Download presentation
Presentation is loading. Please wait.

1
Multiple Sclerosis for the Non-Specialist
Keith Cushing, M.D. Board Certified, Neurology JWM Neurology

2
Disclosures: None

3
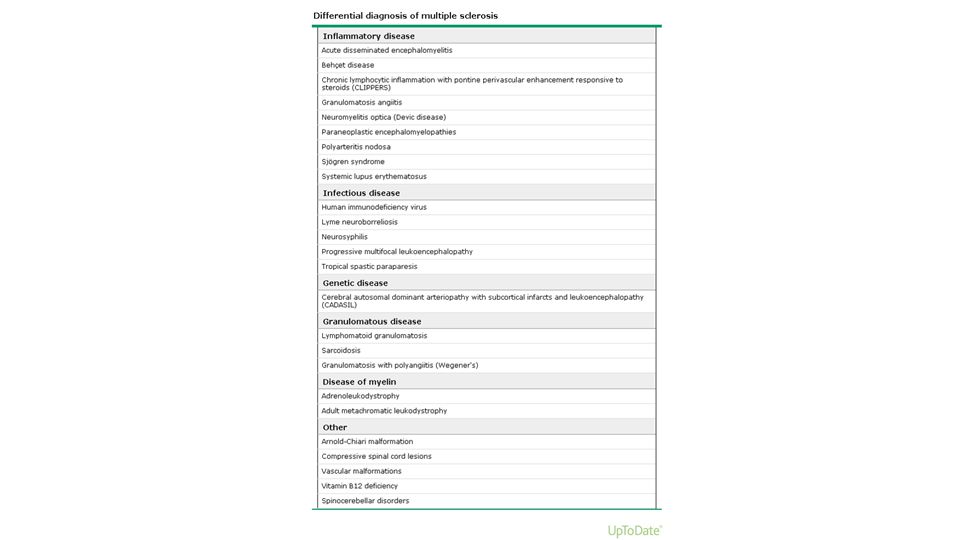
Topic Outline: Multiple Sclerosis
Epidemiology and Demographics Pathophysiology Diagnosis and Differential Treatment Options

4
MS: A brief history first described by French
neurologist Charcot in 1868: “la sclérose en plaques disséminées” named for the scattered, firm, sclerotic plaques seen post-mortem in the brain and spinal cord

5
Epidemiology and Demographics
more common in women than men mean age of onset 30 years peak age of onset 5 years earlier in women than men Source: Up-to-Date,” Epidemiology and clinical features of multiple sclerosis in adults”

6
Epidemiology and Demographics
incidence and prevalence varies geographically high prevalence areas all of Europe, including Russia southern Canada northern U.S. New Zealand southeast Australia lowest risk people of Asian, African, or American Indian origin supposed latitudinal gradient of MS incidence has been recently challenged Source: Up-to-Date,” Epidemiology and clinical features of multiple sclerosis in adults”

7
Epidemiology and Demographics
no association between vaccines and MS though many viruses, including EBV, have been linked, there is no specific evidence linking them directly to the development of MS Source: Up-to-Date,” Epidemiology and clinical features of multiple sclerosis in adults”

8
Epidemiology and Demographics
Genetic factors appear to contribute to the pathogenesis of MS, particularly variation involving the HLA-DRB1 locus Chronic cerebrospinal venous insufficiency has been reported in some patients with MS but its relationship to MS is controversial Source: Up-to-Date,” Epidemiology and clinical features of multiple sclerosis in adults”

9
Natural History Progression of disability due to MS is highly variable, but accumulating evidence suggests that progression in most patients with MS is slow. At the extreme ends of the severity spectrum, there are benign and malignant forms of MS. Source: Up-to-Date,” Epidemiology and clinical features of multiple sclerosis in adults”

10
Natural History Benign MS refers to disease in which the patient remains fully functional in all neurologic systems 15 years after the disease onset. Malignant MS refers to disease with a rapid progressive course, leading to significant disability in multiple neurologic systems or death in a relatively short time after disease onset Source: Up-to-Date,” Epidemiology and clinical features of multiple sclerosis in adults”

11
MS Pathophysiology

12
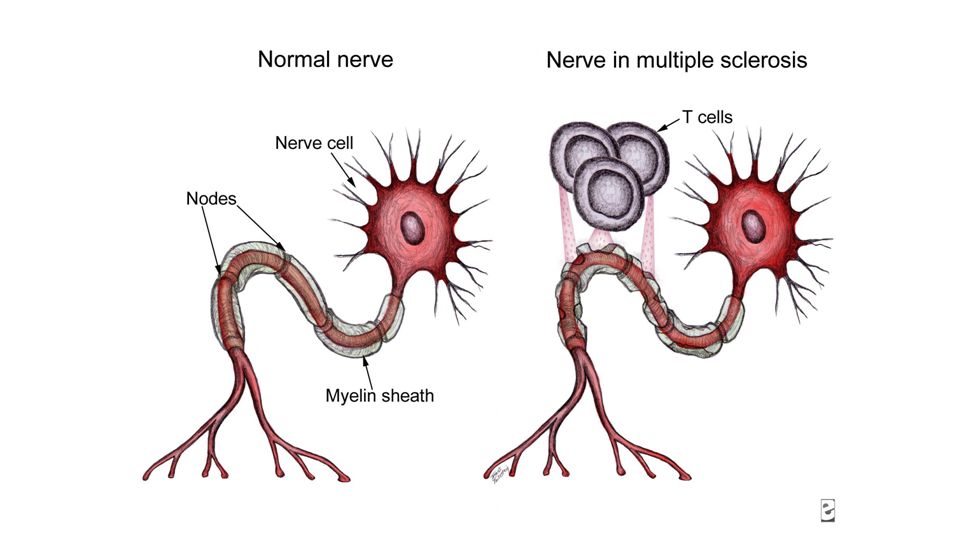
MS: Pathophysiology the precise etiology of MS has not yet been determined pathologic hallmark is multiple focal areas of myelin loss within the CNS it is these areas that are referred to as plaques or lesions Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
13
Pathophysiology myelin loss is typically accompanied by gliosis and inflammation and by relative preservation of the axons Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
15
Pathophysiology active MS lesions are infiltrated by
macrophages containing myelin debris Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
16
Pathophysiology lymphocytic inflammatory infiltrates in MS are composed mainly of CD8+ cytotoxic T cells less so, CD4+ helper T cells, B cells, and plasma cells Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
17
Pathophysiology Gadolinium MRI enhancement
characterizes lesions with a damaged blood-brain barrier, which enables the infiltration of inflammatory cells into the CNS Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
18
Pathophysiology: Heterogeneity
active lesions show a profound pathologic heterogeneity and can be classified into four immunopatterns, suggesting that the targets of injury and the mechanisms of demyelination are distinct in different disease subgroups Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
19
Pathophysiology: Axonal Injury
Although demyelination appears to be the dominant process, axonal injury occurs in multiple sclerosis and is most pronounced during active inflammatory demyelination acute axonal injury occurring in early multiple sclerosis lesions likely contributes to the relapse-related disability observed predominantly during the inflammatory disease phases Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
20
Pathophysiology neurodegeneration is present in demyelinated lesions and is invariably associated with inflammation in chronic inactive lesions from aged patients with long-standing progressive multiple sclerosis where the inflammatory process has died out, the neurodegeneration is also reduced to levels seen in control patients. Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
21
Pathophysiology Extensive remyelination, illustrated by the presence of newly formed myelin sheaths and oligodendrocyte precursor cells, is frequently encountered within active plaques of early multiple sclerosis. Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
22
Pathophysiology Cortical demyelinated lesions are present and common in early multiple sclerosis these lesions are highly inflammatory they may represent the pathologic substrate of cognitive impairment and epilepsy in relapsing-remitting multiple sclerosis. Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
23
Pathophysiology The presence of inflammatory cortical demyelination in early multiple sclerosis argues against a primary neurodegenerative process at this stage of disease this process suggests that neuronal and axonal injury in early cortical demyelination occur on a background of inflammation. Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
24
Pathophysiology Meningeal inflammation is present in early multiple sclerosis and topographically associated with cortical lesions it may drive the cortical demyelination but also set the stage for subsequent subcortical white matter inflammation and demyelination. Popescu, Bogdan F. Gh. MD, PhD; Pirko, Istvan MD, FAAN; Lucchinetti, Claudia F. MD, FAAN. Pathology of Multiple Sclerosis: Where Do We Stand?. CONTINUUM: Lifelong Learning in Neurology. 2013; 19: (4):
:")
25
MS: Diagnostic Subtypes
relapsing-remitting primary progressive secondary progressive

26
Diagnosis and Differential
The majority of patients diagnosed with multiple sclerosis (MS) (80% to 85%) follow an initial relapsing-remitting course characterized by episodes with fairly rapid onset of new or recurrent neurologic deficits followed by partial or complete recovery. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 (80% to 85%) follow an initial relapsing-remitting course characterized by episodes with fairly rapid onset of new or recurrent neurologic deficits followed by partial or complete recovery. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
27
Diagnosis and Differential: The Bible
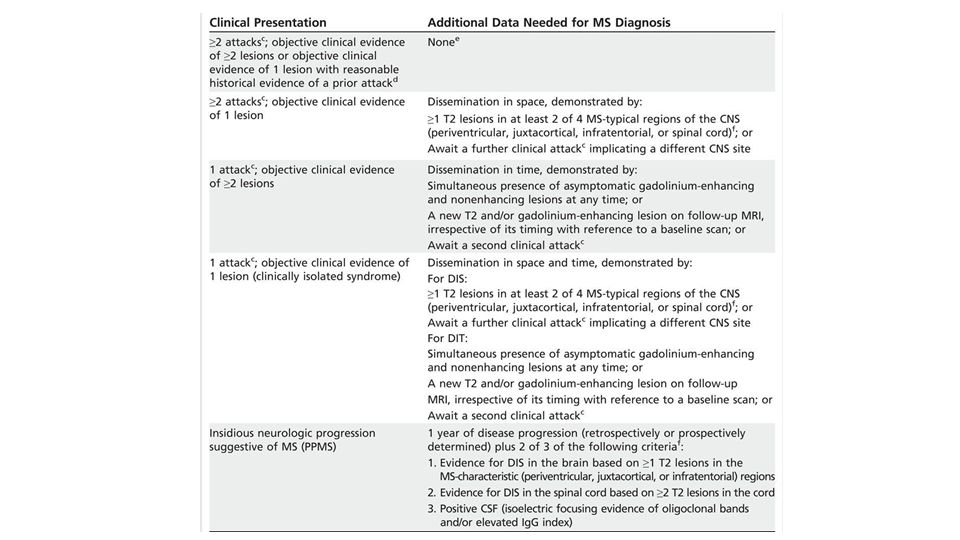
McDonald Criteria first published in 2001 2005 revision 2010 revision Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
28
Diagnosis and Differential
All recent formulations of the diagnostic criteria begin with an initial clinical presentation that includes symptoms typical for a multiple sclerosis attack (also called a relapse or exacerbation) This initial presentation has been termed the “clinically isolated syndrome” (CIS) Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 This initial presentation has been termed the clinically isolated syndrome (CIS) Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
29
Diagnosis and Differential
The McDonald 2010 panel defined an attack as: patient-reported symptoms or objectively observed signs typical of an acute inflammatory demyelinating event in the CNS current or historical with duration of at least 24 hours in the absence of fever or infection Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
30
Diagnosis and Differential
For paroxysmal symptoms (such as paroxysmal dysarthria, tonic spasms, or paroxysmal sensory symptoms) to be considered an attack, symptoms must be recurrent over at least 24 hours. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 to be considered an attack, symptoms must be recurrent over at least 24 hours. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
31
Diagnosis and Differential
Once multiple sclerosis has been established as the most likely etiology of the symptoms, the clinician must evaluate for evidence of: dissemination in space, which requires involvement of multiple areas of the CNS dissemination in time, which requires ongoing disease activity over time. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
32
Diagnosis and Differential
DIS criteria may be satisfied on clinical grounds alone if the patient has: objective clinical evidence of involvement of at least two CNS sites or objective clinical evidence of one lesion with reasonable historical evidence of another site being affected. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
33
Diagnosis and Differential
Objective clinical evidence may include: findings on neurologic examination abnormal visual evoked potentials in a patient with a history of visual loss evidence of a demyelinating lesion on MRI that would explain prior symptoms. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
34
Diagnosis and Differential
If there is only objective clinical evidence of one lesion, DIS may be established by applying the MRI criteria. The revised McDonald 2010 DIS MRI criteria are based on recommendations from the European multicenter collaborative research network that studies MRI in MS (MAGNetic Resonance In Multiple Sclerosis, or MAGNIMS) Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
35
Diagnosis and Differential
Dissemination-in-space MRI criteria now require at minimum only two lesions: at least one T2 lesion in at least two of the four sites typically affected by multiple sclerosis (periventricular, juxtacortical, infratentorial, or spinal cord).
.")
36
Diagnosis and Differential
DIT criteria may be satisfied on clinical grounds alone if the patient has a history of at least two attacks If the patient has a history of one attack, MRI criteria may be applied to establish DIT. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
37
Diagnosis and Differential
Under the 2010 criteria, DIT can be established with the development of a new T2 lesion at any time, compared to a baseline scan performed at any time In certain cases, DIT can actually be established with a single MRI scan Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
38
Diagnosis and Differential
Dissemination in time can be demonstrated with a single MRI if simultaneous asymptomatic gadolinium-enhancing and nonenhancing lesions are present.

40
Diagnosis and Differential
Primary progressive multiple sclerosis: characterized by the insidious onset of symptoms followed by gradual deterioration over time Clinical disease in these patients typically presents as a progressive myelopathy, and less frequently as a brainstem or cerebellar syndrome. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
41
Diagnosis and Differential
Secondary progressive multiple sclerosis: diagnosed when, after an initial relapsing-remitting course, a patient demonstrates disease progression independent of relapses for at least 6 months. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
42
Diagnosis and Differential
Radiologically isolated syndrome: diagnosed when a patient is incidentally found to have imaging findings suggestive of multiple sclerosis, which are not better explained by another medical condition, in the absence of clinical symptoms.

43
Diagnosis and Differential
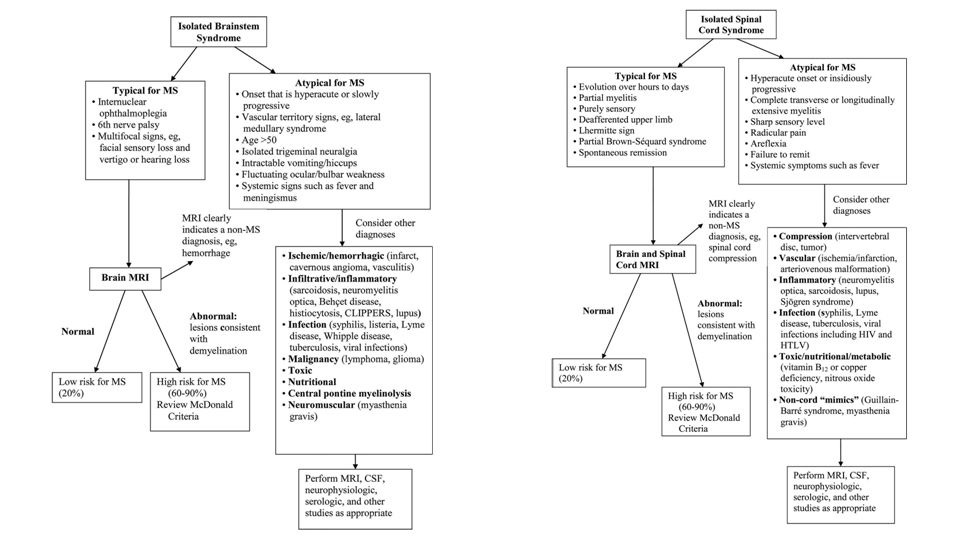
if any element of the: clinical history examination imaging is atypical, additional testing to exclude other etiologies is warranted. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
44
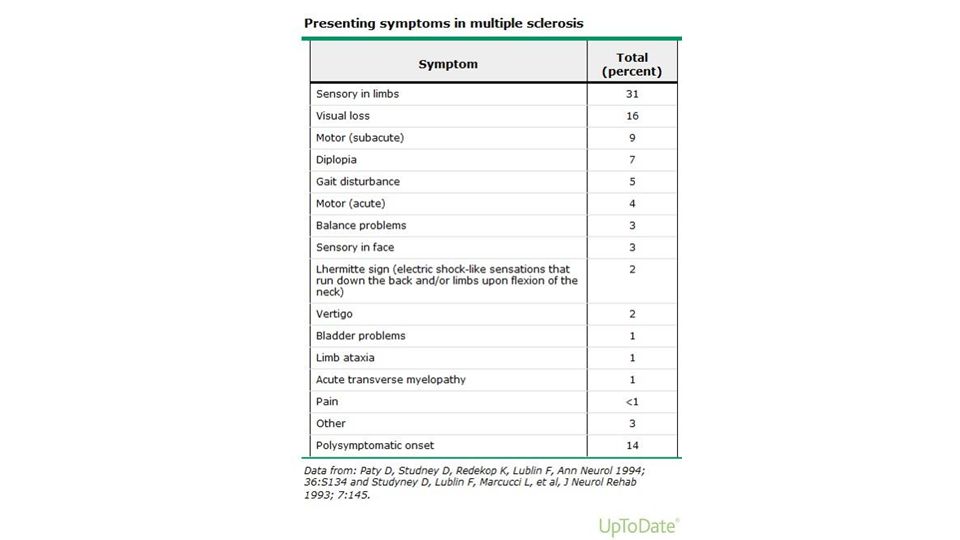
There are no clinical findings that are unique to MS, but some are highly characteristic of the disease

47
Diagnosis and Differential
A classic presentation of a brainstem syndrome suggestive of clinically isolated syndrome is diplopia due to internuclear ophthalmoplegia, which is often bilateral. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
48
Diagnosis and Differential
Patients with optic neuritis related to underlying multiple sclerosis typically present with painful, subacute, unilateral visual loss that manifests as visual blurring or a scotoma.

49
Diagnosis and Differential
Patients with a spinal cord syndrome suggestive of clinically isolated syndrome characteristically present with a partial transverse myelitis, which is usually dominated by sensory symptoms. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
50
Diagnosis and Differential
On MRI, spinal cord lesions due to multiple sclerosis are typically peripheral, with the dorsolateral cord being the most common plaque location. Multiple sclerosis lesions are usually less than two vertebral segments in length and occupy less than half of the cross-sectional cord area. Katz Sand, Ilana B. MD; Lublin, Fred D. MD, FAAN, FANA. Diagnosis and Differential Diagnosis of Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
:")
51
Lhermitte sign electric shock-like sensations that run down the back and/or limbs upon flexion of the neck

52
Uhthoff phenomenon small increases in the body temperature can temporarily worsen current or preexisting signs and symptoms This phenomenon is presumably the result of conduction block developing in central pathways as the body temperature increases

55
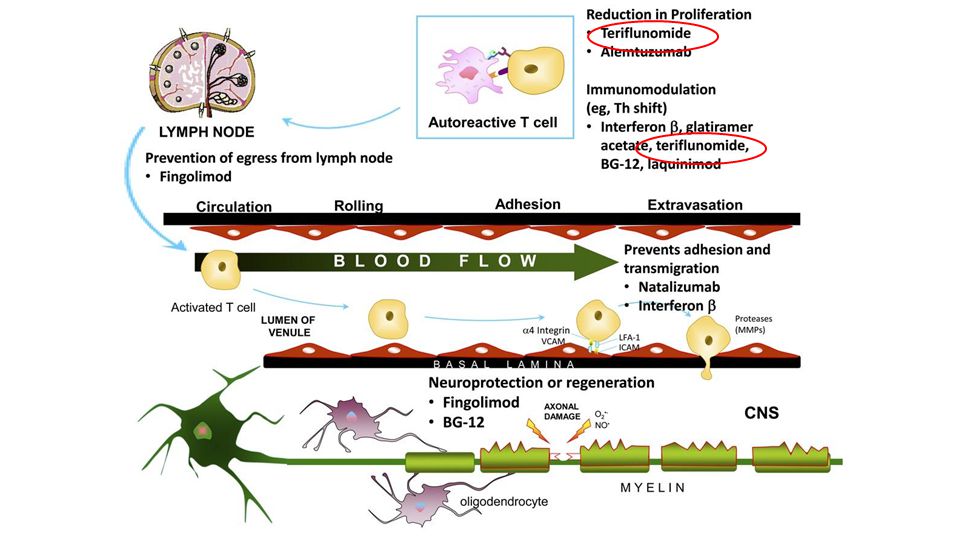
MS Therapies: Interferon beta
available since 1993 four preparations now available Rebif (subcutaneous interferon beta 1a, 3x/week) Betaseron (subcutaneous interferon beta 1b, every other day) Avonex (intramuscular interferon beta 1a, once a week) Extavia (subcutaneous interferon beta 1b, every other day) Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 Betaseron (subcutaneous interferon beta 1b, every other day) Avonex (intramuscular interferon beta 1a, once a week) Extavia (subcutaneous interferon beta 1b, every other day) Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
56
MS Therapies: Interferon beta
Mechanism of Action: modulates T-cell and B-cell function decreases expression of matrix metalloproteinases reverses blood-brain barrier disruption alters expression of a number of cytokines Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
57
Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C)
Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
58
MS Therapies: Interferon beta
Evidence: A series of phase 3 studies in relapsing MS support the benefit of IFN-β in reducing relapses (by approximately 30%) disability progression MRI lesion activity and accrual Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 disability progression. MRI lesion activity and accrual. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
59
MS Therapies: Interferon beta
Side Effects: flulike symptoms (eg, fever, chills, malaise, myalgia) after injection sometimes with concomitant worsening of preexisting neurologic symptoms These symptoms usually last from several to 24 hours after injection and are worse with the initiation of therapy In most cases they attenuate over time Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 after injection. sometimes with concomitant worsening of preexisting neurologic symptoms. These symptoms usually last from several to 24 hours after injection and are worse with the initiation of therapy. In most cases they attenuate over time. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
60
MS Therapies: Interferon beta
Side Effects (continued): injection-site reactions rare skin necrosis depression leukopenia liver abnormalities thyroid disorders patients with preexisting headache syndromes or spasticity may experience a worsening of these symptoms with IFN-β therapy Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
: injection-site reactions. rare skin necrosis. depression. leukopenia. liver abnormalities. thyroid disorders. patients with preexisting headache syndromes or spasticity may experience a worsening of these symptoms with IFN-β therapy. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
61
MS Therapies: Glatiramer Acetate
Mechanism of Action: complex mixture of random synthetic polypeptides probably functions as an altered peptide ligand for the major histocompatibility complex (MHC) class II molecules may also stimulate neuroprotective or repair mechanisms Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 class II molecules. may also stimulate neuroprotective or repair mechanisms. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
63
MS Therapies: Glatiramer Acetate
Evidence: Two phase 3 studies demonstrated that GA 20 mg/d administered by subcutaneous injection reduced annualized relapse rate (ARR) with a reduction of approximately 30% in the second study A separate randomized controlled trial demonstrated a benefit in MRI measures, including gadolinium-enhancing lesions, new T2 lesions, and the proportion of lesions evolving into T1-hypointense “black holes.” Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 with a reduction of approximately 30% in the second study. A separate randomized controlled trial demonstrated a benefit in MRI measures, including gadolinium-enhancing lesions, new T2 lesions, and the proportion of lesions evolving into T1-hypointense black holes. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
64
MS Therapies: Glatiramer Acetate
Side Effects: injection-site tenderness pruritus erythema induration Lipoatrophy (loss of subcutaneous fat with scarring) Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
65
MS Therapies: Glatiramer Acetate
Side Effects: occasionally causes a postinjection systemic reaction comprising various combinations of flushing, diaphoresis, chest tightness, dyspnea, palpitations, and anxiety begins within minutes of injection and resolves spontaneously in 1 to 30 minutes reaction typically occurs once or at most a few times in a given patient and does not recur with continued dosing

66
MS Therapies: Glatiramer Acetate
In contrast to IFN-β, GA is not associated with constitutional side effects depression liver enzyme abnormalities low blood counts worsening headaches spasticity neutralizing antibodies Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
67
MS Therapies: Natalizumab
Mechanism of Action: a humanized monoclonal antibody binds α4-integrin and blocks interaction of α4β1-integrin on leukocytes with vascular cell adhesion molecules and connecting segment-1 (CS-1) on fibronectin sites on vascular endothelial cells As a result, migration of leukocytes from the blood into the CNS is inhibited Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 on fibronectin sites on vascular endothelial cells. As a result, migration of leukocytes from the blood into the CNS is inhibited. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
69
MS Therapies: Natalizumab
Evidence: phase 3 trial showed that monthly IV infusions of 300 mg natalizumab reduced ARR by 68% over 2 years disability progression by 42% MRI gadolinium-enhancing lesion number by 92%, relative to the study placebo group Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
70
MS Therapies: Natalizumab
A second phase 3 study supported these results, showing that natalizumab combined with IFN-β-1a IM was more effective than IFN-β-1a IM plus placebo infusions Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
71
MS Therapies: Natalizumab
Natalizumab is generally considered for: patients who have relapsing MS and continued disease activity despite use of one or more of the standard disease therapies or who are intolerant of the standard agents It also can be considered for patients with disease characteristics that suggest high risk of disability and for whom a more potent although potentially more risky agent is felt to be appropriate

72
MS Therapies: Natalizumab
Side Effects: anxiety fatigue pharyngitis sinus congestion peripheral edema infusion-related symptoms (headache, flushing, erythema, nausea, fatigue, and dizziness).
.")
73
MS Therapies: Natalizumab
Allergic hypersensitivity reactions, including anaphylaxis, urticaria, pruritus, and anaphylactoid syndromes, occurred in 4% of natalizumab-treated patients and were serious in 1%. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
74
MS Therapies: Natalizumab
key safety concern is an increased risk for PML, a concern that did not surface during the course of the original trials This is a serious, often fatal opportunistic infection of oligodendrocytes caused by reactivation of latent John Cunningham (JC) polyomavirus
 polyomavirus.")
75
MS Therapies: Natalizumab
MRI is performed before treatment and intermittently during natalizumab therapy Manifestations that suggest PML include subacutely worsening visual, motor, or cognitive changes and/or gradually enlarging T2 hyperintensities with minimal or no gadolinium enhancement If PML is suspected, natalizumab treatment should be suspended, MRI obtained, and CSF examination performed, including PCR for JC virus.

76
Recently Introduced Oral Therapies
Fingolimod (Gilenya) Teriflunomide (Aubagio) Dimethyl Fumarate (Tecfidera)
 Teriflunomide (Aubagio) Dimethyl Fumarate (Tecfidera)")
77
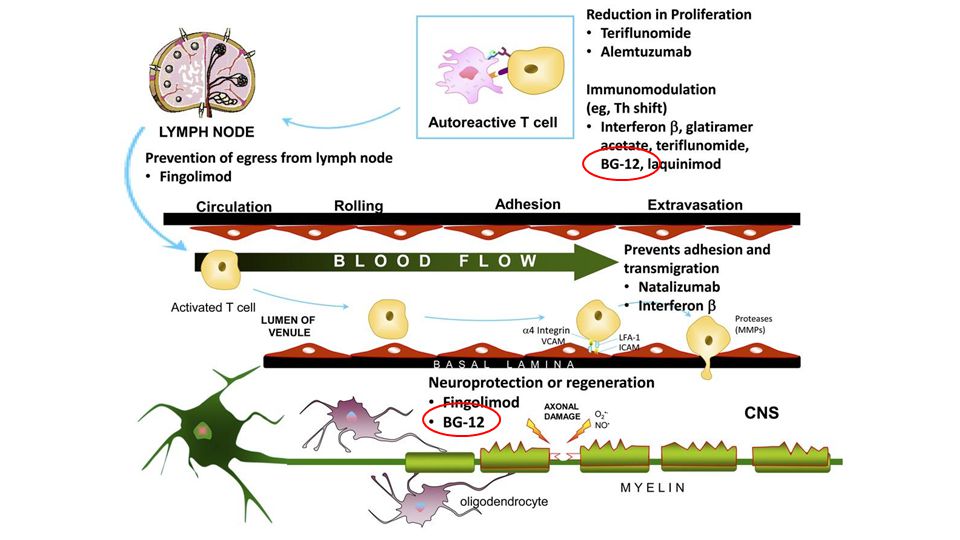
MS Therapies: Fingolimod
the first oral drug to receive North American and European regulatory approval to reduce relapses in patients with relapsing MS.

78
MS Therapies: Fingolimod
Mechanism of Action: sphingosine-1-phosphate receptor (S1P1) modulator that has immunoregulatory features inhibits the migration of T cells from lymphoid tissue into the peripheral circulation and target organs, including the CNS Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 modulator that has immunoregulatory features. inhibits the migration of T cells from lymphoid tissue into the peripheral circulation and target organs, including the CNS. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
80
MS Therapies: Fingolimod
Evidence: (FTY720 Research Evaluating Effects of Daily Oral Therapy in Multiple Sclerosis [FREEDOMS], a placebo-controlled 24-month trial Trial Assessing Injectable Interferon versus FTY720 Oral in Relapsing-Remitting Multiple Sclerosis [TRANSFORMS] a 12-month head-to-head trial with comparator IFN-β-1a IM) demonstrated that orally administered fingolimod (0.5 mg/d) was effective and superior to IFN-β-1a IM at reducing ARR and MRI activity in patients with relapsing MS
 demonstrated that orally administered fingolimod (0.5 mg/d) was effective and superior to IFN-β-1a IM at reducing ARR and MRI activity in patients with relapsing MS.")
81
MS Therapies: Fingolimod
Although fingolimod is generally well tolerated, specific safety issues have been identified: first-dose bradycardia the possible risk of herpes virus dissemination macular edema long-term consequences of elevated blood pressure) Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
82
MS Therapies: Fingolimod
Further long-term data are needed to assess the safety profile of fingolimod Of clinical concern is a patient started on fingolimod who died on the second day of treatment Further analysis of this and other cases led to a more stringent set of criteria for fingolimod therapy and more careful first-dose observation Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
83
MS Therapies: Teriflunomide
Mechanism of Action: Derived directly from leflunomide an antimetabolite that interferes with the de novo synthesis of pyrimidines, sparing the salvage pathway, by inhibiting the mitochondrial enzyme dihydro-orotate dehydrogenase This has the effect of blocking cell replication in rapidly dividing cells, but the exact mechanism by which this translates into efficacy for MS is unknown Typically, the cells that are more involved in mediating autoimmune processes will be more susceptible to the antimetabolite effects of teriflunomide.

85
MS Therapies: Teriflunomide
Evidence: (the Teriflunomide Multiple Sclerosis Oral [TEMSO] trial) showed a significant effect on the primary outcome of relapse rate secondary outcomes on MRI and disability (Expanded Disability Status Scale [EDSS] progression) also reached statistical significance over placebo Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 showed a significant effect on the primary outcome of relapse rate. secondary outcomes on MRI and disability (Expanded Disability Status Scale [EDSS] progression) also reached statistical significance over placebo. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
86
MS Therapies: Teriflunomide
Other Teriflunomide Studies: The Teriflunomide Oral in People with Relapsing- Remitting Multiple Sclerosis (TOWER) A Study Comparing the Effectiveness and Safety of Teriflunomide and Interferon-β-1a in Patients with Relapsing Multiple Sclerosis (TENERE) Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 A Study Comparing the Effectiveness and Safety of Teriflunomide and Interferon-β-1a in Patients with Relapsing Multiple Sclerosis (TENERE) Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
87
MS Therapies: Teriflunomide
Side Effects and Safety: Hair thinning gastrointestinal upset The potential for teratogenicity has come from preclinical studies, which is of particular concern in women of childbearing potential A specific washout program using cholestyramine or activated charcoal can be used to remove teriflunomide from the system; however, without this washout, teriflunomide may remain in the system for months after the last dose Careful counseling is therefore recommended in women of childbearing age contemplating teriflunomide.

88
MS Therapies: Dimethyl Fumarate
fumaric acid ester that can be taken orally and is immediately hydrolyzed by esterases to its metabolite monomethyl fumarate (MMF) DMF is better tolerated than MMF, as it is associated with lower gastrointestinal side effects BG-12 is a formulation of DMF manufactured as an enteric-coated microtablet to improve gastrointestinal tolerability Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 DMF is better tolerated than MMF, as it is associated with lower gastrointestinal side effects. BG-12 is a formulation of DMF manufactured as an enteric-coated microtablet to improve gastrointestinal tolerability. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
89
MS Therapies: Dimethyl Fumarate
The exact mechanism by which it exerts its positive anti-inflammatory effects is unknow It may act on the major transcription factor known as nuclear factor erythroid 2–related factor 2 (Nrf-2), which is released from binding to kelch- like ECH-associated protein 1 (Keap-1) via the activity of DMF In turn, Nrf-2 upregulates an array of antioxidative pathways, such as increased glutathione levels Nrf-2 pathway activation also leads to an inhibition of the translocation of nuclear factor-κB into the nucleus, which would normally turn on the expression of a cascade of inflammatory cytokines, chemokines, and adhesion molecules
, which is released from binding to kelch- like ECH-associated protein 1 (Keap-1) via the activity of DMF. In turn, Nrf-2 upregulates an array of antioxidative pathways, such as increased glutathione levels. Nrf-2 pathway activation also leads to an inhibition of the translocation of nuclear factor-κB into the nucleus, which would normally turn on the expression of a cascade of inflammatory cytokines, chemokines, and adhesion molecules.")
91
MS Therapies: Dimethyl Fumarate
Determination of the Efficacy and Safety of Oral Fumarate in Relapsing-Remitting Multiple Sclerosis (DEFINE)31 was one of two large phase 3 studies comparing two doses of BG-12 to placebo 1234 patients with relapsing MS and EDSS scores of 5.0 or lower were randomized to receive placebo (n = 408) or 240 mg of BG-12 twice a day (n = 410) or 3 times a day (n = 416) clinic visits were every 12 weeks MRI studies were performed at baseline, 24, 48, and 96 weeks in a subgroup of patients (n = 540).
31 was one of two large phase 3 studies comparing two doses of BG-12 to placebo patients with relapsing MS and EDSS scores of 5.0 or lower were randomized to receive placebo (n = 408) or 240 mg of BG-12 twice a day (n = 410) or 3 times a day (n = 416) clinic visits were every 12 weeks. MRI studies were performed at baseline, 24, 48, and 96 weeks in a subgroup of patients (n = 540).")
92
MS Therapies: Dimethyl Fumarate
The primary outcome was the proportion of patients relapsing at 2 years the difference in ARR and the risk for disability progression (measured by EDSS scores) were considered secondary outcome measures in this study Both doses of BG-12 reduced the proportion of patients relapsing by nearly 50% (P<.001) Whereas 46% of placebo patients relapsed, only 27% of the patients dosed with BG-12 twice a day and 26% of those dosed 3 times a day had at least one relapse by 2 years (P<.001 for both comparisons).
 were considered secondary outcome measures in this study. Both doses of BG-12 reduced the proportion of patients relapsing by nearly 50% (P<.001) Whereas 46% of placebo patients relapsed, only 27% of the patients dosed with BG-12 twice a day and 26% of those dosed 3 times a day had at least one relapse by 2 years (P<.001 for both comparisons).")
93
MS Therapies: Dimethyl Fumarate
BG-12 twice a day reduced the ARR relative to the placebo population by 53% and BG-12 3 times a day by 48% (P<.001 for both comparisons) EDSS progression confirmed at 12 weeks was also reduced by both dosing regimens: whereas 27% of patients treated with placebo progressed, only 16% of those treated twice a day with BG-12 and 18% of those treated 3 times a day with BG-12 did so, a relative reduction of 38% and 34%, respectively New or newly enlarging MRI lesions were also substantially reduced by both doses: 85% and 74% for BG-12 twice a day and 3 times a day, respectively, versus placebo (P<.001 for both comparisons).
 EDSS progression confirmed at 12 weeks was also reduced by both dosing regimens: whereas 27% of patients treated with placebo progressed, only 16% of those treated twice a day with BG-12 and 18% of those treated 3 times a day with BG-12 did so, a relative reduction of 38% and 34%, respectively. New or newly enlarging MRI lesions were also substantially reduced by both doses: 85% and 74% for BG-12 twice a day and 3 times a day, respectively, versus placebo (P<.001 for both comparisons).")
95
MS Therapies: Dimethyl Fumarate
Potential negative aspects include the twice a day dosing initial gastrointestinal and flushing symptoms Fumaderm or its generic equivalent, a combination of fumaric acid esters, has been available in Germany and Europe but only recently was associated with a few cases of PML in patients treated mainly for psoriasis.33 Whether BG-12 will turn out to have similar problems remains to be determined.

96
MS Therapies: Other Therapies
Laquinimod Alemtuzumab Daclizumab Ocrelizumab

97
MS Therapies: Caveats Experience with interferon-β and glatiramer acetate over several decades has assured us of their relative safety in the general public of unselected patients with multiple sclerosis The same cannot be said of all of the newer agents Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
98
MS Therapies: Caveats Safety in a carefully selected study set of patients cannot predict how a disease-modifying drug will do when given more generally to unselected patients Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
99
MS Therapies: Caveats Although all agents are tested primarily for their ability to reduce relapses, in populations with low relapse rates, supportive effects are also sought from efficacy on other metrics such as MRI and Expanded Disability Status Scale progression Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
. Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
100
MS Therapies: Caveats Given how few head-to-head trials have been conducted, comparing efficacy among disease-modifying drugs is difficult, so the indication (first- or second-line) comes from the risk profile, with riskier agents relegated to a higher tier Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):
 comes from the risk profile, with riskier agents relegated to a higher tier. Freedman, Mark S. MSc, MD, FAAN, FANA, FRCP(C). Present and Emerging Therapies for Multiple Sclerosis. CONTINUUM: Lifelong Learning in Neurology. 2013; 19:(4):")
101
MS Therapies: Caveats Although newer agents appeal because of convenience (eg, oral dosing) or the perception that they demonstrate superior efficacy to long-standing interferon-β or glatiramer acetate, few data support this Recent studies show annualized relapse rates for interferon-β or glatiramer acetate in the same range as some of the newer agents.
 or the perception that they demonstrate superior efficacy to long-standing interferon-β or glatiramer acetate, few data support this. Recent studies show annualized relapse rates for interferon-β or glatiramer acetate in the same range as some of the newer agents.")
102
MS Therapies: Caveats Not all patients present with the same amount of disease or carry the same risk of progression Risk factors such as disease course, type of relapse and residual disability, MRI burden of disease, or even response to previous disease-modifying drugs must be taken into account when considering a choice for therapy.

Similar presentations







 Recent evidence shows early involvement of CNS axons as.>")





 & Multiple Sclerosis>")




 tumors arising from one of the many different cell types within.>")





