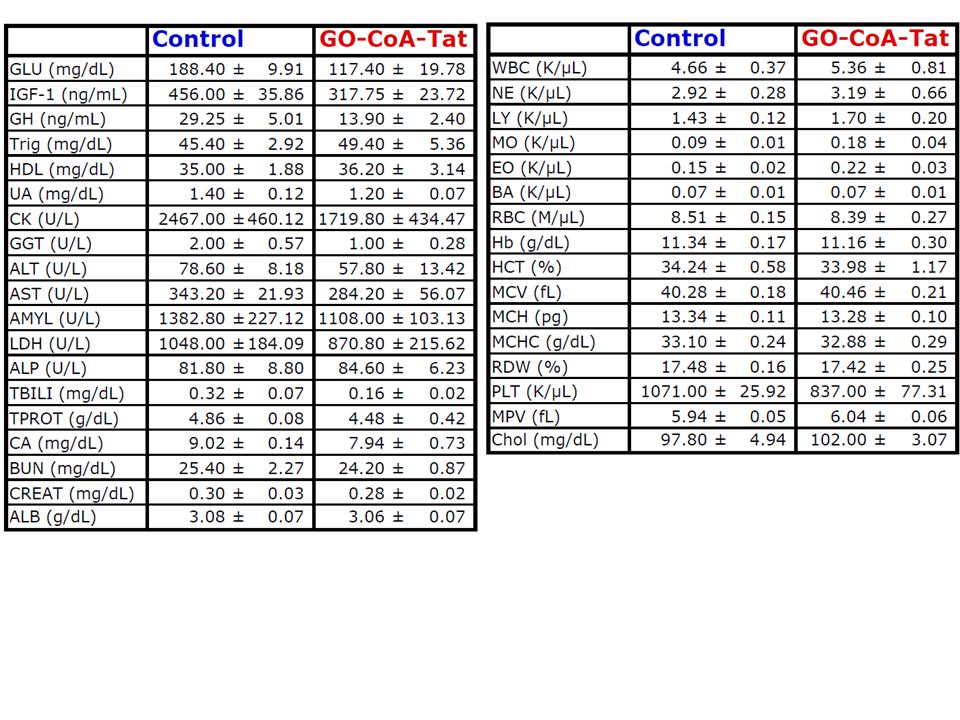
Results: Intraperitoneal administration of GO-CoA-Tat improves glucose tolerance and reduces weight gain in wild-type mice but not in ghrelin-deficient mice, supporting the concept that its beneficial metabolic effects are due specifically to GOAT inhibition.

27
Conclusion: In addition to serving as a research tool for mapping ghrelin actions, GO- CoA-Tat may help pave the way for clinical targeting of GOAT in metabolic diseases.

28
Message/Comments グレリン作用を抑制することで肥満治療が できる可能性がある。

Similar presentations



:>")
>")
















