Download presentation
Presentation is loading. Please wait.

1
JOURNAL REVIEW RADIAL VS FEMORAL ACCESS IN PRIMARY PCI CULPRIT VS MULTIVESSEL PCI IN PRIMARY PCI PRIMARY PCI IN CARDIOGENIC SHOCK Dr Sandeep.R SR CARDIO

2
RADIAL VS FEMORAL ACCESS IN PRIMARY PCI Eikelboom JW et al. Circulation 2006;114(8):774-82
:774-82")
4
HOU ET AL AUG2005 – SEP 2008 INCLUSION : AMI <12hrs EXCLUSION: CS,H/O CABG,ALLEN’S TEST –ve NON PALPABLE RADIAL A. N=200,( TRA =100,TFA=100) PRIMARY OUTCOME: 30 DAY MACE,VASCULAR COMPLCN. HOSPITAL STAY SECONDARY OUTCOME : INTRAPROCEDURE CHARACTERISTICS
 PRIMARY OUTCOME: 30 DAY MACE,VASCULAR COMPLCN. HOSPITAL STAY SECONDARY OUTCOME : INTRAPROCEDURE CHARACTERISTICS.")
5
APRIL 2011 OBJECTIVE To determine if Radial vs. Femoral access for coronary angiography/PCI can reduce the composite of death, MI, stroke or non-CABG major bleeding in ACS patients METHODOLOGY Done in 32 countries n=7021( june 2006 – nov 2010) Primary outcome: Death, Mi, stroke or non CABG bleeding within 30 days Secondary outcomes Death, M. i or stroke, non-CABG-related major bleeding at 30 days, major vascular access site complications at 48 h & 30 days PCI procedural success.
 Primary outcome: Death, Mi, stroke or non CABG bleeding within 30 days Secondary outcomes Death, M. i or stroke, non-CABG-related major bleeding at 30 days, major vascular access site complications at 48 h & 30 days PCI procedural success..")
6
NSTE-ACS and STEMI (n=7021) Radial Access (n=3507) Femoral Access (n=3514) Primary Outcome: Death, MI, stroke or non-CABG-related Major Bleeding at 30 days Randomization RIVAL Study Design Key Inclusion: Intact dual circulation of hand required Interventionalist experienced with both (minimum 50 radial procedures in last year) Jolly SS et al. Am Heart J. 2011;161:254-60. Blinded Adjudication of Outcomes EXCL. 1)CARDIOGENIC SHOCK 2)SEVERE POVD 3)PRIOR CABG WITH >1 LIMA
CARDIOGENIC SHOCK 2)SEVERE POVD 3)PRIOR CABG WITH >1 LIMA.")
7
Primary and Secondary Outcomes Radial (n=3507) % Femoral (n=3514) % HR 95% CI P Primary Outcome Death, MI, Stroke, Non-CABG Major Bleed 3.74.00.920.72-1.170.50 Secondary Outcomes Death, MI, Stroke 3.2 0.980.77-1.280.90 Non-CABG Major Bleeding 0.70.90.730.43-1.230.23
 % Femoral (n=3514) % HR 95% CI P Primary Outcome Death, MI, Stroke, Non-CABG Major Bleed Secondary Outcomes Death, MI, Stroke Non-CABG Major Bleeding")
8
Other Outcomes Radial (n=3507) % Femoral (n=3514) % HR 95% CI P Major Vascular Access Site Complications 1.43.70.370.27-0.52 <0.0001 Other Definitions of Major Bleeding TIMI Non-CABG Major Bleeding 0.5 1.000.53-1.89 1.00 ACUITY Non-CABG Major Bleeding* 1.94.50.430.32-0.57 <0.0001 * Post Hoc analysis
 % Femoral (n=3514) % HR 95% CI P Major Vascular Access Site Complications < Other Definitions of Major Bleeding TIMI Non-CABG Major Bleeding ACUITY Non-CABG Major Bleeding* < * Post Hoc analysis")
9
Other Outcomes Radial (n=3507) % Femoral (n=3514) % HR 95% CI P Death 1.31.50.860.58-1.290.47 MI 1.71.90.920.65-1.31 0.65 Stroke 0.60.41.430.72-2.83 0.30 Stent Thrombosis 0.71.20.630.34-1.17 0.14
 % Femoral (n=3514) % HR 95% CI P Death MI Stroke Stent Thrombosis")
10
Death, MI, Stroke or non-CABG major Bleed Subgroups: Primary Outcome Subgroups: Primary Outcome

11
RESULTS

12
Results stratified by High*, Medium* and Low* Volume Radial Centres Results stratified by High*, Medium* and Low* Volume Radial Centres High (>146 radial PCI/year/ median operator at centre), Medium (61-146), Low (≤60)
, Medium (61-146), Low (≤60)")
13
NSTE/ACS STEMI NSTE/ACS STEMI NSTE/ACS STEMI NSTE/ACS STEMI NSTE/ACS STEMI 5063 1958 5063 1958 5063 1958 5063 1958 5063 1958 3.5 5.2 2.7 4.6 0.8 3.2 1.0 0.9 3.8 3.5 3.8 3.1 3.4 2.7 1.2 1.3 0.6 0.8 1.4 1.3 0.251.004.00 Radial better Femoral better Hazard Ratio(95% CI) 0.025 0.011 0.001 0.56 0.89 Interaction p-value 2NRadial Femoral % Primary Outcome Death, MI or stroke Death Non CABG Major Bleed Major Vascular Complications Outcomes stratified by STEMI vs. NSTEACS R I V A L

14
Conclusion No significant difference between radial and femoral access in primary outcome of death, MI, stroke or non-CABG major bleeding Rates of primary outcome appeared to be lower with radial compared to femoral access in high volume radial centres & STEMI Radial had fewer major vascular complications with similar PCI success

15
OBJECTIVE: Compare the usefulness, effectiveness and procedural course of the TRA and TFA for PCI in pt. with STEMI &compare the effects during hospitalization Small single centre RCT (N=100) April 2005- june 2006 Inclusion criteria: 1)age 18-75 2) STEMI< 12hr
 April june 2006 Inclusion criteria: 1)age ) STEMI< 12hr.")
16
RESULTS CONCLUSION No diff. in outcomes between TRA &TFA TRA for PCI in patients with MI is equally effective as TFA. Total procedure time, X-ray exposure time &contrast vol. did not differ TRA in PCI procedures –early ambulation Complications are rare in both groups.

17
` Aim: To compare the results of TRA and TFA using a StarClose device for primary PCI in patients with ST-elevation myocardial infarction (STEMI) Methods: Patients were randomised to PCI using TRA (n = 49) or PCI using TFA and StarClose (n = 59) - NOV 2006 – MAR 2008 Inclusion criteria were: (1) age 18–75 years, (2)STEMI <12 HR Exclusion criteria were: (1) Killip class III or IV (2) Necessity to use an IABP or TPI (3) patient’s height < 150 cm, (4) history of coronary artery bypass grafting (CABG) Kardiologia Polska 2011; 69, 8: 763–771
 Methods: Patients were randomised to PCI using TRA (n = 49) or PCI using TFA and StarClose (n = 59) - NOV 2006 – MAR 2008 Inclusion criteria were: (1) age 18–75 years, (2)STEMI <12 HR Exclusion criteria were: (1) Killip class III or IV (2) Necessity to use an IABP or TPI (3) patient’s height < 150 cm, (4) history of coronary artery bypass grafting (CABG) Kardiologia Polska 2011; 69, 8: 763–771")
18
RESULTS Kardiologia Polska2011; 69, 8: 763–771

19
CONCLUSIONS 1.Performing PCI in patients with MI -Longer D to B time in TRA vs TFA.(No impact on MACE) 2. The duration and efficacy of PCI were comparable in both groups 3. VCD after PCI in the TFA group resulted in a similar incidence of access site and bleeding complications rates as in the TRA 4. The use of vascular closure devices allows early ambulation in TFA Results: D to B inflation time was 67.4 ± 17.1 vs 57.5 ± 17.5 min (p = 0.009) (tra vs tfa) There were no significant differences in the incidence of MACE or bleeding complications between the groups: 2.1% and 8.2% in the TRA group vs 1.7% and 10.2% in the TFA group Ambulation time comparable Kardiologia Polska 2011; 69, 8: 763–771
 (tra vs tfa) There were no significant differences in the incidence of MACE or bleeding complications between the groups: 2.1% and 8.2% in the TRA group vs 1.7% and 10.2% in the TFA group Ambulation time comparable Kardiologia Polska 2011; 69, 8: 763–771.")
20
Heart 2007;93:1556–1561. Objective: To compare bleeding complications and results of percutaneous coronary intervention (PCI) between patients treated by radial and femoral approaches for acute myocardial infarction (AMI,) and using abciximab and 5 French guiding-catheters Patients: 114 consecutive patients with AMI were prospectively randomised. Exclusion criteria H/O CABG, cardiogenic shock, AV block, and c/I to abciximab or negative Allen test,need for IABP /TPI
 between patients treated by radial and femoral approaches for acute myocardial infarction (AMI,) and using abciximab and 5 French guiding-catheters Patients: 114 consecutive patients with AMI were prospectively randomised. Exclusion criteria H/O CABG, cardiogenic shock, AV block, and c/I to abciximab or negative Allen test,need for IABP /TPI.")
21
Heart 2007;93:1556–1561.

22
Results: No diff in primary outcomes Peripheral arterial complication rates & delays to patient ambulation significantly lower in RA vs FA A cross over necessary in the RA than in FA CAG & FLUORO time were significantly longer in the RA VS FA but PCI duration similar in both groups.

23
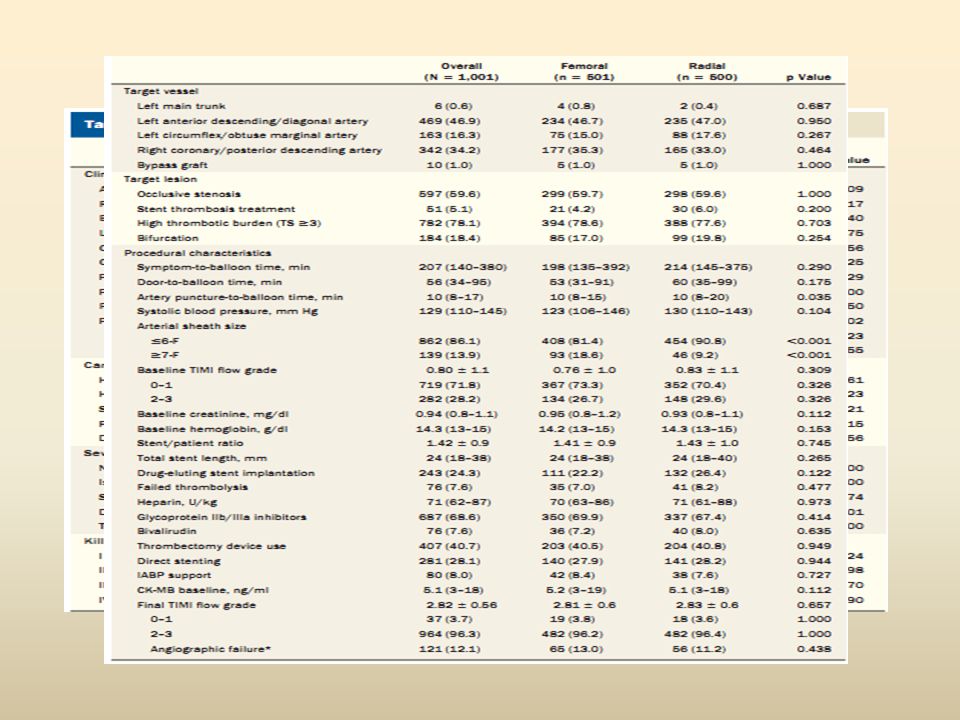
Objectives : The purpose of this study was to assess whether transradial access for STEMI ACS undergoing early invasive treatment is associated with better outcome compared with conventional transfemoral access. METHODOLOGY: Multicenter, randomized, parallel-group study (January 2009 and July 2011) n= 1,001 acute STEMI ACS pts< 24 hrs undergoing primary/rescue PCI were randomized to the radial (500) or femoral (501) approach at 4 high-volume centers The primary endpoint- 30-day rate of net adverse clinical events (NACEs), defined as a composite of cardiac death,stroke, MI, TLR, and bleeding Individual components of NACEs & length of hospital stay -secondary endpoints.
 n= 1,001 acute STEMI ACS pts< 24 hrs undergoing primary/rescue PCI were randomized to the radial (500) or femoral (501) approach at 4 high-volume centers The primary endpoint- 30-day rate of net adverse clinical events (NACEs), defined as a composite of cardiac death,stroke, MI, TLR, and bleeding Individual components of NACEs & length of hospital stay -secondary endpoints..")
24
STUDY DESIGN

26
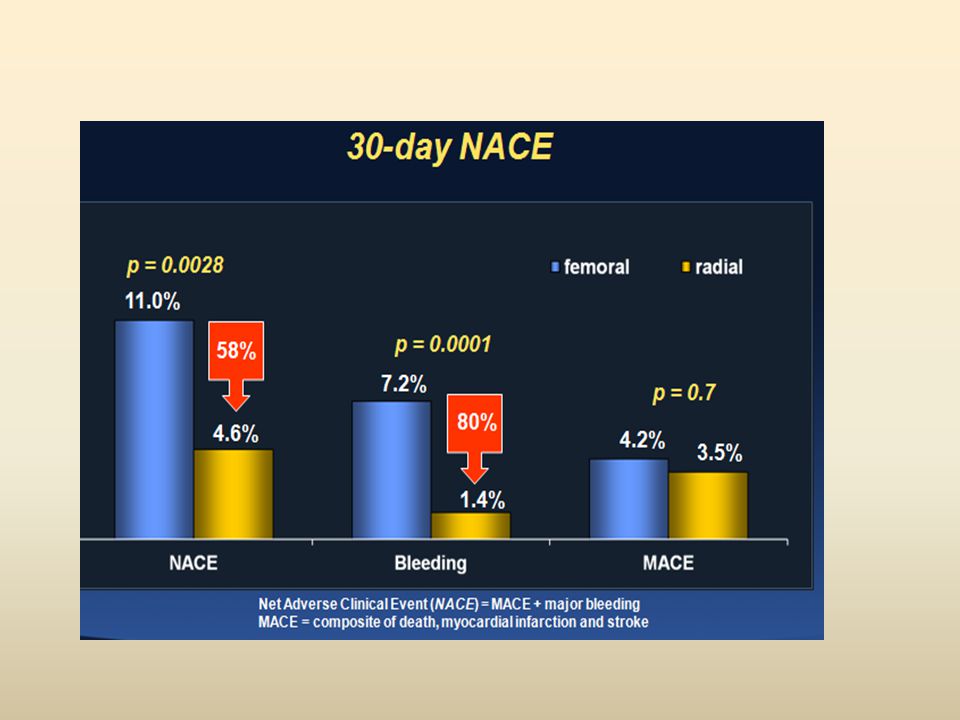
RESULTS

27
CONCLUSION Radial access in patients with STEMI is associated with significant clinical benefit, in terms of both bleeding and cardiac mortality. Radial approach is not just a valid alternative but it should become recommended approach in these pt.

28
To compare radial vs femoral approach in primary PCI for patients with STEMI 80% radial primary PCI) OBJECTIVES
 OBJECTIVES")
30
CONCLUSION In patients with STEMI <12 hrs, radial approach was associated with a significant lower incidence of major bleeding and access site complications and a significant better net clinical benefit. Moreover radial approach reduced significantly ICU stay and contrast volume compared to femoral approach. Our results support the use of radial approach in primary PCI in high volume centers as a first choice

31
META ANALYSIS Am J Cardiol 2012;109:813–818

32
WHAT DOES THE GUIDELINE SAY? ESC GUIDELINES 2013 AHA – NO GUIDELINES Conclusions: In STEMI patients undergoing primary PCI, the radial approach is associated with favorable outcomes and should be the preferred approach for experienced radial operators.

33
CULPRIT VS MULTIPCI INPPCI

34
POLITI et al AIM: To compare long-term outcomes of three different strategies during primary PCI in patients with STEMI and MVD; culprit vessel-only angioplasty; angioplasty of IRA followed by an elective procedure for the treatment of other lesions & simultaneous treatment of IRA & non-IRA METHODOLOGY:n=263 Study period Jan 2003 –Dec 2007, follow up of 2.5 yr Inclusion crit. : AMI < 12 hr Exclusion crit. : Cardiogenic shock, left main coronary disease (>50% diameter stenosis), previous CABG, severe valvular heart disease & failed procedures
, previous CABG, severe valvular heart disease & failed procedures.")
35
After every diagnostic angiography, the eligible patients were randomly allocated to 3 different strategies: 1. Culprit-only revascularisation (COR): the IRA only was dilated and the other arteries were left untreated. 2. Staged revascularisation (SR): the IRA only was treated during the primary intervention while the complete revascularisation was planned in a second procedure. 3. Complete revascularisation (CR): the IRA was opened followed by dilatation of other significantly narrowed arteries during the same procedure.
: the IRA only was dilated and the other arteries were left untreated. 2. Staged revascularisation (SR): the IRA only was treated during the primary intervention while the complete revascularisation was planned in a second procedure. 3. Complete revascularisation (CR): the IRA was opened followed by dilatation of other significantly narrowed arteries during the same procedure..")
36
STUDY PROTOCOL STEMI & MVD (n=243) Excluded 21 CS,6 LM dis.,9 previous CABG,7 VHD,4 failed N=214 COR N=84 SR N=65 CR N=65 The primary endpoint of the study was the incidence of MACE defined as cardiac or non-cardiac death, inhospital death, re-infarction, re-hospitalisation for ACS and repeat coronary revascularisation. FOLLOW UP PERIOD 2.5 YRS

37
RESULTS

38
Results: During a mean follow-up of 2.5 years, 42 (50.0%) patients in the COR group experienced at least one MACE, 13 (20.0%) in SR group & 15 (23.1%) in the CR group, p<0.001. Inhospital death, repeat revascularisation and rehospitalisation occurred more frequently in the COR group (all p<0.05), whereas there was no significant difference in re-infarction among the three groups. Survival free of MACE was significantly reduced in the COR group but was similar in the CR and SR groups CONCLUSION: COR associated with the highest rate of long-term MACE compared with multivessel treatment. Patients scheduled for staged revascularisation experienced a similar rate of MACE to patients undergoing complete simultaneous treatment of non-IRA.
, whereas there was no significant difference in re-infarction among the three groups. Survival free of MACE was significantly reduced in the COR group but was similar in the CR and SR groups CONCLUSION: COR associated with the highest rate of long-term MACE compared with multivessel treatment. Patients scheduled for staged revascularisation experienced a similar rate of MACE to patients undergoing complete simultaneous treatment of non-IRA..")
39
JACC Vol. 58, No. 7, 2011 AIM: To compare a one-time primary PCI of the culprit and nonculprit lesions with PCI of only the culprit lesion and staged nonculprit PCI at a later date in patients with STEMI and MVD METHODOLOGY:HORIZONS-AMI study was a prospective, open-label, randomized, multicenter trial in which 3,602 patients with STEMI <12hrs INCLUSION CRIT. STEMI< 12HRS EXCLUSION CRIT: 1)prior administration of fibrinolytic therapy, bivalirudin, GPI, LMWH, or fondaparinux 2)current use of warfarin 3) history of bleeding diathesis, conditions predisposing to hemorrhagic risk, or refusal to receive blood transfusions 4) Stroke or TIA < 6 months or any permanent neurologic deficit 5) Recent or known platelet count <100,000 cells/mm3 or Hb< 10 g/dl
prior administration of fibrinolytic therapy, bivalirudin, GPI, LMWH, or fondaparinux 2)current use of warfarin 3) history of bleeding diathesis, conditions predisposing to hemorrhagic risk, or refusal to receive blood transfusions 4) Stroke or TIA < 6 months or any permanent neurologic deficit 5) Recent or known platelet count <100,000 cells/mm3 or Hb< 10 g/dl.")
40
JACC Vol. 58, No. 7, 2011 The study endpoints :1-year MACE and its components-death, reinfarction, ischemia- driven TVR & stroke

41
RESULTS JACC Vol. 58, No. 7, 2011

42
RESULTS: Single versus staged PCI was associated with higher 1-year mortality (9.2% vs. 2.3%; hazard ratio [HR]: 4.1, 95% confidence interval [CI]: 1.93 to 8.86, p < 0.0001), cardiac mortality (6.2% vs. 2.0%; HR: 3.14, 95% CI: 1.35 to 7.27, p =0.005), definite/probable stent thrombosis (5.7% vs. 2.3%; HR: 2.49, 95% CI: 1.09 to 5.70, p = 0.02), and a trend toward greater MACE (18.1% vs. 13.4%; HR: 1.42, 95% CI: 0.96 to 2.1, p = 0.08) The mortality advantage favoring staged PCI was maintained in a subgroup of patients undergoing truly elective multivessel PCI. Staged PCI strategy was independently associated with lower all-cause mortality at 30 days and at 1 year. CONCLUSION:A deferred angioplasty strategy of nonculprit lesions should remain the standard approach in patients with STEMI undergoing primary PCI, as multivessel PCI may be associated with a greater hazard for mortality and stent thrombosis.
, cardiac mortality (6.2% vs. 2.0%; HR: 3.14, 95% CI: 1.35 to 7.27, p =0.005), definite/probable stent thrombosis (5.7% vs. 2.3%; HR: 2.49, 95% CI: 1.09 to 5.70, p = 0.02), and a trend toward greater MACE (18.1% vs. 13.4%; HR: 1.42, 95% CI: 0.96 to 2.1, p = 0.08) The mortality advantage favoring staged PCI was maintained in a subgroup of patients undergoing truly elective multivessel PCI. Staged PCI strategy was independently associated with lower all-cause mortality at 30 days and at 1 year. CONCLUSION:A deferred angioplasty strategy of nonculprit lesions should remain the standard approach in patients with STEMI undergoing primary PCI, as multivessel PCI may be associated with a greater hazard for mortality and stent thrombosis..")
43
APEX AMI TRIAL European Heart Journal (2010) 31, 1701–1707 TYPE NINCLUSION CRITERIA EXCLUSION CRITERIA OUTCOMERESULTS APEX AMI SUBGP. STUDY2201 (2004- 2006) STEMI with high risk ecg<6hr 1)Rescue PCI 2)isolated IW MI 90-day mortality 90-day composite of death, CHF& CS 12.5 (NIRA)vs. 5.6%(IRA), P < 0.001 17.4(NIRA) vs. 12.0%(IRA), P = 0.020 [adjusted hazard ratio 2.44, 95% CI (1.55–3.83), P < 0.001]
 STEMI with high risk ecg<6hr 1)Rescue PCI 2)isolated IW MI 90-day mortality 90-day composite of death, CHF& CS 12.5 (NIRA)vs. 5.6%(IRA), P < (NIRA) vs. 12.0%(IRA), P = [adjusted hazard ratio 2.44, 95% CI (1.55–3.83), P < 0.001].")
44
EuroIntervention 2012;8:456-464 STUDY TYPE NINCLUSION CRITERIA EXCLUSION CRITERIA END PT.RESULT JENSON ET AL Retrospective1174 (2002-09) STEMI<12hrcardiogenic shock, IABP All-cause Mortality
 STEMI<12hrcardiogenic shock, IABP All-cause Mortality")
49
AHA GUIDELINES 2013 ESC GUIDELINE 2012

51
PRIMARY PCI IN CARDIOGENIC SHOCK

52
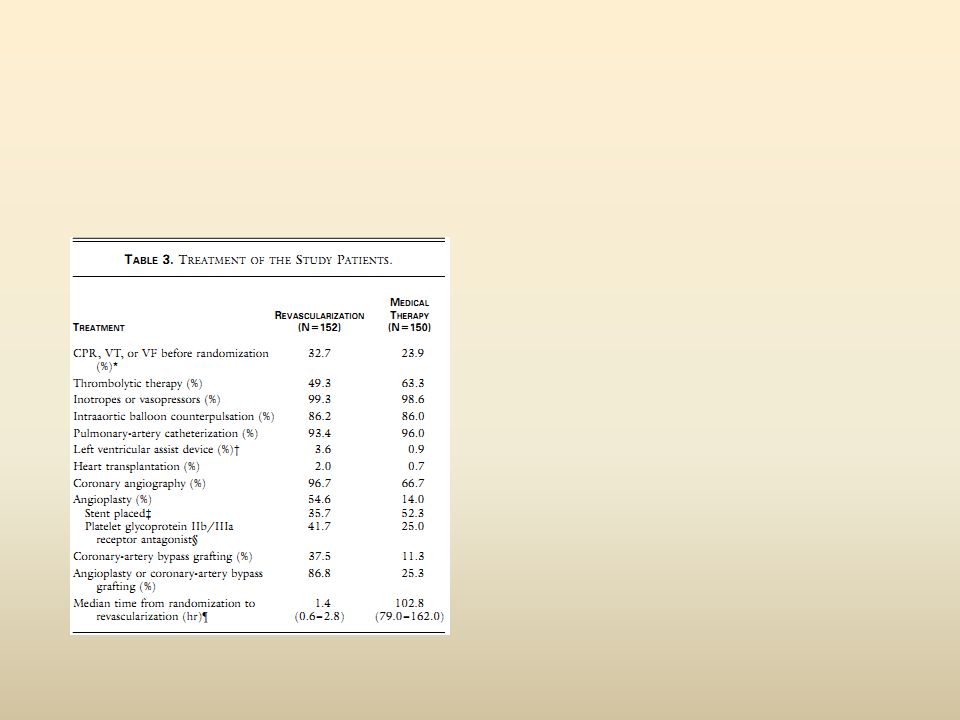
s OBJECTIVE : To compare the effects of early revascularization ( PCI & CABG) on 30 day & 1yr survival in patients who present with cardiogenic shock after AMI vs initial medical stabilizn 30 centre ( APR 1993-NOV 1998) The primary end point - overall mortality 30 days after randomization. Secondary end point -overall mortality 6 & 12 months after infarction INCLUSION : AMI with shock < 36hr of MI EXCLUSION: Severe systemic illness Mechanical or other cause of shock, Severe valvular disease DCMPY Inability to gain access for catheterization & unsuitability for revascrln.

54
RESULTS

56
CONCLUSION: Overall mortality at 30 days did not differ significantly between the revascularization and medical-therapy groups (46.7 % and 56.0 %, respectively; difference, -9.3 %; 95 % confidence interval for the difference, -20.5 to 1.9 percent; P=0.11) Six-month mortality was lower in the revascularization group than in the medical- therapy group (50.3 percent vs. 63.1 percent, P=0.027) However, early revascularization resulted in lower mortality from all causes at six months Hence, early revascularization be strongly considered for patients with acute myocardial infarction complicated by cardiogenic shock.
 However, early revascularization resulted in lower mortality from all causes at six months Hence, early revascularization be strongly considered for patients with acute myocardial infarction complicated by cardiogenic shock..")
57
SUB GROUP ANALYSIS J Am Coll Cardiol 2003;42:1380–6

58
Percutaneous Coronary Intervention for Cardiogenic Shock in the SHOCK Trial JACC Vol. 42, No. 8, 2003 Conclusion. Successful early restoration of coronary blood flow is a major predictor of survival and an important therapeutic goal. Benefit of reperfusion appears to extend > accepted 12-h post-MI window. Surgery - in shock patients with severe MR or multivessel disease

59
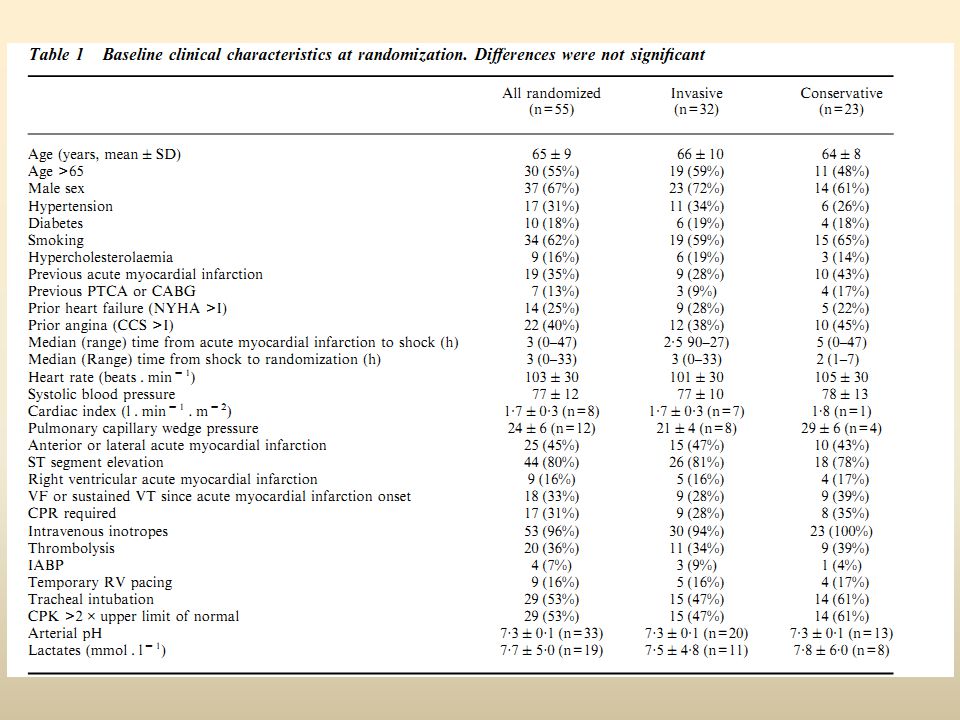
Aim : To compare a strategy of early intervention when appropriate vs initial medical management in shock pt. due to primary pump failure < 48hrs AMI METHODOLOGY: Multicentre ( nine centres) RCT,1992-1996,30 day &1 yr survival studied N= 55 patients ( 32 invasive & 23 medical).Of the 32 patients in the invasive group, 30 (94%) underwent early angiography, 27 (84%) PTCA, and one (4%) CABG. Primary end-point: the main study end-point was mortality from all causes (cardiac and non-cardiac) 30 days after randomization. Secondary end-points: (1) need for non-emergency PTCA and/or CABG during hospital stay (2) (CCS) angina and (NYHA) heart failure class at discharge from hospital; (3) Mortality, cardiac events and functional status at 1 year.
 RCT, ,30 day &1 yr survival studied N= 55 patients ( 32 invasive & 23 medical).Of the 32 patients in the invasive group, 30 (94%) underwent early angiography, 27 (84%) PTCA, and one (4%) CABG. Primary end-point: the main study end-point was mortality from all causes (cardiac and non-cardiac) 30 days after randomization. Secondary end-points: (1) need for non-emergency PTCA and/or CABG during hospital stay (2) (CCS) angina and (NYHA) heart failure class at discharge from hospital; (3) Mortality, cardiac events and functional status at 1 year..")
61
CONCLUSION : Failed to demonstrate that emergency PTCA significantly improves survival in patients with AMI & early cardiogenic shock. As the study was stopped prematurely, due to an insufficient patient inclusion rate, a clinically meaningful benefit of early reperfusion may have been missed

62
Objectives: To assess the impact of multivessel (MV) primary percutaneous coronary intervention (PCI) on clinical outcomes in patients with ST-segment elevation myocardial infarction (STEMI) presenting with cardiogenic shock (CS) and resuscitated cardiac arrest (CA) Background :The safety and efficacy of MV primary PCI in patients with STEMI and refractory CS is unknown METHODOLOGY : Multicentre observational study done in 5 french centres (1998 - 2010) INCLUSION CRIT. 1)Resuscitated from cardiac arrest, 2) Satisfied the criteria for STEMI and CS 3) Culprit lesion on CAG < 24 h after AMI EXCLUSION CRIT. 1)Futile on arrival at the cath lab 2)Alternative cause of shock was suspected 3)Mechanical complication of myocardial infarction (MI) determined before PCI
Resuscitated from cardiac arrest, 2) Satisfied the criteria for STEMI and CS 3) Culprit lesion on CAG < 24 h after AMI EXCLUSION CRIT. 1)Futile on arrival at the cath lab 2)Alternative cause of shock was suspected 3)Mechanical complication of myocardial infarction (MI) determined before PCI.")
63
The primary outcome measure of the study was 6-month survival Secondary endpoints included death due to CS, recurrent cardiac arrest, and a composite of these endpoints

65
Results. Patients with SVD (36.5% had increased 6-month survival compared to those with MVD (29.6% vs. 42.3%, p - 0.032). However, 6-month survival was significantly greater in patients who underwent MV PCI (43.9% vs. 20.4%, p -0.0017). This survival advantage was mediated by a reduction in the composite of recurrent CA and death due to shock (p - 0.024) in MV PCI patients Conclusions:The results of this study suggest that in STEMI patients with MVD presenting with CS and CA, MV primary PCI may improve clinical outcome.
. However, 6-month survival was significantly greater in patients who underwent MV PCI (43.9% vs. 20.4%, p ). This survival advantage was mediated by a reduction in the composite of recurrent CA and death due to shock (p ) in MV PCI patients Conclusions:The results of this study suggest that in STEMI patients with MVD presenting with CS and CA, MV primary PCI may improve clinical outcome..")
66
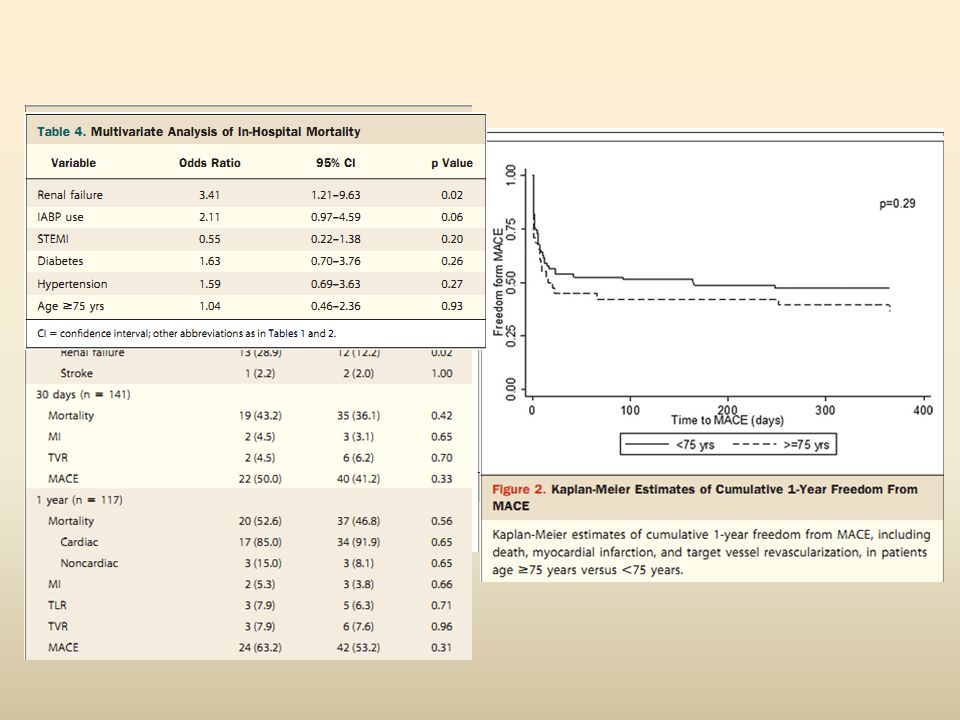
AIM:To evaluate the clinical characteristics, lesion features, procedural details, and clinical outcomes of elderly pts >75 years old compared with pts <75 years old undergoing PCI for acute MI complicated by CS in a large, contemporary multicenter PCI registry. BACKGROUND :Although benefits of early PCI have been shown in younger groups only few studies have reported on clinical outcomes in elderly shock patients using current PCI techniques METHODOLOGY: 145 pts ( n=45 >75yr & n=98 <75yr) ( AMI &CS) from the Melbourne Interventional Group registry between 2004 and 2007 were analyzed Primary outcome: 1)All cause mortality 2)Periprocedural Mi 3)Bleeding 4)CHF 5)Renal failure/Stroke 6)Emergent PCI or CABG SECONDARY OUTCOME 30day & 1 YR 1)All cause mortality 2)Cardiac & noncardiac death 3)TLR &TVR 4) MACE
 ( AMI &CS) from the Melbourne Interventional Group registry between 2004 and 2007 were analyzed Primary outcome: 1)All cause mortality 2)Periprocedural Mi 3)Bleeding 4)CHF 5)Renal failure/Stroke 6)Emergent PCI or CABG SECONDARY OUTCOME 30day & 1 YR 1)All cause mortality 2)Cardiac & noncardiac death 3)TLR &TVR 4) MACE.")
68
RESULTS CONCLUSION: 1-year survival of elderly patients with AMI complicated by CS undergoing PCI using contemporary techniques was comparable with survival rates of younger patients. Elderly patients presenting with CS may benefit from selective use of early revascularization and merits further investigation. Elderly patients were more likely to be female (46.7% vs. 22.4%, p = 0.01), Hypertensive(77.8% vs. 46.4%, p = 0.01), previous MI (31.1% vs. 15.5%, p =0.03), renal failure (24.4% vs. 11.3%, p = 0.05) and MVD (93.1% vs. 68.3%, p = 0.01) In-hospital, 30-day, and 1-year mortality in the elderly group versus the younger group were 42.2% vs. 33.7% (p = 0.32), 43.2% vs. 36.1% (p =0.42), and 52.6% vs. 46.8% (p=0.56), respectively.
, Hypertensive(77.8% vs. 46.4%, p = 0.01), previous MI (31.1% vs. 15.5%, p =0.03), renal failure (24.4% vs. 11.3%, p = 0.05) and MVD (93.1% vs. 68.3%, p = 0.01) In-hospital, 30-day, and 1-year mortality in the elderly group versus the younger group were 42.2% vs. 33.7% (p = 0.32), 43.2% vs. 36.1% (p =0.42), and 52.6% vs. 46.8% (p=0.56), respectively..")
69
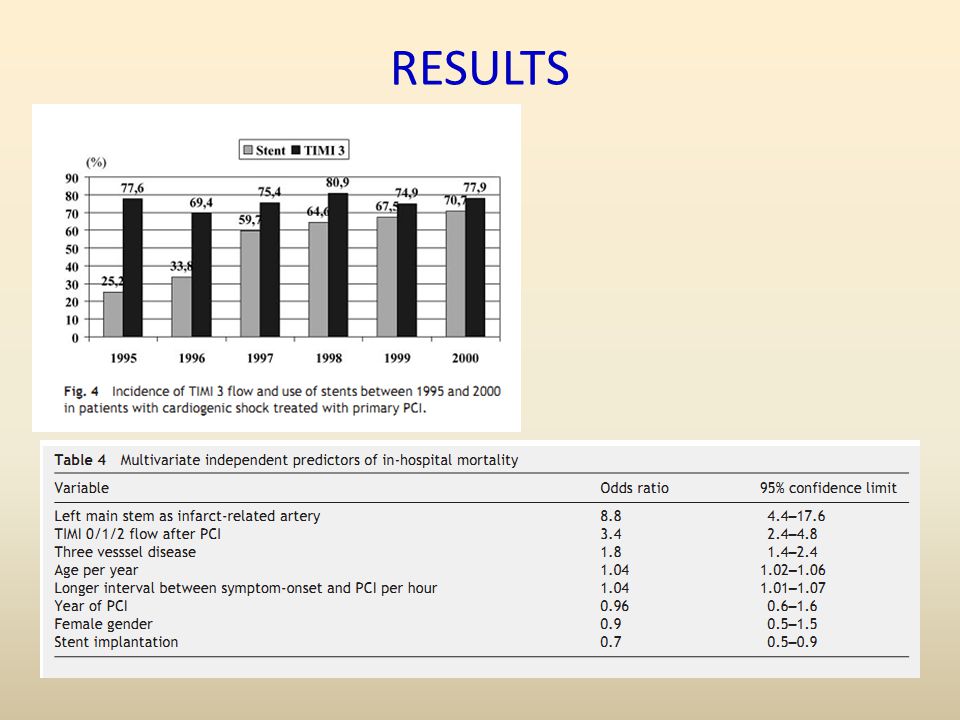
AIM:To evaluate predictors of in-hospital mortality of a large cohort of consecutive patients with cardiogenic shock treated with primary PCI METHODOLOGY: Data collected from PCI registry of 80 centres in germany from July 1994- Mar 2001 INCLUSION CRIT.: All patients with AMI with shock <24 hrs EXCLUSION : pt who were lysed before PCI SAMPLE SIZE:A total of 9422 procedures were registered, of these 1333 (14.2%) were performed in patients with cardiogenic shock
 were performed in patients with cardiogenic shock")
70
RESULTS

72
Total in-hospital mortality was 46.1% and was dependent on TIMI flow grade after PCI In a multivariate analysis left main disease, TIMI <3 flow after PCI, older age, TVD and longer time-intervals between symptom onset &PCI -independent predictors of mortality Significant decrease in mortality over the years (P for trend 0.02) CONCLUSION: Younger age, absence of TVD, shorter time between symptom-onset and PCI, and the achievement of TIMI 3 flow - best predictors of an improved in-hospital mortality. The decision for interventional therapy in the elderly (>75 years) to be individualized
 to be individualized.")
73
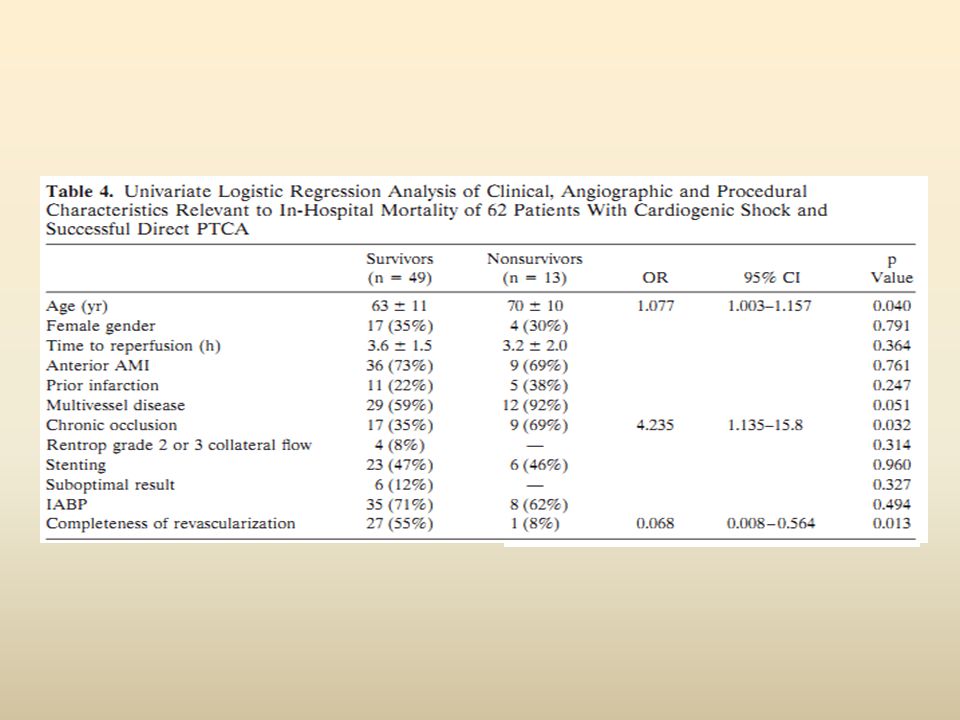
Objectives. This prospective observational study was conducted to examine the apparent impact of a systematic direct PTCA strategy on mortality in a series of 66 consecutive patients with AMI complicated by CS, and to analyze the predictors of outcome after successful direct PTCA. INCLUSION CRITERIA : 1)STEMI< 6 HRS of symptom onset 2) STEMI with ongoing ischaemia 6-24 hrs EXCLUSION CRIT.: 1)Thrombolyzed 2)Angiographic exclusion criteria for direct PTCA were a)infarct-related artery diameter stenosis,70%, b)inability to identify the infarct-related artery. 3)Patients with septal or papillary muscle rupture
STEMI< 6 HRS of symptom onset 2) STEMI with ongoing ischaemia 6-24 hrs EXCLUSION CRIT.: 1)Thrombolyzed 2)Angiographic exclusion criteria for direct PTCA were a)infarct-related artery diameter stenosis,70%, b)inability to identify the infarct-related artery. 3)Patients with septal or papillary muscle rupture.")
74
RESULTS

76
CONCLUSION: Systematic direct PTCA, including stent supported PTCA, can establish a Thrombolysis in Myocardial Infarction (TIMI) 3 flow in majority of patients presenting with AMI and early CS Results.: In patients with CS, direct PTCA had a success rate of 94%; optimal angiographic result was achieved in 85%; primary stenting of the IRA was accomplished in 47%; and the in hospital mortality rate was 26%. Univariate analysis showed that patient age, chronic coronary occlusion and completeness of revascularization were significantly related to in-hospital mortality. The mean follow-up period was 16 months. Survival rate at 6 months was 71%. Comparison of event-free survival in patients with a stented or nonstented infarct-related artery suggests an initial and long-term benefit of primary stenting.

77
ESC GUIDELINE 2012 AHA GUIDELINE 2013

78
THANK YOU

Similar presentations






 AHA, 2008.>")








>")








 after thrombolytic therapy By Dr. Mohamed Mahros Assistant lecturer of cardiology Benha faculty of medicine.>")
