Download presentation
Presentation is loading. Please wait.

1
Electrocardiogram Interpretation
ISMAIL HAMAM, MD DEPARTMENT OF CARDIOLOGY JORDAN UNIVERSITY HOSPITAL

2
Objectives To review Basic Concepts for the 12-Lead ECG
To know Normal Criteria for the ECG To perform a Systematic Approach to ECG Interpretation. To discuss a deferent Rhythms on the 12-Lead ECG

3
Basic Concepts The heart is a pump with an electrical conduction system 2 basic types of cardiac cells in the heart 1. Myocardial cells or “muscle” cells 2. Specialized cells of the conduction system or “pacemaker” cells

4
The Electrical Cycle 1.The S-A Node generates an action potential.
2. The action potential propagates in the atria and causes a contraction. It is also transmitted to the AV Node. 3.The action potential is delayed at the A-V Node. 4.The action potential is transmitted to the ventricles and causes contraction

5
The electrocardiogram (ECG) is a standardize way to measure and display the electrical activity of the heart. Physicians can diagnose problems with the heart by analyzing its ECG and comparing it to the ECG

6
12-lead ECG Simultaneous measurements from: – Three limb leads
– Three augmented limb leads – Six chest leads Process data from all leads to obtain ECG waveform

7
Structure of a 12-Lead Recording
The three standard or limb leads 1,2 and 3 have been in use since the late 1800’s, but the augmented limb leads aVR, aVL and aVF, and the precordial or chest leads V1-6 only came into use in the 1930’s. The six precordial electrodes create a six-lead image of the heart on the transverse plane .Each of the pericardial leads is unipolar (1 electrode constitutes a lead).
.")
8
Limb leads are three electrodes that are placed on the two arms and left leg create a 360o six-lead electrical image of the heart on the frontal plane on the ECG recording (1, 2, 3, aVR, aVL, aVF). The lead on the right leg is system ground. Accurate lead placement is important. Malposition can lead to significant interpretation errors, especially while comparing serial recordings from the same patient.

10
Limb Leads Lead Relative angle l: RA-LA 0° ll: RA-LL 60° lll: LA-LL
120°

11
Augmented Limb Leads: aVR = (LA-LL) vs. RA(+) aVL = (RA-LL) vs. LA(+)
aVF = (RA-LA) vs. LL(+)
 vs. LL(+)")
12
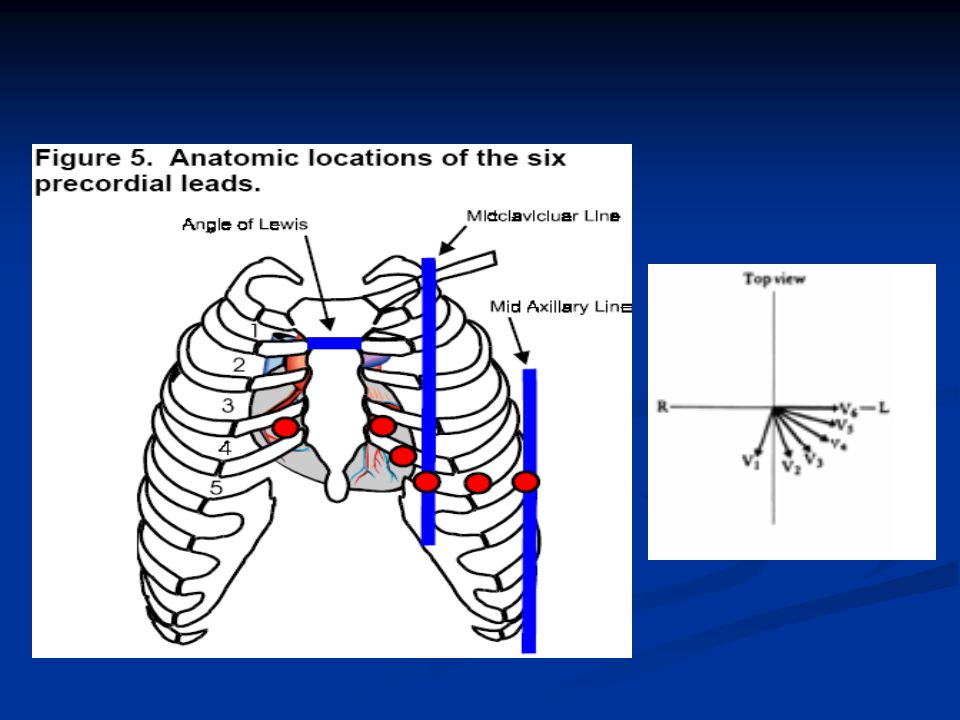
Locating the leads The four limb leads are placed on the four limbs.
V1 in the 4th intercostal space adjacent to the right sternum. V2 in the 4th intercostal space adjacent to the left sternum. V4 in the 5th intercostal space in the mid- clavicular line. V6 90o to the sternal axis at the same level as V4 and on the mid- axillary line. V3 halfway between V2 and V4. V5 halfway between V4 and V6, in the anterior axillary line.

14
Paper Speed and Voltages
Time is measured for cardiac heartbeats in milliseconds on the x-axis. The standard 12-lead recording is made with the paper running through the machine at rate of 25 mm/sec. This produces tracings along the X-axis with a duration of 40 msec/mm (“one small square”), or 200 msec for each 5 mm thick line (“one large square”) . Strength of the electrical signal from the heart is measured in millivolts on the y-axis. The ECG normally records a gain of 1 mV/cm on the Y-axis .
, or 200 msec for each 5 mm thick line ( one large square ) . Strength of the electrical signal from the heart is measured in millivolts on the y-axis. The ECG normally records a gain of 1 mV/cm on the Y-axis .")
15
paper Paper speed = 25mm / second Voltage Time .1 mv .5 mv .04 seconds

16
Standard 12-lead electrocardiogram

17
The ECG Complex Component Physiologic Correlation P wave
Atrial depolarization PR interval AV node refractory period PR segment Atrial repolarization QRS complex Ventricular depolarization J point End of ventricular depolarization ST segment Blood flow from the ventricles T wave Ventricular repolarization U wave Uncertain TP Segment Rest prior to next heartbeat cycle

18
Heart Excitation Related to ECG
SA node generates impulse; atrial excitation begins Impulse delayed at AV node Impulse passes to heart apex; ventricular excitation begins Ventricular excitation complete SA node AV node Bundle branches Purkinje fibers

19
Normal Criteria for the ECG
P wave ≤ 110 msec. <0.25 mvolts in the limb leads. Upright in 1, 2, aVF, V4-6. Inverted in aVR. Leads 1-3: single peak, or two peaks if they are < 40 msec apart. Second half in V1 positive.

20
PR interval PR segment 120 - 200 msec. Usually measure in lead 2.
Shorter at faster rates and younger persons. Longer in larger hearts and older persons. PR segment Usually isoelectric

21
QRS complex < 120 msec. And > 0.5 mV in all the limb leads.
> 1.0 mV in all of the precordial leads Measure in the lead with the longest QRS duration. Any initial upward deflection means that an R wave, not a Q wave, is present. R wave increases in amplitude across the precordial leads, usually becoming larger in voltage than the S wave in V2 - V4 (transition zone) in adult
 in adult.")
22
Limb lead QRS axis Net electrical vector of ventricular contraction -30o to +105o Overweight: more leftward, Thin: more rightward.

23
ST segment Usually within 1 mm of the isoelectric baseline.
Horizontal, with a smooth entry to the T wave. Limb leads: isoelectric in 75% of normal persons; in the remaining 25% slight elevation is more common. Precordial leads: slight elevation in 90% of normal persons, more common in men, usually in V2 and V3, where it can reach 3 mm. ST depression is rare in 1, 2, and aVF in normal persons, and is considered abnormal in the precordial lead

24
T wave < 0.5 mvolts in the limb leads.
< 1.0 mvolt in the chest leads. More gradual slope in the first half than the second half. Upright in 1, 2 and V4-6 , inverted in aVR, variable in all other leads. Upright, flat or slightly inverted in 3. Upright in aVL, aVF if QRS > 0.5 mV. Can be inverted in V1-2 in adult men, V1-3 in adult women (shallowly in V3). Always upright in V5-V6.
. Always upright in V5-V6.")
25
TP segment U wave QT interval
Varies with the heart rate, age and gender. Usually less than half the RR interval at normal sinus rates (65-90 bpm). TP segment Usually isoelectric Can be used as a baseline reference like the PR segment. U wave Usually 5-25% the amplitude of the T wave. Usually same polarity as the T wave.
. TP segment. Usually isoelectric. Can be used as a baseline reference like the PR segment. U wave. Usually 5-25% the amplitude of the T wave. Usually same polarity as the T wave.")
26
The Normal EKG (ECG)
")
27
A Systematic Approach to Electrocardiogram Interpretation.
Step 1 To know the age, gender and history of the patient Step 2 Standardization. Y-axis (voltage, normally one millivolt per cm X-axis (rate of recording, normally 25 mm/sec, or 200 msec/5 mm).
.")
28
Step 3 Rate. Calculate the rate by knowing that the Y-axis standardization is 25 mm/sec. One small square (1 mm) is 40 msec in duration. Therefore 2.5 cm represents one second.

29
Count the number of complexes across the 25 cm page (10 seconds), multiply by 6 and you get the average rate per one minute. This is a useful way to estimate rate for irregular features. Count the large squares between P waves for atrial rate and R waves for ventricular rate 300 ÷ number of large squares = number of beats/min

30
Step 4 Rhythm Identify P waves and QRS complexes.
Is the RR interval regular or irregular? Note whether the QRS complex is wide (> 3 mm or 120 msec) or narrow. Observe for -- rate, P wave and QRS complex synchrony, RR interval regularity, and width of the QRS complex – you can begin to sort out the rhythm. Look for extra complexes such as premature atrial, junctional and ventricular contractions.
 or narrow. Observe for -- rate, P wave and QRS complex synchrony, RR interval regularity, and width of the QRS complex – you can begin to sort out the rhythm. Look for extra complexes such as premature atrial, junctional and ventricular contractions.")
31
Normal sinus rhythm Rate 60 – 100 bpm Rhythm Regular
P wave Upright, normal P-R – 0.20 sec QRS – 0.12 sec P : QRS Rasio 1: 1

32
12 lead ECG

33
Step 5 Axis Each of the 12 leads on the ECG has a different pattern because each lead views the hearts electrical axis from a different position Atrial and ventricular depolarization and repolarization generate an electric current known as an electrical axis or vector (different from the axis of a lead) The electrical current of a heartbeat normally flows from the SA node into the ventricles, roughly toward the positive pole of lead 2. The normal range -30o to 105o but varies with age.
 The electrical current of a heartbeat normally flows from the SA node into the ventricles, roughly toward the positive pole of lead 2. The normal range -30o to 105o but varies with age.")
34
Limb lead axis.

35
Left axis deviation (LAD) any age group. -30o to -90o.
Right axis deviation (RAD) in adults. +90o to +180o. Extreme axis deviation (EAD) any age group. -90o to -180o.
 in adults. +90o to +180o. Extreme axis deviation (EAD) any age group. -90o to -180o.")
36
Step 6 P Waves. PR interval QRS Complex. Duration of PR interval
Note the width, height and shape of the P waves. PR interval Duration of PR interval Dose PR segment is isoelectric QRS Complex. Note the width, height, shape and pattern of the complex. Always assess Q waves relative to other clinical information If Q waves are not clearly diagnostic, then call them “nondiagnostic”.

37
ST Segments Study the ST segments separately from the T waves first, then together with the T waves. Look for deviation from the baseline, and shape of the ST segment. Shapes include flat, upsloping, downsloping, curved and straight. Note where the ST segment is relative to baseline 2 mm (80 msec) after the J point. Note carefully how the ST segment enters the T wave: is it smooth, or does it have an ominous abrupt entry?
 after the J point. Note carefully how the ST segment enters the T wave: is it smooth, or does it have an ominous abrupt entry")
38
Measuring ST Segments ST measurement = vertical difference between the isoelectric line + end of QRS complex, the “J” point”

39
ST segment elevation = >1 mm (>0
ST segment elevation = >1 mm (>0.1 mV) above baseline after the J point ST segment elevation due to severe injury temporary until ischemia resolved or injured heart tissue heals or dies ST segments elevate in leads facing the injury ST segments depress in leads opposite (reciprocal ) leads
 above baseline after the J point. ST segment elevation due to severe injury temporary until ischemia resolved or injured heart tissue heals or dies. ST segments elevate in leads facing the injury. ST segments depress in leads opposite (reciprocal ) leads.")
40
T Waves Note height and shape of the T waves. Shapes include smooth symmetry, asymmetry sharp peaking, inversion, and biphasic. Check again for the way the ST segment enters the T wave. QT Interval Calculate the QT interval to spot unusually short or long duration.

41
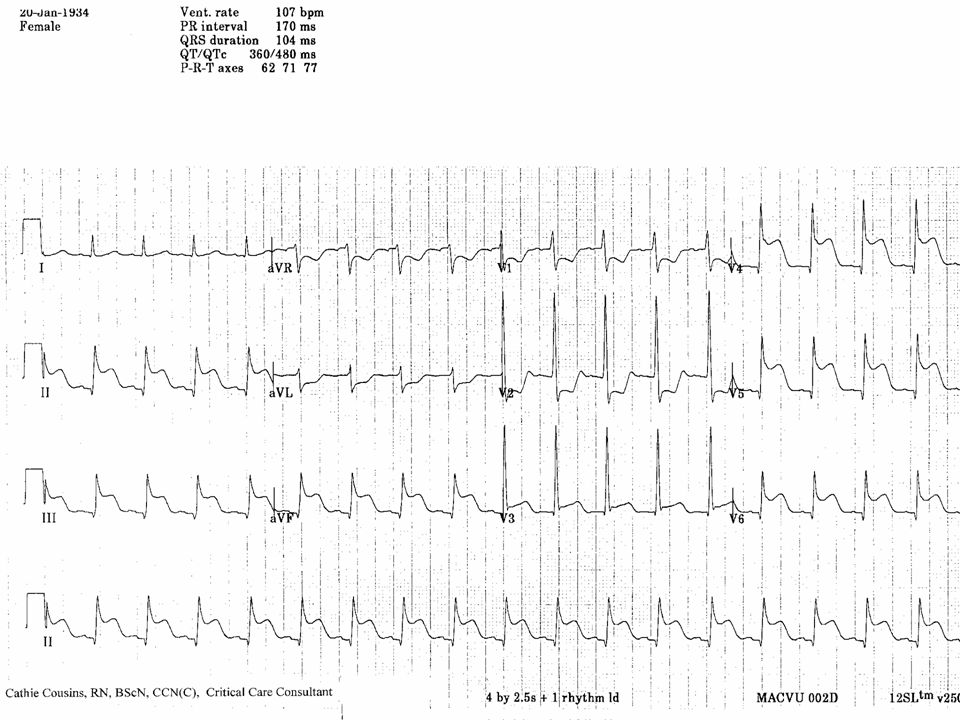
Sinus Tachycardia Causes Fever Pain Anxiety Hypoxia CHF
Fright or stress

42
Rate Rhythm regular P wave upright, normal P-R sec QRS sec P: QRS ratio 1: 1

43
Sinus Bradycardia Causes Normal in athletes Increased vagal tone
Sinus node disease Hypothermia Acute MI Drug effect (digoxin, CCB , BB)
")
44
Rate less than 60 bpm Rhythm regular P wave upright, normal P-R sec QRS sec P: QRS ratio 1: 1

45
Junctional Rhythm Causes Digitalis toxicity Acute MI Ischemia Hypoxia
Post valve surgery

46
Sinus node and atria fail to pace the heart.
AV junction paces at → 40-60/min No P wave or PR interval < 0.12, QRS normal

47
Idioventricular Rhythm
Causes SA node and AV node fail to initiate rhythm. MI Digoxin toxicity Metabolic imbalance Dying heart

48
Sinus node, atria, and AV junction fail to pace
Sinus node, atria, and AV junction fail to pace. Ectopic pacemaker in the ventricles paces at → 20-40/min No P wave, QRS wide, ST & T waves often abnormal

49
AV Blocks First degree AV block Causes
May be normal findings especially in athletes Myocardial ischemia injuring the AV node or junction Medication :quinidine, BB, CHB, digoxin, and amiodaron Acute MI Rheumatic heart disease Increased vagal tone

50
Usually normal rate , regular
PR interval is prolonged > 0.20 Normal QRS P: QRS Ratio 1:1

52
Second degree AV block Causes
Ischemic damage below the AV node, involving the bundle of his or the bundle branch Drugs , digoxin ,BB Increased vagal tone

53
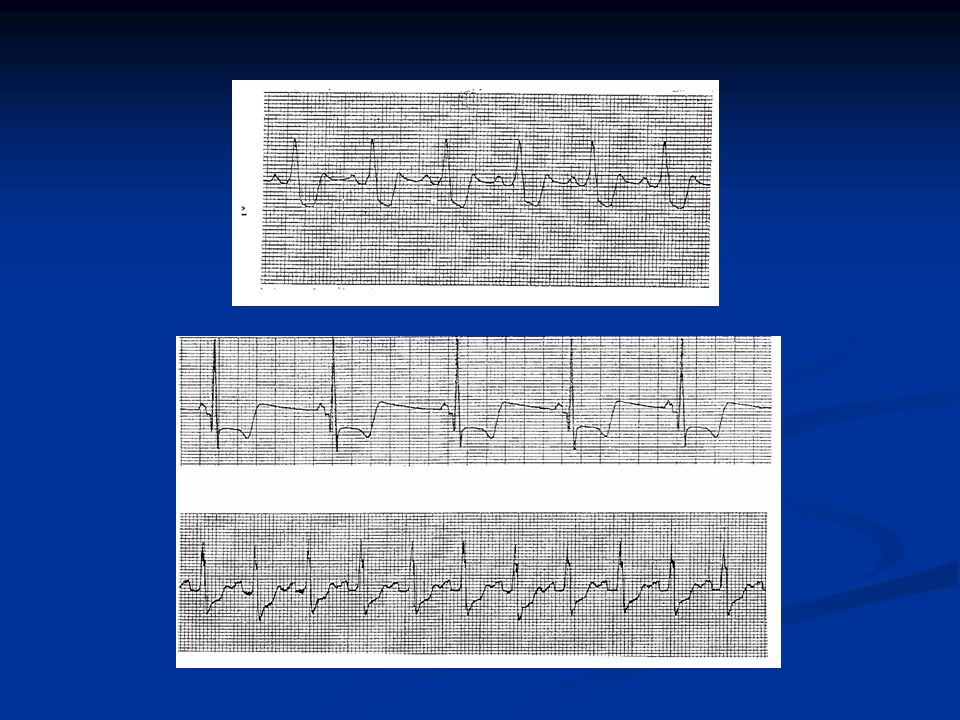
Mobitz type I (Wenckebach)
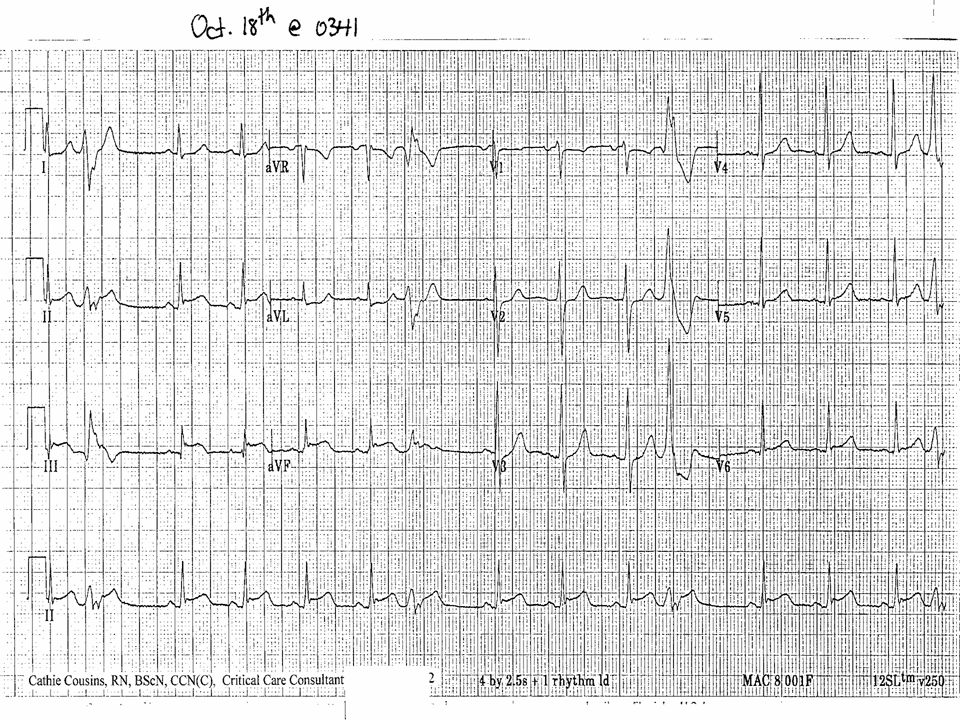
Progressive prolongation of PR interval until P wave fails to conduct to the ventricle Progressive shortening of RR interval until P wave is not conducted The RR interval containing the nonconducted P wave is shorter than the sum of two PP intervals

54
Acute inferior myocardial infarction with atrioventricular
block, second degree–Mobitz type I (Wenckebach),
,")
55
AV block, second degree–Mobitz type II
There are intermittent nonconducted P waves with no evidence of atrial prematurity In conducted beats, PR intervals stay constant The RR interval containing the nonconducted P wave is equal to two PP intervals

56
Sinus rhythm with atrioventricular block, second degree–Mobitz type II, and right bundle branch block.

57
Third degree AV block Causes Ischemic damage Post cardiac surgery Chronic degenerative changes of the conduction system Drugs, digoxin ,BB

58
Independent atrial and ventricular activities
Atrial rate faster than ventricular rate Ventricular rhythm maintained by a junctional or idioventricular escape rhythm or ventricular pacemaker When the ventricular rate is faster than the atrial rate, AV dissociation (not AV block)
")
60
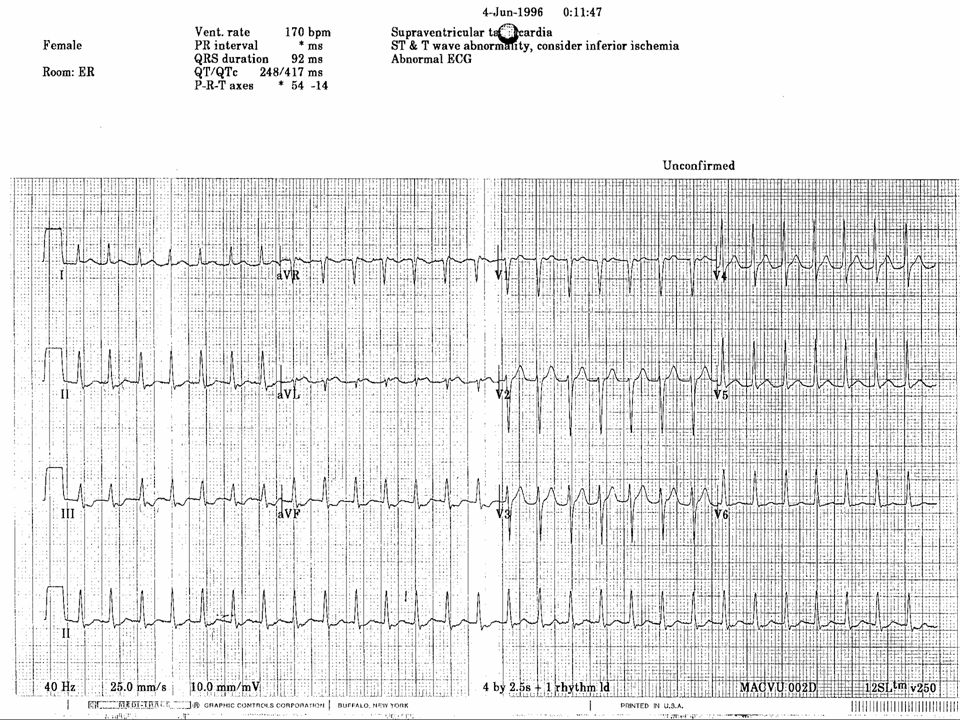
Superventricular Tachycardia
Ectopic focus in atria or AV junction paces the heart or Abnormal conduction thru AV node or Accessory pathway P wave or no P wave, QRS narrow or wide, rate > 150/min

62
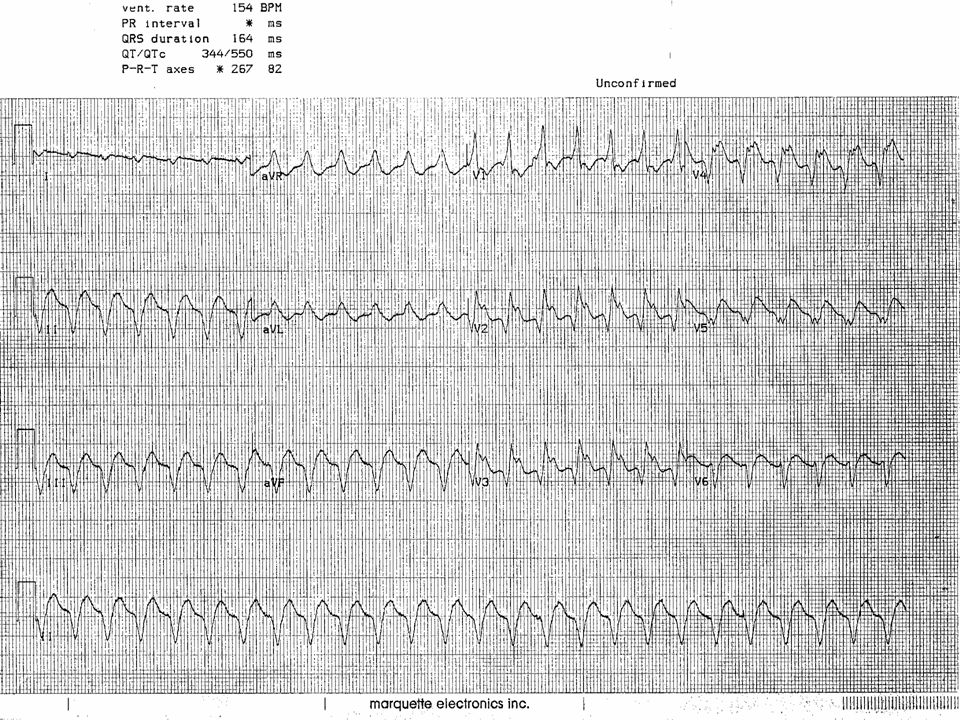
Ventricular Tachycardia
Ectopic pacemaker in ventricles paces the heart No P wave, QRS wide and bizarre

65
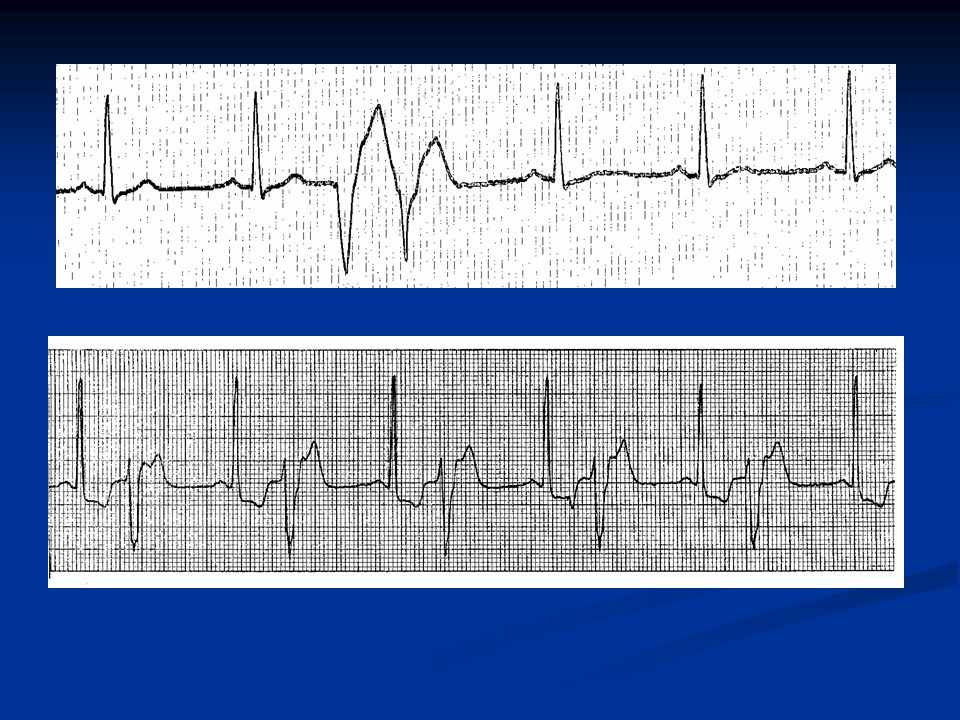
Premature Ventricular Contractions
QRS Duration QRS duration - depolarization of right and left ventricles, from the endocardium to epicardium Normal QRS duration sec QRS duration > sec, a conduction delay exists in the bundle branches, Purkinjie network or ventricular myocardium, or ventricular ectopic conduction exists

66
PVC’s, premature ventricular complexes:
the premature beat originates in an ectopic focus in one ventricle, it depolarizes that ventricle, then the other No P wave, QRS wide & bizarre, ST often abnormal, T wave often opposite the rhythm Multifocal PVC’s come from more than one ectopic focus, each foci has a different shape

67
1 PVC = a PVC 2 PVC’s = couplet 3 PVC’s = triplet 4 PVC’s = ventricular tachycardia Every 2nd PVC = bigeminy Every 3rd PVC = trigeminy Bigeminy or trigeminy can refer to any ectopic beat so clarify - eg. bigeminal PVC’s or bigeminal PAC’s, etc.

72
ST Segments

73
Other Common Causes of ST Segment Elevation
Coronary artery vasospasm Acute pericarditis Ventricular aneursym Hyperkalemia Non-specific ST-T wave changes

74
ST Segment Depression ST segment depression = > 1 mm below baseline after the J point ST segment depression due to severe ischemia temporary until ischemia resolved or heart tissue heals ST segments depress in leads facing the ischemia ST segments elevate in opposite (reciprocal) leads
 leads.")
76
Other Common Causes of ST Segment Depression
Left and right ventricular hypertrophy Left and right bundle branch block Digitalis in therapeutic and toxic doses

77
Acute MI Facing Leads Opposite Leads
Anterior Septal V1-V None Anterior V3-V None Lateral I, aVL, & V5 or V II, III, & aVF Inferior II, III, & aVF I & aVL Posterior V7,V8, V9 on 18 lead V1-V4 Right Ventricle V4R None

80
Thank you

Similar presentations













>")












>")