Download presentation
Presentation is loading. Please wait.

1
Hypokalaemia By Dr Nihal Abosaif Consultant acute physician UHCW

2
Outline Physiology of K+ transport Factors modifying transcellular K+ distribution Causes of Hypokalaemia Diseases associated with it Management of Hypokalaemia

3
Most abundant cation in human body Regulates intracellular enzyme function and helps to determine neuromuscular & cardiovascular tissue excitability. 90 % of total body K+ : Intracellular ( predominantly in muscle ) 10 % : Extracellular fluid < 1 % : Plasma Introduction : Potassium
 10 % : Extracellular fluid < 1 % : Plasma Introduction : Potassium.")
4
Ratio of extracellular K+ to Intracellular K+ : determines the membrane potential The acuity of changes in serum potassium concentration & membrane potential determines clinical symptoms and underlying signs Plasma concentration varies from 3.5 to 5.3 mmol/l Introduction : Potassium

5
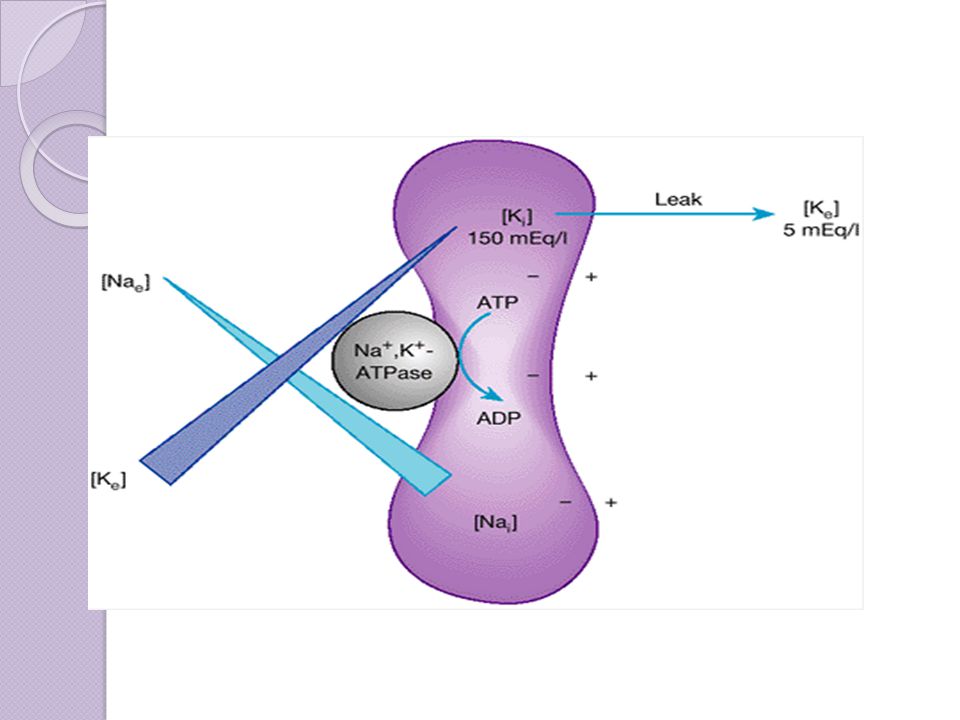
K+ uptake into cells : actively driven by Na+/K+/ATPase Leak back into ECF : opposed by electrical gradient Physiology Of Potassium Homeostasis

7
Acid base status Pancreatic hormones : insulin, glucagon Catecholamines Aldosterone Plasma Osmolality Exercise Cellular K+ content Factors modifying transcellular K+ distribution

8
Alkalosis promotes K+ uptake by cells Acidosis diminishes K+ uptake by cells Acute respiratory alkalosis, in contrast increase plasma K+ by 0.2 mmol/l per 0.1 pH unit due to increased adrenergic activity Acid Base Status

9
Insulin stimulates cellular uptake of K+ by activating Na+/K+/ATPase ( decreasing plasma K+ ) Insulin affects K+ transport independently of glucose uptake Glucagon increase plasma K+ independently of changes in plasma glucose / insulin Pancreatic Hormones
 Insulin affects K+ transport independently of glucose uptake Glucagon increase plasma K+ independently of changes in plasma glucose / insulin Pancreatic Hormones")
10
Beta 2 adrenergic activity – hypokalaemia Alpha adrenergic antagonists – hypokalaemia Catecholamines

11
Invitro studies Aldosterone stimulates Na+/K+/ATPase and thereby activating Na + influx Aldosterone

12
Hyperosmolality ( Mannitol infusion / hyperglycemia in DM ) : increase plasma K+ Each 10 mOsm / Kg rise in plasma osmolality, increases plasma K+ by 0.6 mmol/l Osmolality
 : increase plasma K+ Each 10 mOsm / Kg rise in plasma osmolality, increases plasma K+ by 0.6 mmol/l Osmolality")
13
Recurrent contraction increases K+ egress from muscle Modest exercise : high K+ in ECF in local environment produces vasodilatation & thereby increased regional blood flow Severe exercise : increase plasma K+ modestly Physical training increases Na+/K+/ATPase activity in skeletal muscle which helps skeletal muscle to take up K+ again Exercise

14
Kidney is dominant in sustaining K+ balance >90 % K+ : excreted in urine Remainder through faeces Decrease in GFR, K+ excretion via faeces increased GI Loss : K+ secretion by proximal & distal colon K+ Balance

15
Renal Handling of K+ Glomerulus: freely filtered PCT, TAL, Loop of Henle : reabsorbed

16
Defined as plasma concentration of K+ < 3.5 mEq/L Mild Hypokalemia : 3.0 – 3.5 mEq/L : asymptomatic Hypokalemia < 3.0 mEq/L : symptomatic Clinical manifestations of hypokalemia vary greatly between individual patients & their severity depends on degree of hypokalemia Hypokalemia

17
Clinical features Investigations Diagnosis

18
Mild hypokalemia : generally asymptomatic Increased risk of mortality for pts with cardiovascular disease – trigger ventricular tachycardia / ventricular fibrillation (decrease K+ : d/t sympathetic stimulation) Digitalis induced arrhythmias – can occur with normal drug levels if hypokalemia is present Diuretic induced hypokalemia & hypomagnesemia must be avoided in pts on drugs that prolong QT interval : as it predisposes to polymorphic VT / Torsade de pointes Hypokalemia < 3 mEq/L : Symptomatic Clinical Features
 Digitalis induced arrhythmias – can occur with normal drug levels if hypokalemia is present Diuretic induced hypokalemia & hypomagnesemia must be avoided in pts on drugs that prolong QT interval : as it predisposes to polymorphic VT / Torsade de pointes Hypokalemia < 3 mEq/L : Symptomatic Clinical Features")
19
Digitalis Intoxication : ventricular extrasystoles ventricular tachycardia ventricular fibrillation partial-complete AV block bradycardia atrial flutter atrial fibrillation Ventricular arrhythmias : tachycardia / fibrillation Cardiac

20
Fatigue Myalgia Muscular weakness involving lower limbs Severe Hypokalemia : Paralysis ( extremities ) Weakness of respiratory muscles ( dyspnea ) Rhabdomyolysis (exercise induced) Neuro-muscular
 Weakness of respiratory muscles ( dyspnea ) Rhabdomyolysis (exercise induced) Neuro-muscular")
21
Constipation Paralytic ileus Gastro-intestinal

22
Chronic interstitial nephritis due to functional decrease in renal blood flow – decreased GFR Chronic renal failure Renal Cysts Renal

23
Polyuria ( nephrogenic diabetes insipidus ) Polydipsia ( nephrogenic diabetes insipidus ) Increased ammonia production ( intracellular acidosis ) precipitate hepatic coma in pts with advanced liver ds Edema Chloride wasting Metabolic alkalosis Hypercalciuria Phosphaturia Fluid – Electrolyte
 Polydipsia ( nephrogenic diabetes insipidus ) Increased ammonia production ( intracellular acidosis ) precipitate hepatic coma in pts with advanced liver ds Edema Chloride wasting Metabolic alkalosis Hypercalciuria Phosphaturia Fluid – Electrolyte")
24
Glucose intolerance ( decreased insulin secretion ) Growth retardation ( Reduced Growth hormone receptors, Reduced IGF-1 ) Hypertension ( increased renin secretion ) Endocrine
 Growth retardation ( Reduced Growth hormone receptors, Reduced IGF-1 ) Hypertension ( increased renin secretion ) Endocrine")
25
ECG : Initially : flattening of t wave depression of ST Segment development of prominent u waves Severe hypokalemia : increased amplitude of p wave increased QRS duration S.Potassium Basic Investigations

26
Investigations – Causes Urinary K+ TTKG Urinary Chloride CBC Peripheral Smear ABG Echocardiogram Cardiac Enzymes Serum aldosterone Serum renin USG Abdomen CT / MRI Abdomen FBS / PPBS / Urine Ketones TSH / free T3 / free T4 Colonoscopy / OGDscopy

27
Decreased net intake Shift into cells Increased net loss Causes of hypokalaemia

29
Decreased total body K+ Decreased intake Renal loss of K+ Extra renal loss of K+

30
Occurs in patients with extreme leukocytosis eg : in myeloproliferative disorders Invitro WBC uptake potassium within the test tube Spurious Hypokalemia

31
Starvation Clay ingestion ( binds to dietary K+ & Iron ) Diarrhoea and vomiting Decreased Intake or increased loss
 Diarrhoea and vomiting Decreased Intake or increased loss")
32
Acid – Base Status : Metabolic Alkalosis Hormonal : Increased Insulin Increased Beta 2 Adrenergic activity Drugs : Beta 2 agonists Theophylline Barium Intoxication Chloroquine Calcium Channel Blockers Transcellular shifts

33
Catecholamine release associated with : Asthma COPD – exacerbations Heart failure Myocardial infarction / angina Drug withdrawal syndrome – alcohol / narcotics / barbiturates Transcellular shift

34
Insulin administration – for treatment of DKA Refeeding Syndrome Hypokalemic Periodic Paralysis Thyrotoxic Periodic Paralysis Treatment of anemia : Vit B12 / Folic acid deficiency Use of GM – CSF in patients with Neutropenia Transcellular shift

35
Urinary K+: > 20 mEq/L – Renal loss Urinary K + : < 20 mEq/L – Extrarenal loss TTKG : Transtubular Potassium Gradient ( Urine K+ / Plasma K+ ) ( Urine Osm / Plasma Osm ) TTKG : Renal loss : > 4 Extra renal loss : < 4 Renal Vs Extra renal loss
 ( Urine Osm / Plasma Osm ) TTKG : Renal loss : > 4 Extra renal loss : < 4 Renal Vs Extra renal loss")
36
Algorithm for diagnosis of Extra Renal Loss Urinary K+ < 20 mEq/L Metabolic Acidosis GI Loss Diarrhoea Laxative Abuse Normal pH Villous Adenoma Laxative Abuse Metabolic Alkalosis GI Loss: rare Laxative abuse : rare

37
Urinary loss K+ > 20 mEq/L Metabolic Acidosis RTA DKA Ureterosigmoido stomy Variable pH ATN recovery Post obstructive diuresis Drugs Metabolic Alkalosis Urinary chloride level Renal Loss

38
Urinary Chloride < 20 mmol/L Diuretics Vomiting > 20 mmol/L Check BP Renal Loss + Metabolic Alkalosis

39
Check BP, ECFLow BPCheck Bicarb Low - RTAHigh : Bartter, Gitelman HTN, Increased ECF Check Renin, Aldosterone Renal loss +Urine Cl > 20 mEq/L

40
Amphotericin B : tubular damage increased excretion of K+ Aminoglycosides : renal wasting of K+ Thiazides, Furosemide, Acetazolamide : renal loss K+ Cisplatin HYPOMAGNESEMIA : Significant renal K+ wasting Renal loss - Drugs

41
Management of Hypokalaemia If mild asymptomatic Oral KCl If severe or symptomatic hypokalemia IV KCl supplement

42
IV infusion rate for severe or symptomatic hypokalemia. Standard IV replacement rate 10 - 20 mmol/h Serum potassium < 2.5 meq/L, or Moderate-severe symptoms 20 - 40 mmol/h Serum potassium < 2.0 Meq/L, or Life-threatening symptoms > 40 mmol/h If heart block, or Renal insufficiency exists 5 - 10 mmol/h

43
THANK YOU

Similar presentations













 Major determinant of resting membrane potential. (arrhythmia’s etc) Long term =>")

 Potassium Disorders 1.Normal potassium metabolism: (1) Balance of potassium intake and excretion: K + intake : 50-200mmol/day from vegetable.>")

What are the adverse medical implications of this condition.>")


