Download presentation
Presentation is loading. Please wait.

1
Ordinary to Extraordinary Improving Healthcare in Florida
Ferdinand Richards III, MD Chief Medical Director Peggy Loesch, BSN, MBA, RN Care Transitions Quality Specialist

2
Overview FMQAI – Information for Healthcare Improvement
Quality Improvement Organization (QIO) Program End Stage Renal Disease (ESRD) Network Program Key activities and opportunities to participate Improving Care Transitions through Collaboration, Commitment, and Action Care transitions and the reduction of avoidable readmissions Root causes of readmissions in Florida Coalition building across care settings to improve patient-centered care
 Program. End Stage Renal Disease (ESRD) Network Program. Key activities and opportunities to participate. Improving Care Transitions through Collaboration, Commitment, and Action. Care transitions and the reduction of avoidable readmissions. Root causes of readmissions in Florida. Coalition building across care settings to improve patient-centered care.")
3
FMQAI Information for Healthcare Improvement

4
Who is FMQAI? Established in 1992 as Florida Medical Quality Assurance, Inc. Improve quality care and outcomes through data, education, and technical assistance Collaborate with physicians, health plans, home health agencies, nursing homes, dialysis facilities, rehabilitation facilities, and hospitals Nationally recognized healthcare contractor Florida Quality Improvement Organization (QIO) End Stage Renal Disease (ESRD) Networks – Arkansas, Florida, Louisiana, Oklahoma, and Southern California Department of Health Private medical record review and chart abstraction FMQAI is Florida's leader in healthcare quality improvement, having implemented more than 80 projects with hospitals, home health agencies, nursing homes, managed care organizations, chronic dialysis facilities, kidney transplant centers and physicians. We offer consultation services on quality indicator development, performance measurement, rapid cycle improvement, planning, implementation, and evaluation of collaborative intervention models, cultural competence and other strategies to improve healthcare. Assist providers with the implementation of best practices Federal, state, and private contracts
 End Stage Renal Disease (ESRD) Networks – Arkansas, Florida, Louisiana, Oklahoma, and Southern California. Department of Health. Private medical record review and chart abstraction. FMQAI is Florida s leader in healthcare quality improvement, having implemented more than 80 projects with hospitals, home health agencies, nursing homes, managed care organizations, chronic dialysis facilities, kidney transplant centers and physicians. We offer consultation services on quality indicator development, performance measurement, rapid cycle improvement, planning, implementation, and evaluation of collaborative intervention models, cultural competence and other strategies to improve healthcare. Assist providers with the implementation of best practices. Federal, state, and private contracts.")
5
The QIO Program Legislated under sections of the Social Security Act 53 QIOs tasked with review of medical care, investigation of beneficiary complaints, and implementation of quality improvement activities for Medicare Evolution of the QIO program 1970s – Professional Standards Review Organization (PSRO) – performed utilization reviews and special studies to improve quality of care 1982 – Utilization and Quality Control Peer Review Organization (PRO) – data analysis to determine unnecessary, inappropriate, or poor quality 1992 – Health Care Quality Improvement Initiative (HCQII) – focus shifted from case review to reporting patterns of care 2001 – QIO Program – renamed to be consistent with collaboration The Medicare Program was signed into law on July 30, 1965 by President Lyndon B. Johnson. At the bill-signing ceremony, President Johnson enrolled former President Harry S. Truman as the first Medicare beneficiary and presented him with the first Medicare card. QIO program dates back to the 1970s with the creation of the Professional Standards Review Organization (PSRO) program. PSROs performed utilization reviews and special studies to improve the quality of care, primarily for Medicare and Medicaid. In 1982, as part of the Tax Equity and Fiscal Responsibility Act, Congress replaced the PSRO program with the Utilization and Quality Control PRO. Assembled and analyzed data on services provided to Medicare beneficiaries Intervened when services had been provided unnecessarily, inappropriately, or with inadequate quality Required to randomly sample a percentage of hospital records for case review, including inadequate discharge planning, medical instability of the patient at discharge, and deaths In 1992, role of PROs changed with implementation of Health Care Quality Improvement Initiative (HCQII). HCQII shifted focus from individual case reviews to reporting patterns of care delivered to beneficiaries. PROs were to: Examine practice patterns at the institutional, regional, and national level, rather than uncover individual physician lapses in quality for punitive purposes. Evaluate quality of care using national, disease-specific guidelines, rather than local criteria. Work collaboratively with hospitals as partners in the development and implementation of hospital quality improvement initiatives (instead of merely collecting data). Consistent with the new collaborative style and broadening scope of the PRO program, it was officially renamed the QIO Program in 2001. The roots of the QIO program date back to the 1970s with the creation of the Professional Standards Review Organization (PSRO) program. PSROs were charged with performing utilization reviews and studies to improve the quality of care for federally subsidized insurance programs, primarily Medicare and Medicaid (Jost 1989). In 1982, as part of the Tax Equity and Fiscal Responsibility Act, Congress replaced the PSRO program with the Utilization and Quality Control PRO Program (Jost 1989; Institute of Medicine 1990), now known as the QIO Program. The PROs initially took an “inspect and detect” approach to assessing the quality of services. PROs were to: (1) assemble and analyze data on services provided to Medicare beneficiaries and (2) intervene when services had been provided unnecessarily, inappropriately, or with inadequate quality (Jost 1989). Under their contracts with the Health Care Financing Administration (HCFA, now CMS), the PROs were required to randomly sample a percentage of hospital records for case review. This case review focused on seven indicators of deficient care (General Accounting Office 1988; Jost 1989; Institute of Medicine 1990): inadequate discharge planning, medical instability of the patient at discharge, deaths, nosocomial infection, unscheduled return to surgery, trauma suffered in the hospital, and medication or treatment changes within 24 hours of discharge without adequate observation (Institute of Medicine 1990). If a hospital had too many deficiencies within sampled records, the PROs could do an intensified (100%) review of records to estimate the magnitude of the deficiency (Jost 1989). Physicians with persistent quality problems faced harsh penalties, including payment denial and recommended exclusion from participation in the Medicare program (Jost 1989). The “inspect and detect” approach was problematic for several reasons. Many physicians and hospitals perceived the review process to be flawed, a view supported by studies showing poor reliability of peer assessments of quality of care (Berry 1992; Goldman 1992) and inconsistent PRO processes across states (Institute of Medicine 1990; Kellie and Kelly 1991). In addition, HCFA was unable to document any improvement in the quality of care delivered to Medicare beneficiaries as a result of the PRO “inspect and detect” efforts (General Accounting Office 1988; Audet and Scott 1993; Ellerback et al. 1995; Weinmann 1998). The PRO processes of retrospective auditing and potential penalties led to an acrimonious relationship between PROs and hospitals and their physicians (Jencks and Wilensky 1992; Nash 1992; Audet and Scott 1993; Weinmann 1998). Rather than fostering an environment for proactive improvement of the quality of care for patients, the inspection approach pitted regulators against hospitals and physicians, and did little to advance quality improvement initiatives (Weinmann 1998). In 1992, HCFA dramatically changed the role of PROs with the implementation of the Health Care Quality Improvement Initiative (HCQII) (Jencks and Wilensky 1992). The HCQII changed the PRO program's approach to data collection, its quality of care evaluation criteria, and its role in implementing quality initiatives. First, the approach to data collection shifted from individual case reviews to reporting patterns of care delivered to beneficiaries (Audet and Scott 1993). PROs were to examine practice patterns at the institutional, regional, and national level, rather than uncover individual physician lapses in quality for punitive purposes (Audet and Scott 1993). Second, PROs were to evaluate quality of care using national, disease-specific guidelines, rather than local criteria (Jencks and Wilensky 1992). Third, instead of merely collecting and reporting data, PROs were to work collaboratively with hospitals as partners in the development and implementation of hospital quality improvement initiatives (Jencks and Wilensky 1992). These changes, designed to transform the PRO from adversary to partner, represented a dramatic shift in vision and potential impact of the PRO system on hospital quality. The first initiative for the HCQII was the implementation of the Cooperative Cardiovascular Project, which began in 1992 as a four-state pilot project to develop quality indictors for the care of AMI patients and support hospitals in their development of quality improvement initiatives (Sprague 2002). Quality indicators were applied using retrospective review of the medical records of Medicare patients discharged with a principle diagnosis of AMI over a 9-month period in four pilot states (Ellerbeck et al. 1995). PROs also intervened in these four states by facilitating and encouraging the adoption of quality improvement initiatives in AMI care. A follow-up study found significant improvement in the quality indicators and survival rates after AMI in the pilot states, as compared with the nonpilot states, suggesting significant success of the interventions aided by the PROs (Marciniak et al. 1998). During the next two contract cycles (1996–1999 and 1999–2002), PROs implemented AMI quality initiatives in hospitals nationwide, and, by 1999, had broadened their scope to include national quality of care projects in breast cancer, diabetes, heart failure, pneumonia, and stroke (Sprague 2002). During the period 1998/99 to 2000/01, more than half of the states improved on 20 of the 22 quality of care indicators for these medical conditions (Jencks, Huff, and Cuerdon 2003). Consistent with the new collaborative style and broadening scope of the PRO program, it was officially renamed the QIO Program in 2001 (CMS Federal Register 2002). While this name change was largely symbolic, it was indicative of the expanding role of QIOs in quality improvement initiatives. QIOs are currently operating within the seventh contract cycle with CMS and have been charged with quality improvement initiatives in numerous clinical areas and across a variety of health care settings. However, despite the expansion in the QIOs' responsibilities, there has been no published assessment of whether or not hospitals believe QIO interventions are improving the quality of care. This information would be helpful to define the extent of the QIOs' current success in assisting hospitals to improve care and to direct future efforts of the QIOs. If a hospital had too many deficiencies within sampled records, the PROs could do an intensified review (100%). Physicians with persistent quality problems faced harsh penalties, including payment denial and recommended exclusion from participation in the Medicare program.
 – performed utilization reviews and special studies to improve quality of care – Utilization and Quality Control Peer Review Organization (PRO) – data analysis to determine unnecessary, inappropriate, or poor quality – Health Care Quality Improvement Initiative (HCQII) – focus shifted from case review to reporting patterns of care – QIO Program – renamed to be consistent with collaboration. The Medicare Program was signed into law on July 30, 1965 by President Lyndon B. Johnson. At the bill-signing ceremony, President Johnson enrolled former President Harry S. Truman as the first Medicare beneficiary and presented him with the first Medicare card. QIO program dates back to the 1970s with the creation of the Professional Standards Review Organization (PSRO) program. PSROs performed utilization reviews and special studies to improve the quality of care, primarily for Medicare and Medicaid. In 1982, as part of the Tax Equity and Fiscal Responsibility Act, Congress replaced the PSRO program with the Utilization and Quality Control PRO. Assembled and analyzed data on services provided to Medicare beneficiaries. Intervened when services had been provided unnecessarily, inappropriately, or with inadequate quality. Required to randomly sample a percentage of hospital records for case review, including inadequate discharge planning, medical instability of the patient at discharge, and deaths. In 1992, role of PROs changed with implementation of Health Care Quality Improvement Initiative (HCQII). HCQII shifted focus from individual case reviews to reporting patterns of care delivered to beneficiaries. PROs were to: Examine practice patterns at the institutional, regional, and national level, rather than uncover individual physician lapses in quality for punitive purposes. Evaluate quality of care using national, disease-specific guidelines, rather than local criteria. Work collaboratively with hospitals as partners in the development and implementation of hospital quality improvement initiatives (instead of merely collecting data). Consistent with the new collaborative style and broadening scope of the PRO program, it was officially renamed the QIO Program in The roots of the QIO program date back to the 1970s with the creation of the Professional Standards Review Organization (PSRO) program. PSROs were charged with performing utilization reviews and studies to improve the quality of care for federally subsidized insurance programs, primarily Medicare and Medicaid (Jost 1989). In 1982, as part of the Tax Equity and Fiscal Responsibility Act, Congress replaced the PSRO program with the Utilization and Quality Control PRO Program (Jost 1989; Institute of Medicine 1990), now known as the QIO Program. The PROs initially took an inspect and detect approach to assessing the quality of services. PROs were to: (1) assemble and analyze data on services provided to Medicare beneficiaries and (2) intervene when services had been provided unnecessarily, inappropriately, or with inadequate quality (Jost 1989). Under their contracts with the Health Care Financing Administration (HCFA, now CMS), the PROs were required to randomly sample a percentage of hospital records for case review. This case review focused on seven indicators of deficient care (General Accounting Office 1988; Jost 1989; Institute of Medicine 1990): inadequate discharge planning, medical instability of the patient at discharge, deaths, nosocomial infection, unscheduled return to surgery, trauma suffered in the hospital, and medication or treatment changes within 24 hours of discharge without adequate observation (Institute of Medicine 1990). If a hospital had too many deficiencies within sampled records, the PROs could do an intensified (100%) review of records to estimate the magnitude of the deficiency (Jost 1989). Physicians with persistent quality problems faced harsh penalties, including payment denial and recommended exclusion from participation in the Medicare program (Jost 1989). The inspect and detect approach was problematic for several reasons. Many physicians and hospitals perceived the review process to be flawed, a view supported by studies showing poor reliability of peer assessments of quality of care (Berry 1992; Goldman 1992) and inconsistent PRO processes across states (Institute of Medicine 1990; Kellie and Kelly 1991). In addition, HCFA was unable to document any improvement in the quality of care delivered to Medicare beneficiaries as a result of the PRO inspect and detect efforts (General Accounting Office 1988; Audet and Scott 1993; Ellerback et al. 1995; Weinmann 1998). The PRO processes of retrospective auditing and potential penalties led to an acrimonious relationship between PROs and hospitals and their physicians (Jencks and Wilensky 1992; Nash 1992; Audet and Scott 1993; Weinmann 1998). Rather than fostering an environment for proactive improvement of the quality of care for patients, the inspection approach pitted regulators against hospitals and physicians, and did little to advance quality improvement initiatives (Weinmann 1998). In 1992, HCFA dramatically changed the role of PROs with the implementation of the Health Care Quality Improvement Initiative (HCQII) (Jencks and Wilensky 1992). The HCQII changed the PRO program s approach to data collection, its quality of care evaluation criteria, and its role in implementing quality initiatives. First, the approach to data collection shifted from individual case reviews to reporting patterns of care delivered to beneficiaries (Audet and Scott 1993). PROs were to examine practice patterns at the institutional, regional, and national level, rather than uncover individual physician lapses in quality for punitive purposes (Audet and Scott 1993). Second, PROs were to evaluate quality of care using national, disease-specific guidelines, rather than local criteria (Jencks and Wilensky 1992). Third, instead of merely collecting and reporting data, PROs were to work collaboratively with hospitals as partners in the development and implementation of hospital quality improvement initiatives (Jencks and Wilensky 1992). These changes, designed to transform the PRO from adversary to partner, represented a dramatic shift in vision and potential impact of the PRO system on hospital quality. The first initiative for the HCQII was the implementation of the Cooperative Cardiovascular Project, which began in 1992 as a four-state pilot project to develop quality indictors for the care of AMI patients and support hospitals in their development of quality improvement initiatives (Sprague 2002). Quality indicators were applied using retrospective review of the medical records of Medicare patients discharged with a principle diagnosis of AMI over a 9-month period in four pilot states (Ellerbeck et al. 1995). PROs also intervened in these four states by facilitating and encouraging the adoption of quality improvement initiatives in AMI care. A follow-up study found significant improvement in the quality indicators and survival rates after AMI in the pilot states, as compared with the nonpilot states, suggesting significant success of the interventions aided by the PROs (Marciniak et al. 1998). During the next two contract cycles (1996–1999 and 1999–2002), PROs implemented AMI quality initiatives in hospitals nationwide, and, by 1999, had broadened their scope to include national quality of care projects in breast cancer, diabetes, heart failure, pneumonia, and stroke (Sprague 2002). During the period 1998/99 to 2000/01, more than half of the states improved on 20 of the 22 quality of care indicators for these medical conditions (Jencks, Huff, and Cuerdon 2003). Consistent with the new collaborative style and broadening scope of the PRO program, it was officially renamed the QIO Program in 2001 (CMS Federal Register 2002). While this name change was largely symbolic, it was indicative of the expanding role of QIOs in quality improvement initiatives. QIOs are currently operating within the seventh contract cycle with CMS and have been charged with quality improvement initiatives in numerous clinical areas and across a variety of health care settings. However, despite the expansion in the QIOs responsibilities, there has been no published assessment of whether or not hospitals believe QIO interventions are improving the quality of care. This information would be helpful to define the extent of the QIOs current success in assisting hospitals to improve care and to direct future efforts of the QIOs. If a hospital had too many deficiencies within sampled records, the PROs could do an intensified review (100%). Physicians with persistent quality problems faced harsh penalties, including payment denial and recommended exclusion from participation in the Medicare program.")
6
QIO 10th Statement of Work
Bold goals – supports the aims of the DHHS National Quality Strategy Patient-centered care – includes the voice of the beneficiary in all their activities Boundarilessness – breaks down organizational, cultural, and geographic barriers Learning and Action Network (LAN) – accelerates change and spread of best practices where everyone teaches and learns Value-based purchasing – provides technical assistance, including sharing best practices and QI activities
 – accelerates change and spread of best practices where everyone teaches and learns. Value-based purchasing – provides technical assistance, including sharing best practices and QI activities.")
7
Medical Case Review Beneficiary complaints Immediate advocacy Appeals
Higher Weighted Diagnosis-Related Groups (HWDRGs) Emergency Medical Treatment and Active Labor Act (EMTALA)
 Emergency Medical Treatment and Active Labor Act (EMTALA)")
8
Patient Safety Hospitals Nursing homes
Central line-associated bloodstream infections (CLABSI) Catheter-associated urinary tract infections (CAUTI) Clostridium difficile (C. diff) Surgical site infections (SSI) Nursing homes Pressure ulcers Physical restraints Use of antipsychotic medications Clinical pharmacists, physicians, and facilities Adverse drug events (ADE) Potential ADEs
 Catheter-associated urinary tract infections (CAUTI) Clostridium difficile (C. diff) Surgical site infections (SSI) Nursing homes. Pressure ulcers. Physical restraints. Use of antipsychotic medications. Clinical pharmacists, physicians, and facilities. Adverse drug events (ADE) Potential ADEs.")
9
Prevention Assist physician practices with use of electronic health record (EHR) system Coordinate prevention services Report quality measures Reduce patient risk factors for cardiac disease Partner with local Health Information Technology Regional Extension Centers (REC) The QIO Program is the largest federal program dedicated to improving health quality at the community level. QIOs in every state and territory, united in a network administered by CMS, have the flexibility to respond to local needs. From August 2011 through July 2014, health care providers and other quality stakeholders who participate in QIO initiatives can: • Improve Individual Patient Care. QIO patient safety initiatives in hospitals will reduce central line bloodstream infections by implementing the Comprehensive Unit-Based Safety Program (CUSP), then expand to encompass catheter-associated urinary tract infections, Clostridium difficile and surgical site infections. All Medicare-participating hospitals also will receive QIO technical assistance for reporting inpatient and outpatient quality data to CMS. In nursing homes, work initially targets pressure ulcers and physical restraints, then evolves to address other health care-acquired conditions, such as falls and catheter-associated urinary tract infections. To decrease adverse drug events, QIOs are bringing clinical pharmacists, physicians and facilities together in local Patient Safety Clinical Pharmacy Services Collaboratives (PSPC), following the successful HRSA model. • Improve Health for Populations and Communities. QIOs are assisting physician practices that want to use their electronic health record system to coordinate preventive services and report related quality measures to CMS. Practices also can participate in a learning network focused on reducing patient risk factors for cardiac disease. QIOs will partner with their local Health Information Technology Regional Extension Center (REC) to promote health IT integration into clinical practice. • Integrate Care for Populations and Communities. QIOs are bringing together hospitals, nursing homes, patient advocacy organizations and other stakeholders in community coalitions. Goals are to build capacity for improving care transitions and to support the coalition’s success in obtaining grant funding through Section 3026 of the Affordable Care Act. • Deliver Beneficiary and Family Centered Care. QIO Program improvement initiatives result in safer, more effective patient care, lead to better health for populations and communities, and drive lower health care costs through improvement. QIOs also fulfill CMS’ obligation to protect the rights of Medicare beneficiaries by reviewing complaints about quality and appeals about the denial or discontinuation of health care services.
 The QIO Program is the largest federal program dedicated to improving health quality at the community level. QIOs in every state and territory, united in a network administered by CMS, have the flexibility to respond to local needs. From August 2011 through July 2014, health care providers and other quality stakeholders who participate in QIO initiatives can: • Improve Individual Patient Care. QIO patient safety initiatives in hospitals will reduce central line bloodstream infections by implementing the Comprehensive Unit-Based Safety Program (CUSP), then expand to encompass catheter-associated urinary tract infections, Clostridium difficile and surgical site infections. All Medicare-participating hospitals also will receive QIO technical assistance for reporting inpatient and outpatient quality data to CMS. In nursing homes, work initially targets pressure ulcers and physical restraints, then evolves to address other health care-acquired conditions, such as falls and catheter-associated urinary tract infections. To decrease adverse drug events, QIOs are bringing clinical pharmacists, physicians and facilities together in local Patient Safety Clinical Pharmacy Services Collaboratives (PSPC), following the successful HRSA model. • Improve Health for Populations and Communities. QIOs are assisting physician practices that want to use their electronic health record system to coordinate preventive services and report related quality measures to CMS. Practices also can participate in a learning network focused on reducing patient risk factors for cardiac disease. QIOs will partner with their local Health Information Technology Regional Extension Center (REC) to promote health IT integration into clinical practice. • Integrate Care for Populations and Communities. QIOs are bringing together hospitals, nursing homes, patient advocacy organizations and other stakeholders in community coalitions. Goals are to build capacity for improving care transitions and to support the coalition’s success in obtaining grant funding through Section 3026 of the Affordable Care Act. • Deliver Beneficiary and Family Centered Care. QIO Program improvement initiatives result in safer, more effective patient care, lead to better health for populations and communities, and drive lower health care costs through improvement. QIOs also fulfill CMS’ obligation to protect the rights of Medicare beneficiaries by reviewing complaints about quality and appeals about the denial or discontinuation of health care services.")
10
Additional QIO Efforts
Maintenance & Development of Medication Measures Hospital Outpatient / Ambulatory Surgical Center Quality Reporting Program Support Contractor Beneficiary-centered Model for Weight Loss in African American Communities – Senior Lifestyle Improvement Movement (SLIM) Patient and Family Engagement Campaign – Promoting e-Health Technology, Awareness & Knowledge (PEAK) Heart Health Beneficiary and Family-centered Care National Coordinating Center
 Patient and Family Engagement Campaign – Promoting e-Health Technology, Awareness & Knowledge (PEAK) Heart Health. Beneficiary and Family-centered Care National Coordinating Center.")
11
The ESRD Network Program
The Social Security Amendments of 1972 created the national ESRD Program, which extended Medicare coverage to individuals with ESRD The Social Security Act was again amended in 1978 to create the ESRD Network Program Originally 32 regional ESRD Networks, now only 18 Networks Responsible for effective and efficient administration of ESRD benefits Improve quality of care, collect data, provide technical assistance, and review patient grievances October , the Medicare ESRD Program was signed into law by President Nixon. TEXT: Dialysis -- Number of facilities = 763 and Number of patients = 24,391 TEXT: Transplant -- Number of facilities = 151 and Number of patients transplanted = 3,044 (Insert a scan of the report)
")
12
Current ESRD Statement of Work
Strategic Aims Drivers of Change Patient experience of care Access to dialysis Vascular access management Patient safety – healthcare acquired infections (HAIs) Immunization rates ESRD quality incentive program Facility data submission Breakthrough collaboratives Patient engagement Campaigns Technical assistance On-site visits Learning and Action Networks (LANs)
 Immunization rates. ESRD quality incentive program. Facility data submission. Breakthrough collaboratives. Patient engagement. Campaigns. Technical assistance. On-site visits. Learning and Action Networks (LANs)")
13
Key Activities & Opportunities
HealthHub – community portal to promote sharing and collaboration of information resources, tools, and knowledge Learning and Action Networks – initiative that brings together healthcare professionals, patients, and other stakeholders No Place Like Home – stakeholders across care continuum to improve transitions of care and prevent hospital readmissions QIO Strategic Council (QSC) – leadership group to assist with coordinating efforts, minimizing duplication, maintaining momentum, enhancing commitment, and spreading the best practices
 – leadership group to assist with coordinating efforts, minimizing duplication, maintaining momentum, enhancing commitment, and spreading the best practices.")
14
www.healthhubfl.com Password protected
Secure repository for documents, tools, and resources Forums Polls Calendar of events

15
Learning and Action Network
April 11, 2014 Tampa, Florida Connect with organizations and individuals from across all provider types that have similar QI goals and challenges Learn from others in an "all teach, all learn" environment Benefit from others' best practices Receive and share free information and tools Be recognized for meeting or exceeding improvement targets

16
Improving Care Transitions through Collaboration, Commitment, and Action

17
Objectives Know the significance of improving the quality of care transitions to reduce avoidable readmissions Understand the root causes of readmissions in Florida Recognize the importance of coalition building across care settings to improve patient-centered care

18
National Strategy for Quality Improvement in Healthcare
Established by the Affordable Care Act Develops an infrastructure at the community level that assumes responsibility for improvement efforts Promotes patient-centered outcomes, efficiency, and appropriate care while reducing or eliminating waste from the healthcare system The 2012 National Quality Strategy progress report identified three strategic opportunities for accelerating system-wide improvement across all of the aims and priorities; this report provides information on progress made against each. The three opportunities are: Develop a national strategy for data collection, measurement, and reporting that supports performance measurement and improvement efforts of public- and private-sector stakeholders at the national and community level. Develop an infrastructure at the community level that assumes responsibility for improvement efforts; resources for communities to benchmark and compare performance; and mechanisms to identify, share, and evaluate progress. Develop payment and delivery system reforms—emphasizing primary care—that reward value over volume; promote patient-centered outcomes, efficiency, and appropriate care; and seek to improve quality while reducing or eliminating waste from the system. Making care safer by reducing harm caused in the delivery of care. Ensuring that each person and family is engaged as partners in their care. Promoting effective communication and coordination of care. Promoting the most effective prevention and treatment practices for the leading causes of mortality, starting with cardiovascular disease. Working with communities to promote wide use of best practices to enable healthy living. Making quality care more affordable for individuals, families, employers, and governments by developing and spreading new health care delivery models. Source:

19
“Three-Part Aim” National Quality Strategy
Better Health for the Population Lower Cost Through Improvement Better Care for Individuals

20
National Strategy for Quality Improvement in Healthcare
Safer Care Reduce Readmissions Reduce inappropriate or unnecessary care Engage Enable patients and families to be able to navigate, coordinate care Improve the experience of care related to quality, safety, and access across settings Coordinate Improve care transitions and communications Establish shared accountability and integration of communities and providers Source:

21
Timeline for National Quality Initiatives
/2016 Hospital Medicare readmission penalties NH Value-based purchasing demo (ended June 2012) Hospital value-based purchasing program penalties Community-based care transitions program Expansion of pilot programs to evaluate bundling payment for an episode of care Reduce avoidable hospitalizations among nursing facility residents (ends August 2016) QAPI demonstration project (ended August 2013) Source: The Henry J. Kaiser Foundation. Health Reform Implementation Timeline :
 Hospital value-based purchasing. program penalties. Community-based care transitions program. Expansion of pilot programs to evaluate bundling payment for an episode of care. Reduce avoidable hospitalizations among nursing facility residents (ends August 2016) QAPI demonstration project (ended August 2013) Source: The Henry J. Kaiser Foundation. Health Reform Implementation Timeline :")
22
Definition of Readmissions
“… in the case of an individual who is discharged from an applicable hospital, the admission of the individual to the same or another applicable hospital with in 30 days from the date of discharge.” Source:

23
Readmissions Impact Multiple Areas
Quality Patient Safety Cost

24
Magnitude of the Problem
Analysis of 2007 Medicare data finds: 20% of beneficiaries are re-hospitalized within 30 days 35% are re-hospitalized within 90 days Among those re-hospitalized within 30 days: 50% had no claim for physician services between discharge and re-hospitalization Source: Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. The New England Journal of Medicine. 2009;360:

25
Magnitude of the Problem (continued)
Beneficiaries with 10 or more chronic conditions are 6 times more likely to be readmitted to the hospital. Analysis of 2008 Medicare data finds: Beneficiaries with 10 or more chronic conditions are 6 times more likely than those with 1-4 chronic conditions to be readmitted to the hospital Beneficiaries with 10 or more chronic conditions are: 8.9% of all Medicare beneficiaries, but are responsible for 31% of all hospitalizations, and 50.2% of all readmissions Source: Berkowitz SA, Anderson GF. Medicare beneficiaries most likely to be readmitted. J. Hosp. Med. Nov 2013;8(11):
:")
26
Magnitude of the Problem (continued)
A managed care organization with 18 hospitals: 250 out of 537 (or 47%) readmissions were considered potentially avoidable. Factors contributing to avoidable readmissions: Index stay Suboptimal management of the condition present The discharge process, care transitions, and care coordination Unaddressed psychological and social needs Follow-up care Failure to adjust the plan of care to better meet patient needs Source: Feigenbaum P, Neuwirth E, Trowbridge L, et al. Factors contributing to all-cause 30-day readmissions: a structured case series across 18 hospitals. Med. Care. Jul 2012;50(7):
 readmissions were considered potentially avoidable. Factors contributing to avoidable readmissions: Index stay. Suboptimal management of the condition present. The discharge process, care transitions, and care coordination. Unaddressed psychological and social needs. Follow-up care. Failure to adjust the plan of care to better meet patient needs. Source: Feigenbaum P, Neuwirth E, Trowbridge L, et al. Factors contributing to all-cause 30-day readmissions: a structured case series across 18 hospitals. Med. Care. Jul 2012;50(7):")
27
30-Day Readmission Rates
Nation 18.60% Florida 19.36% Data: Medicare Fee-For-Service (FFS) Admissions from January 1, 2012 to December 31, 2012. Nationally: 10,663,197 beneficiary admissions 1,912,227 beneficiary readmissions 30-day Readmission Rate: 18.60% Florida: 763,995 beneficiary admissions 143,995 beneficiary readmissions 30-day Readmission Rate: 19.36% Source: ICPC Quarterly Scorecard for Florida, 1/1/ /31/2012 issued 6/1/2013 from Colorado Foundation for Medical Care
 Admissions from January 1, 2012 to December 31, Nationally: 10,663,197 beneficiary admissions. 1,912,227 beneficiary readmissions. 30-day Readmission Rate: 18.60% Florida: 763,995 beneficiary admissions. 143,995 beneficiary readmissions. 30-day Readmission Rate: 19.36% Source: ICPC Quarterly Scorecard for Florida, 1/1/ /31/2012 issued 6/1/2013 from Colorado Foundation for Medical Care.")
28
No post-acute follow up
Risk of Readmissions Hospital Discharge No post-acute follow up Readmission In Florida, 53.76% of readmitted beneficiaries returned to the hospital without receiving any formal care after the index hospital discharge.

29
Issues Related to Care Transitions: Findings From Florida Communities
This demonstrates the innumerable complexities of the issues with improving care transitions and reducing readmissions. It spans all providers including patients and caregivers. We need everyone’s participation to improve cross-setting processes.

30
Examples of Causes of Readmissions in Florida
Lack of Effective Communication Medication Related Issues Lack of Resources Discharge Processes Examples: Patients: Need nutritional support. Do not understand their treatment plan and/or illness. Lack support at home Do not have primary care physicians. Physicians/Health Care Providers: Primary care physician is unaware of patient hospitalization. Lack of communication. Lack of care coordination. Patients do not follow up with the physician. Resources: Patients do not have transportation. Medications: Poly-pharmacy. Patients do not understand their medications. Discharge: Discharges are rushed, unstructured, and/or chaotic. Poorly defined transition process.

31
At $9,600 per readmission in 2011 readmission cost
Industry Impact $ At $9,600 per readmission in 2011 readmission cost Nation: $18,931,200,000 Florida: $47,833,440 National: 1,972,000 beneficiary readmissions at $9,600 per readmission Cost estimate: $18,931,200,000 Florida 99,653 beneficiary readmissions at $9,600 per readmission Cost estimate: $47,833,440 Source: Medicare FFS Inpatient Claims, 2011.

32
Patient Impact Re-hospitalization places patient and family under significant physical and emotional distress. The patient is at risk for potential medical errors, falls, and infections. Exposed to Post-Hospital Syndrome: “During hospitalization, patients are commonly deprived of sleep, experience disruption of normal circadian rhythms, are nourished poorly, have pain and discomfort, confront a baffling array of mentally challenging situations, receive medications that can alter cognition and physical function, and become deconditioned by bed rest or inactivity…” Source: Krumholz HM. Post-hospital syndrome--an acquired, transient condition of generalized risk. N. Engl. J. Med. Jan ;368(2):
:")
33
State and National Quality Initiatives
Use logos and website addresses: Nursing Home Quality Care Campaign CMS Innovation programs Community-based Care Transitions Program No Place Like Home Campaign Home Health Quality Improvement Hospital Engagement Networks – Partnership for Patients Logo

34
FMQAI – The Florida QIO Collaboration Commitment
The Centers for Medicare & Medicaid Services (CMS) leads the largest federal program dedicated to improving health quality at the local level. FMQAI is the Medicare Quality Improvement Organization (QIO) for the state of Florida. We bring communities together for learning and action to achieve national health quality goals supporting improvements in population health, while decreasing healthcare costs for all Americans. The QIO program is a catalyst for widespread significant improvement of healthcare quality through collaboration with local organizations, patients and families, healthcare providers, and other stakeholders for mutual learning and improvement. Collaboration Commitment
 leads the largest federal program dedicated to improving health quality at the local level. FMQAI is the Medicare Quality Improvement Organization (QIO) for the state of Florida. We bring communities together for learning and action to achieve national health quality goals supporting improvements in population health, while decreasing healthcare costs for all Americans. The QIO program is a catalyst for widespread significant improvement of healthcare quality through collaboration with local organizations, patients and families, healthcare providers, and other stakeholders for mutual learning and improvement. Collaboration. Commitment.")
35
Role of FMQAI in Care Transitions
Facilitate in coalition building Assist with conducting root cause analyses Provide education and support for the selection of evidence-based interventions, implementation, and measurement Partner with local, regional, & statewide groups Provide technical assistance including readmission data for the coalitions

36
The Role of the Community Organization
Spearheads coalition building among providers, stakeholders, and service organizations Seen as trusted community presence Understands and transcends the politics of the community Motivates and engages in ongoing communications among community stakeholders Promotes a shared vision for patient-centered change

37
The Role of the Community Organization (continued)
Provides expertise in the local community regarding needs and resources to maintain the health, independence, and choice of older adults and individuals with disabilities Represents the voice of the patient Identifies the self-management support needed to enhance patient and family engagement in their care

38
The Care Transitions Solution
Partnering with Beneficiary Service Organizations Define the Problem Discharge Process Mapping Cause & Effect Diagram (Fishbone) Data Driven Root-Cause Analysis Evidenced-Based Solutions Cost-Benefit Analysis Action Plan for Improvement Measure Intervention Results Sustain or Modify the Plan Home Health Hospitals Skilled Nursing Physicians Patients Partnering with Beneficiary Advocacy Groups Provider QI Community SNFs HHAs / ALFs Hospitals Outpatient Facilities MCOs (include payers role in speakers note for this slide)
 Data Driven Root-Cause Analysis. Evidenced-Based Solutions. Cost-Benefit Analysis. Action Plan for Improvement. Measure Intervention Results. Sustain or Modify the Plan. Home Health. Hospitals. Skilled Nursing. Physicians. Patients. Partnering with Beneficiary Advocacy Groups. Provider QI Community. SNFs. HHAs / ALFs. Hospitals. Outpatient Facilities. MCOs (include payers role in speakers note for this slide)")
39
CMS Partnership for Patients
Hospital Engagement Networks (HENs) Community-based Care Transitions Program (CCTP) Patient and family engagement (through HEN, CCTP, and QIO) Source:
 Community-based Care Transitions Program (CCTP) Patient and family engagement (through HEN, CCTP, and QIO) Source:")
40
26 Hospital Engagement Networks
8 of the 26 HENs are working with Florida Hospitals The Health Research & Educational Trust, an affiliate of the American Hospital Association (AHA) Ascension Health Intermountain Healthcare Joint Commission Resources, Inc. Lifepoint Hospitals, Inc. Premier UHC (formerly University Health System Consortium) VHA Source :
 Ascension Health. Intermountain Healthcare. Joint Commission Resources, Inc. Lifepoint Hospitals, Inc. Premier. UHC (formerly University Health System Consortium) VHA. Source :")
41
The Goals of the Hospital Engagement Networks (HENs)
Learning Collaboratives Patient Safety Training Technical Assistance Track & Monitor Progress Coach Hospitals to Serve as Leaders GOALS: Develop learning collaboratives for hospitals; Provide a wide array of initiatives & activities to improve patient safety; Conduct intensive training programs to help hospitals make patient care safer; Provide technical assistance to help hospitals achieve quality measurement goals; Establish & implement a system to track & monitor hospital progress in meeting quality improvement goals. Identify high performing hospitals and their leaders to coach and serve as national faculty to other hospitals. Source:

42
Community-based Care Transitions Program (CCTP)
The CCTP Partners – 5 in Florida Elder Options FL – Gainesville Catholic Health Care Transitions Services, Inc. − Lauderdale Lakes Osceola-St. Cloud Community-based Care Transitions Coalition The Greater Miami Coalition to Prevent Unnecessary Rehospitalizations FL West Central Florida Area Agency on Aging − Tampa

43
The Goals of the Community-Based Care Transitions Program
Improve Quality of Care Improve Care Transitions Reduce Readmissions Document Savings to Medicare GOALS: To improve transitions of beneficiaries from the inpatient hospital setting to other care settings To improve quality of care To reduce readmissions for high risk Medicare beneficiaries To document measurable savings to the Medicare program Source:

44
No Place Like Home Campaign
A campaign supported by a broad and growing base of stakeholders in the Florida healthcare community Focused on: Addressing the drivers of through the implementation of evidenced-based practices READMISSIONS

45
No Place Like Home Campaign (continued)
Shared Vision: A healthcare system where discharged patients: UNDERSTAND their conditions KNOW who to contact with questions (and when) ARE SUPPORTED by healthcare professionals who have access to the right information, at the right time
 ARE SUPPORTED by healthcare professionals who have access to the right information, at the right time.")
46
No Place Like Home Campaign (continued)
Aligns with the mission of the Aging Network to maximize independence for at-risk older adults and individuals with disabilities. Works across the continuum of care to reduce avoidable hospital readmissions in Florida. Works as an adjunct to existing programs. Seeks commitment from all Florida providers. Engages healthcare providers in local communities who work with patients post-discharge.

47
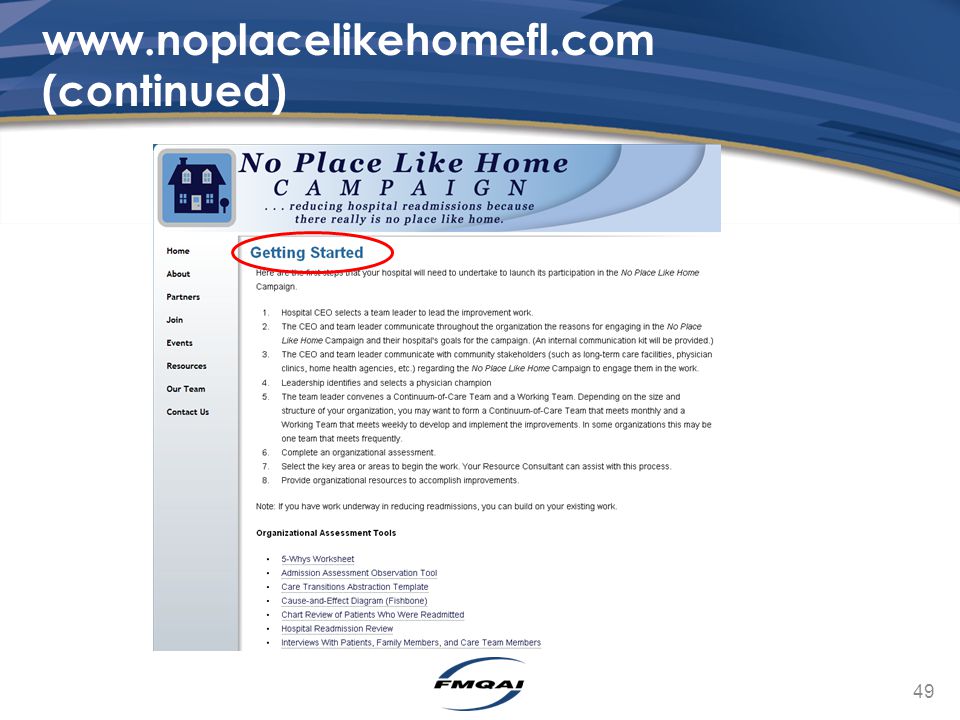
No Place Like Home Campaign Basics
Hospitals assign a multidisciplinary team Team lead, physician champion, and other team players Collect and analyze data Invite post-discharge providers to participate Skilled nursing facilities, home health, managed care organizations Develop and evaluate corrective actions using Plan, Do, Study, Act (PDSA) Implement successful corrective actions Share lessons learned throughout the organization and community
 Implement successful corrective actions. Share lessons learned throughout the organization and community.")
48
30-day All-Cause Readmissions by Regions
Source: Medicare fee-for-service claims for Florida inpatient discharges January 1, 2013 – June 30, 2013.

49
www.noplacelikehomefl.com (continued)
50
www.noplacelikehomefl.com (continued)
")
51
www.noplacelikehomefl.com (continued)
")
52
Moving From Competition To Collaboration
Taking risk (in this case, collaborating with your competition) can be the best opportunity for success and innovation. Create a strategic alliance with the goal of providing mutual benefit (e.g., improving the quality of patient centered care while reducing readmission rates). Recognize that improving care transitions and reducing readmissions takes time and commitment. Some challenges require “quick and easy” fixes while most others will take long-term dedication.
 can be the best opportunity for success and innovation. Create a strategic alliance with the goal of providing mutual benefit (e.g., improving the quality of patient centered care while reducing readmission rates). Recognize that improving care transitions and reducing readmissions takes time and commitment. Some challenges require quick and easy fixes while most others will take long-term dedication.")
53
Moving From Competition To Collaboration (continued)
Providers tend to have similar challenges but rarely have a chance to discuss these challenges across provider types. Identifying challenges within a community with all provider types represented at the table often starts with lots of finger pointing. Use other providers’ perspectives as learning opportunities. Challenges are likely interconnected between providers. Once everyone at the table decides to take ownership of the challenges as a community, actionable items arise. Include MCOs in speakers note for this slide.

54
Organizing: People, Power, & Change
Source: Colorado Foundation for Medical Care.

55
The ability to achieve purpose The ability to grow in capacity
What is Power? The ability to achieve purpose The ability to grow in capacity Source: Adapted from ReThink Health.

56
Building Relationships
Source: Colorado Foundation for Medical Care.

57
One to One Meeting Source: Colorado Foundation for Medical Care.

58
Collective Impact Conditions needed to foster change through collective impact: Shared agenda Common, consistent measurement Mutually reinforced activities Continuous, two-way communication Backbone support A shared agenda: All participants have a shared vision for change (including the problem and approach). Consistent and common measurement: All participants remain aligned and hold each other accountable. Mutually reinforced activities: Participant activities must be differentiated while still being coordinated through a mutually reinforcing plan of action Continuous, two-way communication: consistent and open communication is needed across players to build trust, assure mutual objectives, and appreciate common motivation. Backbone support: Creating and managing collective impact requires a separate organization (e.g., CBOs) to serve as the backbone for the initiative and coordinate participating organizations and agencies. Source: Hanleybrown F, Kania J, Kramer M. Channeling change: Making collective impact work. Stanford Social Innovation Review;2012.
. Consistent and common measurement: All participants remain aligned and hold each other accountable. Mutually reinforced activities: Participant activities must be differentiated while still being coordinated through a mutually reinforcing plan of action. Continuous, two-way communication: consistent and open communication is needed across players to build trust, assure mutual objectives, and appreciate common motivation. Backbone support: Creating and managing collective impact requires a separate organization (e.g., CBOs) to serve as the backbone for the initiative and coordinate participating organizations and agencies. Source: Hanleybrown F, Kania J, Kramer M. Channeling change: Making collective impact work. Stanford Social Innovation Review;2012.")
59
What To Do By Next Tuesday?
Leave in Action: Save the Date – April 11, 2014 Join HealthHub What is a request or offer you would like to make? “If you want to go quickly, go alone. If you want to go far, go together.” -African proverb

60
Questions Ferdinand Richards III, MD frichards@fmqai.com 813-865-3584
Peggy Loesch, BSN, MBA, RN This material was prepared by FMQAI, the Medicare Quality Improvement Organization for Florida, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the Department of Health and Human Services (HHS). The contents presented do not necessarily reflect CMS policy. FL-201X10SOW-XXXXXX-XX-XXXX
, an agency of the Department of Health and Human Services (HHS). The contents presented do not necessarily reflect CMS policy. FL-201X10SOW-XXXXXX-XX-XXXX.")
Similar presentations









 Program.>")



![[Hospital Name | Presenter name and title | Date of presentation]](/19/5722524/big_thumb.jpg "[Hospital Name | Presenter name and title | Date of presentation]>")





