Download presentation
Presentation is loading. Please wait.

2
Case A 46-year-old man with severe vertigo, nausea, and vomiting was brought to the emergency department. She reported that she had felt slightly dizzy when she got out of bed that morning, and that during the next several hours, she had experienced increasing vertigo(illusion in rotation way) and nausea, and eventually vomiting. Her balance was impaired and she was having difficulty focusing her eyes--"everything seems to be jumping back and forth." with vertical displacement of objects. There was no hearing loss or other ear symptoms. Her history was significant only for mild hypertension. A 46-year-old man with severe vertigo, nausea, and vomiting was brought to the emergency department. She reported that she had felt slightly dizzy when she got out of bed that morning, and that during the next several hours, she had experienced increasing vertigo(illusion in rotation way) and nausea, and eventually vomiting. Her balance was impaired and she was having difficulty focusing her eyes--"everything seems to be jumping back and forth." with vertical displacement of objects. There was no hearing loss or other ear symptoms. Her history was significant only for mild hypertension.
 and nausea, and eventually vomiting. Her balance was impaired and she was having difficulty focusing her eyes-- everything seems to be jumping back and forth. with vertical displacement of objects. There was no hearing loss or other ear symptoms. Her history was significant only for mild hypertension. A 46-year-old man with severe vertigo, nausea, and vomiting was brought to the emergency department. She reported that she had felt slightly dizzy when she got out of bed that morning, and that during the next several hours, she had experienced increasing vertigo(illusion in rotation way) and nausea, and eventually vomiting. Her balance was impaired and she was having difficulty focusing her eyes-- everything seems to be jumping back and forth. with vertical displacement of objects. There was no hearing loss or other ear symptoms. Her history was significant only for mild hypertension..")
3
examination blood pressure was 150/80 mm Hg; her pulse was 88 b.p.m and regular, dehydrated from repeated vomiting. blood pressure was 150/80 mm Hg; her pulse was 88 b.p.m and regular, dehydrated from repeated vomiting. The patient was able to stand and walk, although she tended to veer to the right and was obviously unsteady. He had a brisk spontaneous nystagmus that was horizontal-torsional ; increased in amplitude when she looked to the left and decreased when she looked to the right, but did not change direction. The patient was able to stand and walk, although she tended to veer to the right and was obviously unsteady. He had a brisk spontaneous nystagmus that was horizontal-torsional ; increased in amplitude when she looked to the left and decreased when she looked to the right, but did not change direction. Cover-uncover testing indicated the presence of skew deviation, with the right eye slightly lower than the left in all directions of gaze. Cover-uncover testing indicated the presence of skew deviation, with the right eye slightly lower than the left in all directions of gaze. The remainder of the physical examination was unremarkable. The remainder of the physical examination was unremarkable.

4
دوخة Vertigo, dizziness versus ataxia= dysequilberium Definition of each and causes? Definition of each and causes? How we can differentiate between them? How we can differentiate between them? Concept map of approach ? Concept map of approach ? -type of symptoms and causes? -str. involved=localization -most likely cause -----investigation -Treatments : symptomatic and specific? -

5
دوخة Vertigo, dizziness versus ataxia= dysequilberium 1-Dizziness is non-specific broad term that includes vertigo, pre syncope (lightheadedness, impending fainting or giddiness,dimming of vision) instability and disequilibrium. Mechanisms? 1-Dizziness is non-specific broad term that includes vertigo, pre syncope (lightheadedness, impending fainting or giddiness,dimming of vision) instability and disequilibrium. Mechanisms? Vertigo: One of common problem we face in neurology and medicine. Vertigo: One of common problem we face in neurology and medicine. It is illusion of movement of the body or environment.it is often associated with sense of impulsion, visual illusion of movement (oscillopsia), nausea,vomiting,or ataxia. It is illusion of movement of the body or environment.it is often associated with sense of impulsion, visual illusion of movement (oscillopsia), nausea,vomiting,or ataxia. Vertigo must differentiated from non vertiginous dizziness mentioned above that result from impair brain ’ s supply of blood,oxygen, or glucose ex: vasovagal,orthostatic hypotension,cardiac ischemia and arrhythmias, hypoxia and hypoglycemia ; all may culminate into loss of consciousness and fall. If it is due to decresed cerebral hypo perfusion is called syncope. Vertigo must differentiated from non vertiginous dizziness mentioned above that result from impair brain ’ s supply of blood,oxygen, or glucose ex: vasovagal,orthostatic hypotension,cardiac ischemia and arrhythmias, hypoxia and hypoglycemia ; all may culminate into loss of consciousness and fall. If it is due to decresed cerebral hypo perfusion is called syncope. don ’ t forget hyperventilation where dizziness aggravated by 3 min. HV. don ’ t forget hyperventilation where dizziness aggravated by 3 min. HV.
 instability and disequilibrium. Mechanisms. Vertigo: One of common problem we face in neurology and medicine. Vertigo: One of common problem we face in neurology and medicine. It is illusion of movement of the body or environment.it is often associated with sense of impulsion, visual illusion of movement (oscillopsia), nausea,vomiting,or ataxia. It is illusion of movement of the body or environment.it is often associated with sense of impulsion, visual illusion of movement (oscillopsia), nausea,vomiting,or ataxia. Vertigo must differentiated from non vertiginous dizziness mentioned above that result from impair brain ’ s supply of blood,oxygen, or glucose ex: vasovagal,orthostatic hypotension,cardiac ischemia and arrhythmias, hypoxia and hypoglycemia ; all may culminate into loss of consciousness and fall. If it is due to decresed cerebral hypo perfusion is called syncope. Vertigo must differentiated from non vertiginous dizziness mentioned above that result from impair brain ’ s supply of blood,oxygen, or glucose ex: vasovagal,orthostatic hypotension,cardiac ischemia and arrhythmias, hypoxia and hypoglycemia ; all may culminate into loss of consciousness and fall. If it is due to decresed cerebral hypo perfusion is called syncope. don ’ t forget hyperventilation where dizziness aggravated by 3 min. HV. don ’ t forget hyperventilation where dizziness aggravated by 3 min. HV..")
6
2-Ataxia: is incoordination or clumsiness of movement that is not due to weakness. it is caused by vestibular,cerebellar, or sensory (proprioceptive) disorders. ataxia can affect eye movement limbs, trunk or gait 2-Ataxia: is incoordination or clumsiness of movement that is not due to weakness. it is caused by vestibular,cerebellar, or sensory (proprioceptive) disorders. ataxia can affect eye movement limbs, trunk or gait------------------------------------------------------------------------------- Draw concept map: When you diagnose vertigo as problem and depending on H., examination &investigation: When you diagnose vertigo as problem and depending on H., examination &investigation: 1st step is to differentiate between Central (due to lesion affecting brainstem VN or their connection) versus peripheral v (peripheral vest. lesion affecting labyrinth, inner ear or v. division of 8th cranial nerve). 1st step is to differentiate between Central (due to lesion affecting brainstem VN or their connection) versus peripheral v (peripheral vest. lesion affecting labyrinth, inner ear or v. division of 8th cranial nerve). central is more serious than peripheral central is more serious than peripheral Think about the etiology Think about the etiology Treatment. Treatment.
 disorders. ataxia can affect eye movement limbs, trunk or gait 2-Ataxia: is incoordination or clumsiness of movement that is not due to weakness. it is caused by vestibular,cerebellar, or sensory (proprioceptive) disorders. ataxia can affect eye movement limbs, trunk or gait Draw concept map: When you diagnose vertigo as problem and depending on H., examination &investigation: When you diagnose vertigo as problem and depending on H., examination &investigation: 1st step is to differentiate between Central (due to lesion affecting brainstem VN or their connection) versus peripheral v (peripheral vest. lesion affecting labyrinth, inner ear or v. division of 8th cranial nerve). 1st step is to differentiate between Central (due to lesion affecting brainstem VN or their connection) versus peripheral v (peripheral vest. lesion affecting labyrinth, inner ear or v. division of 8th cranial nerve). central is more serious than peripheral central is more serious than peripheral Think about the etiology Think about the etiology Treatment. Treatment..")
7
Peripheral central Peripheral central Vertigo: often intermittent :sever often constant usually less sever Vertigo: often intermittent :sever often constant usually less sever Nausea &vomiting : common uncommon Nausea &vomiting : common uncommon Nystagmus present: never vertical absent if present vertical Nystagmus present: never vertical absent if present vertical Unidirectional uni or bi-directional Unidirectional uni or bi-directional Hearing loss &tinnitus: often present rarely present Hearing loss &tinnitus: often present rarely present Intrinsic BS signs include : absent typically present Intrinsic BS signs include : absent typically present -M or S deficit -M or S deficit -dysartheria, ataxia -dysartheria, ataxia Visual fixation: Inhibited no effect Visual fixation: Inhibited no effect Head thrust sign positive negative etiology: etiology: BPV, V.neuronitis, labyrinthitis VB- ischemia,MS. cerebellar H.or infarction.or infarction

8
is in-coordination or clumsiness of movement that is not due to weakness. it is caused by vestibular,cerebellar, or sensory (proprioceptive) disorders. ataxia can affect eye movement limbs, trunk or gait. is in-coordination or clumsiness of movement that is not due to weakness. it is caused by vestibular,cerebellar, or sensory (proprioceptive) disorders. ataxia can affect eye movement limbs, trunk or gait. it result from same central or peripheral lesions that cause V. it result from same central or peripheral lesions that cause V. Sensory ataxia and motor Ataxias. Sensory ataxia and motor Ataxias. Vestibular ataxia: nystagmus is frequently present,usually unilateral most prominent on gaze away from side of lesion, dysartheria does not occur. It is gravity dependent : in coordination is not present in lying position. It is gravity dependent : in coordination is not present in lying position. Romberg ’ s signs is positive.? It is sensory ataxias. Romberg ’ s signs is positive.? It is sensory ataxias. Cerebellar ataxia: cerebellar disease itself or it ’ s connection. We have limb ataxia (hemisphere lesion) and truncal ataxia (vermis lesion) cerebellar disease itself or it ’ s connection. We have limb ataxia (hemisphere lesion) and truncal ataxia (vermis lesion) frontal lobe lesion may give picture mimic ataxia resulting from controlateral Cerebellar Hemisphere ?due to crossed connection between frontal lobe and cerebellar H. frontal lobe lesion may give picture mimic ataxia resulting from controlateral Cerebellar Hemisphere ?due to crossed connection between frontal lobe and cerebellar H.
 disorders. ataxia can affect eye movement limbs, trunk or gait. is in-coordination or clumsiness of movement that is not due to weakness. it is caused by vestibular,cerebellar, or sensory (proprioceptive) disorders. ataxia can affect eye movement limbs, trunk or gait. it result from same central or peripheral lesions that cause V. it result from same central or peripheral lesions that cause V. Sensory ataxia and motor Ataxias. Sensory ataxia and motor Ataxias. Vestibular ataxia: nystagmus is frequently present,usually unilateral most prominent on gaze away from side of lesion, dysartheria does not occur. It is gravity dependent : in coordination is not present in lying position. It is gravity dependent : in coordination is not present in lying position. Romberg ’ s signs is positive.. It is sensory ataxias. Romberg ’ s signs is positive.. It is sensory ataxias. Cerebellar ataxia: cerebellar disease itself or it ’ s connection. We have limb ataxia (hemisphere lesion) and truncal ataxia (vermis lesion) cerebellar disease itself or it ’ s connection. We have limb ataxia (hemisphere lesion) and truncal ataxia (vermis lesion) frontal lobe lesion may give picture mimic ataxia resulting from controlateral Cerebellar Hemisphere due to crossed connection between frontal lobe and cerebellar H. frontal lobe lesion may give picture mimic ataxia resulting from controlateral Cerebellar Hemisphere due to crossed connection between frontal lobe and cerebellar H..")
9
Cerebellar ataxia: it characterized by limb or truncal ataxia,dysartheria,nystagmus often present with or without other ocular abnormality like gaze paresis and defective saccadic and pursuit movement. vertigo may be present. it characterized by limb or truncal ataxia,dysartheria,nystagmus often present with or without other ocular abnormality like gaze paresis and defective saccadic and pursuit movement. vertigo may be present. The patient is unable to stand with feet together whether eyes is closed or not. The patient is unable to stand with feet together whether eyes is closed or not. C/F OF cerebellar disease? Specific and non specific. ? C/F OF cerebellar disease? Specific and non specific. ? Main causes : Main causes : *Acquired :infection,inflammatory, neoplastic and demyelinating ; vitamin E dependent A. *Acquired :infection,inflammatory, neoplastic and demyelinating ; vitamin E dependent A. *inherited : Olivopontocerebellar degeneration, Frederich's ataxia., spinocerebellar degeneration, metabolic like Wilson's disease. *inherited : Olivopontocerebellar degeneration, Frederich's ataxia., spinocerebellar degeneration, metabolic like Wilson's disease.

10
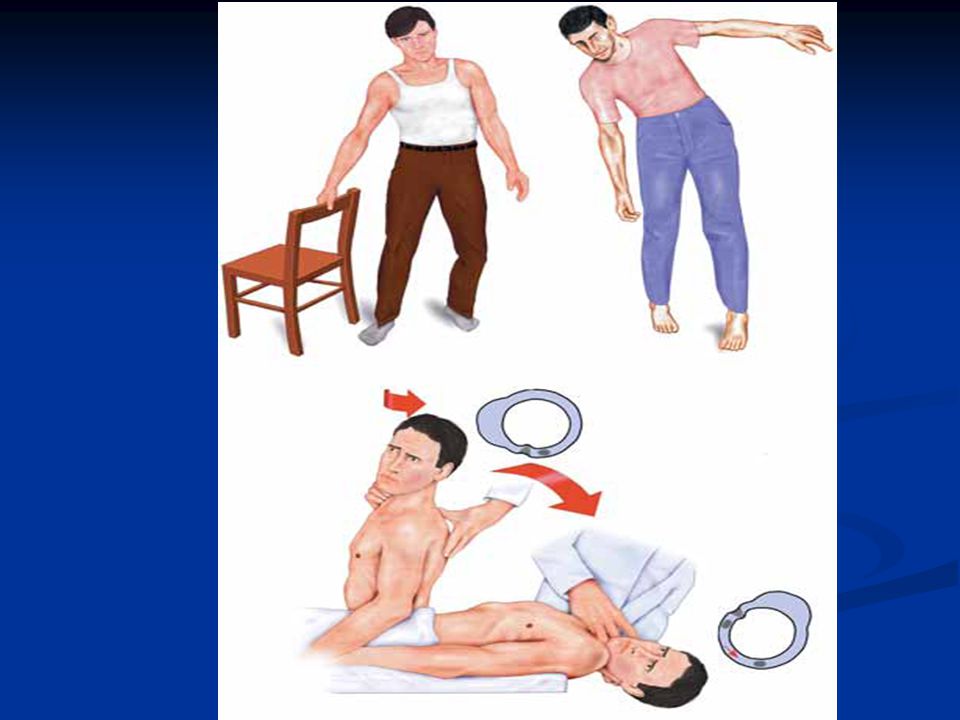
Sensory ataxia? result from disorder that affect the proprioceptive pathways in peripheral sensory nerve,sensory root, post. Column of spinal cord or m. lemniscuses. result from disorder that affect the proprioceptive pathways in peripheral sensory nerve,sensory root, post. Column of spinal cord or m. lemniscuses. Thalamic and parietal are rare causes of controlateral sensory hemi-ataxia. clinically the patient have: Thalamic and parietal are rare causes of controlateral sensory hemi-ataxia. clinically the patient have: impaired vibration and position sense, depressed ankle jerk impaired vibration and position sense, depressed ankle jerk able to stand with feet together when is opened not if it is closed (Romberg ’ s sign). able to stand with feet together when is opened not if it is closed (Romberg ’ s sign). Limb ataxia in legs may present Limb ataxia in legs may present Vertigo, dysartheria and nystagmus are absent. Vertigo, dysartheria and nystagmus are absent. Main causes: polyneuropathy, posterior SC lesion as in trepanomal disease, MS, Frederich's ataxia
. able to stand with feet together when is opened not if it is closed (Romberg ’ s sign). Limb ataxia in legs may present Limb ataxia in legs may present Vertigo, dysartheria and nystagmus are absent. Vertigo, dysartheria and nystagmus are absent. Main causes: polyneuropathy, posterior SC lesion as in trepanomal disease, MS, Frederich s ataxia.")
11
Approach? history : signs and symptoms vertigo or not, if ataxia which type? history : signs and symptoms vertigo or not, if ataxia which type? onset &time course onset &time course medical H medical H Family H Family H general physical examination general physical examination neurological examination including: neurological examination including: Mental state Mental state Gait &stance Gait &stance Cranial nerves checking i.e.: occulomotor,trochlear,abducent and acoustic nerves. Cranial nerves checking i.e.: occulomotor,trochlear,abducent and acoustic nerves. Check for PD which suggest increase ICP, or optic atrophy in case of MS,neurosyphilis,B12 deficiency Check for PD which suggest increase ICP, or optic atrophy in case of MS,neurosyphilis,B12 deficiency Facial nerve affection,corneal reflex associated with C-P angle mass Facial nerve affection,corneal reflex associated with C-P angle mass

12
Treatments

Similar presentations
 (MND) are a group of neurological disorders that selectively affect motor neurons.>")



>")






 Is it a stroke? (2) What part of the brain is affected? (3) What caused this stroke? Is it a haemorrhage or an infarct? Can.>")







