Download presentation
Presentation is loading. Please wait.

1
DRUG THERAPY OF AIRFLOW OBSTRUCTION PROFESSOR B J LIPWORTH Preventers (anti-inflammatory)Preventers (anti-inflammatory) Relievers (bronchodilators)Relievers (bronchodilators)
Preventers (anti-inflammatory) Relievers (bronchodilators)Relievers (bronchodilators)")
2
THE INFLAMMATORY CASCADE Genetic predisposition + Trigger factor Avoidance (e.g. viral, allergen, chemicals) (e.g. viral, allergen, chemicals) Airway inflammation Anti-inflammatory - corticosteroid Airway inflammation Anti-inflammatory - corticosteroid Mediators Anti-leukotriene Mediators Anti-leukotriene (e.g. histamine, leukotriene) Anti-histamine (e.g. histamine, leukotriene) Anti-histamine Twitchy smooth muscle Bronchodilators Twitchy smooth muscle Bronchodilators (Hyper-reactivity) - 2 -agonists (Hyper-reactivity) - 2 -agonists
 (e.g. viral, allergen, chemicals) Airway inflammation Anti-inflammatory - corticosteroid Airway inflammation Anti-inflammatory - corticosteroid Mediators Anti-leukotriene Mediators Anti-leukotriene (e.g. histamine, leukotriene) Anti-histamine (e.g. histamine, leukotriene) Anti-histamine Twitchy smooth muscle Bronchodilators Twitchy smooth muscle Bronchodilators (Hyper-reactivity) - 2 -agonists (Hyper-reactivity) - 2 -agonists.")
3
THE ASTHMA TREATMENT PYRAMID Oral Oral Steroid Steroid Controller Theophylline (Additive to ICS ) Leukotriene-antagonist Increasing Long-acting 2 -agonist severity Long-acting 2 -agonist severity Preventer Inhaled steroid ( Cromogylcate ?) ( Cromogylcate ?) Reliever Short-acting 2 -agonist PRN
 Leukotriene-antagonist Increasing Long-acting 2 -agonist severity Long-acting 2 -agonist severity Preventer Inhaled steroid ( Cromogylcate ) ( Cromogylcate ) Reliever Short-acting 2 -agonist PRN")
4
BTS Asthma Guidelines intermittent mild persistent moderate persistent severe persistent Short-acting ß2 agonists prn Inhaled steroids Add on LABA Add on LTRA/Theo Step 1 Step 2 Step 3 Step 4

7
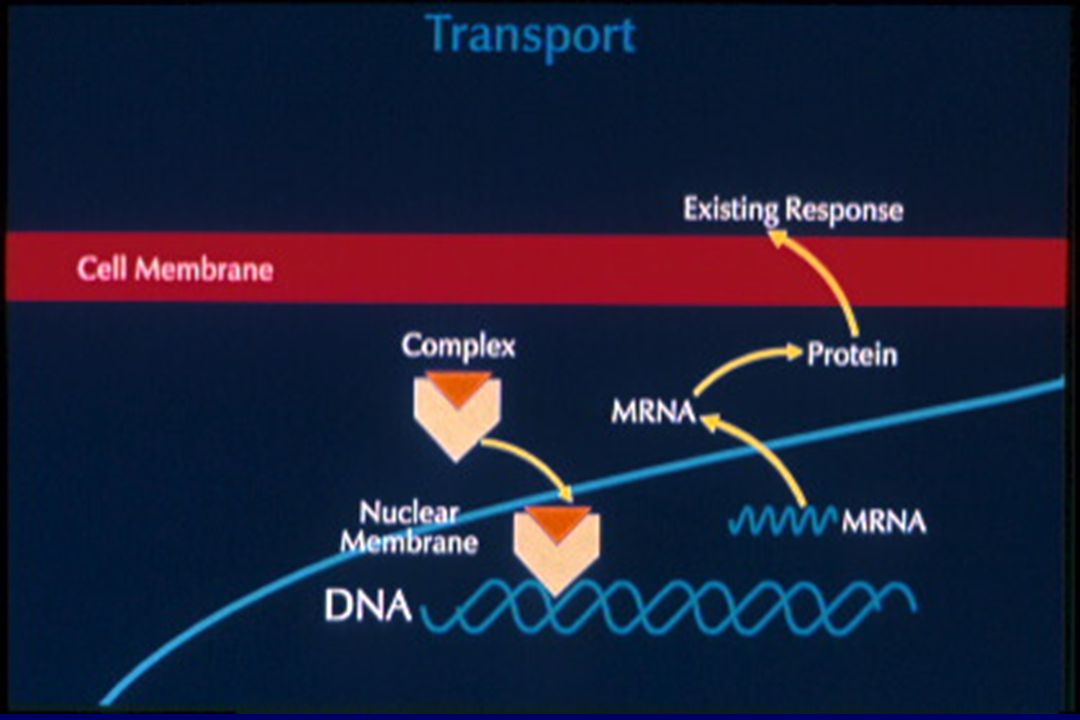
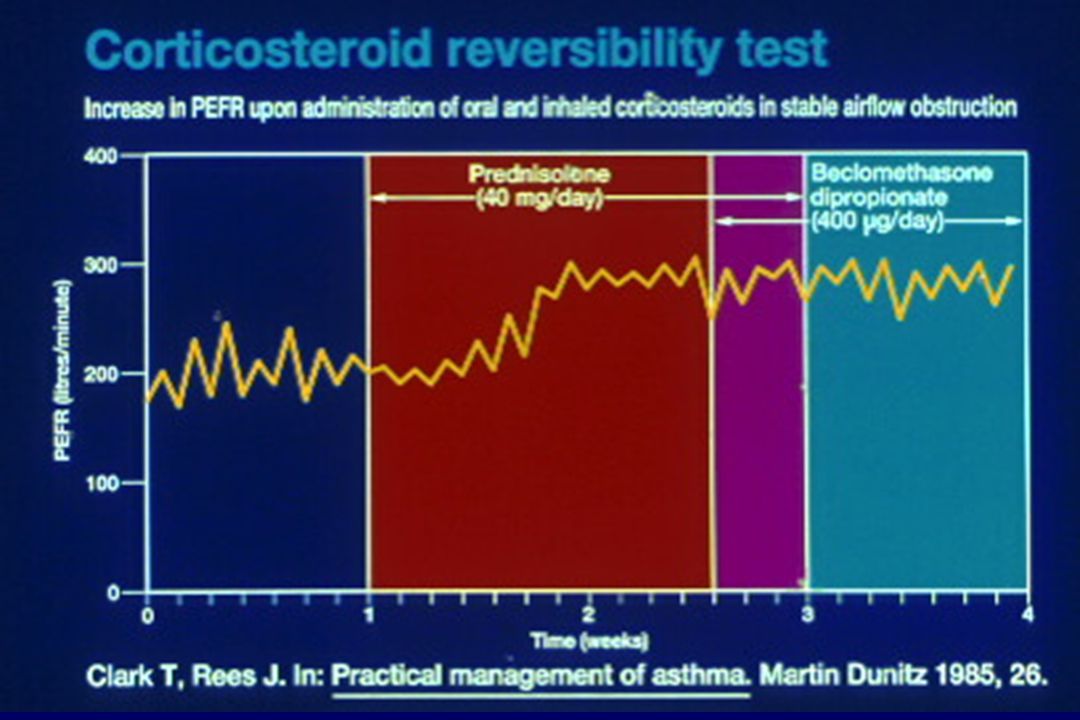
ANTI-INFLAMMATORY: CORTICOSTEROIDS Used in asthma and COPDUsed in asthma and COPD Oral steroid (prednisolone) - low therapeutic ratioOral steroid (prednisolone) - low therapeutic ratio - only used for acute exacerbations Inhaled steroid (beclomethasone) - higher therapeutic ratioInhaled steroid (beclomethasone) - higher therapeutic ratio - used for maintenance therapy Optimise lung delivery - large volume spacerOptimise lung delivery - large volume spacer
 - low therapeutic ratioOral steroid (prednisolone) - low therapeutic ratio - only used for acute exacerbations Inhaled steroid (beclomethasone) - higher therapeutic ratioInhaled steroid (beclomethasone) - higher therapeutic ratio - used for maintenance therapy Optimise lung delivery - large volume spacerOptimise lung delivery - large volume spacer")
10
Lung deposition of HFA-BDP, fluticasone and CFC-BDP MMAD = 1.1 µmMMAD = 2.5 µmMMAD = 3.5 µm

12
Actions of a spacer device Avoids coordination problems with pMDI Reduces oropharyngeal and laryngeal side effects Reduces systemic absorption from swallowed fraction Acts a holding chamber for aerosol Reduces particle size and velocity Improves lung deposition

14
ANTI-INFLAMMATORY: CROMONES Only used in asthma (eg Cromoglycate)Only used in asthma (eg Cromoglycate) Mast cell stabiliser - weak anti-inflammatory cf steroidsMast cell stabiliser - weak anti-inflammatory cf steroids Cromoglycate effective in atopic children (exercise asthma)Cromoglycate effective in atopic children (exercise asthma) Inhaled route only (compliance with QID dosing )Inhaled route only (compliance with QID dosing ) No longer used due to poor efficacyNo longer used due to poor efficacy
Only used in asthma (eg Cromoglycate) Mast cell stabiliser - weak anti-inflammatory cf steroidsMast cell stabiliser - weak anti-inflammatory cf steroids Cromoglycate effective in atopic children (exercise asthma)Cromoglycate effective in atopic children (exercise asthma) Inhaled route only (compliance with QID dosing )Inhaled route only (compliance with QID dosing ) No longer used due to poor efficacyNo longer used due to poor efficacy")
17
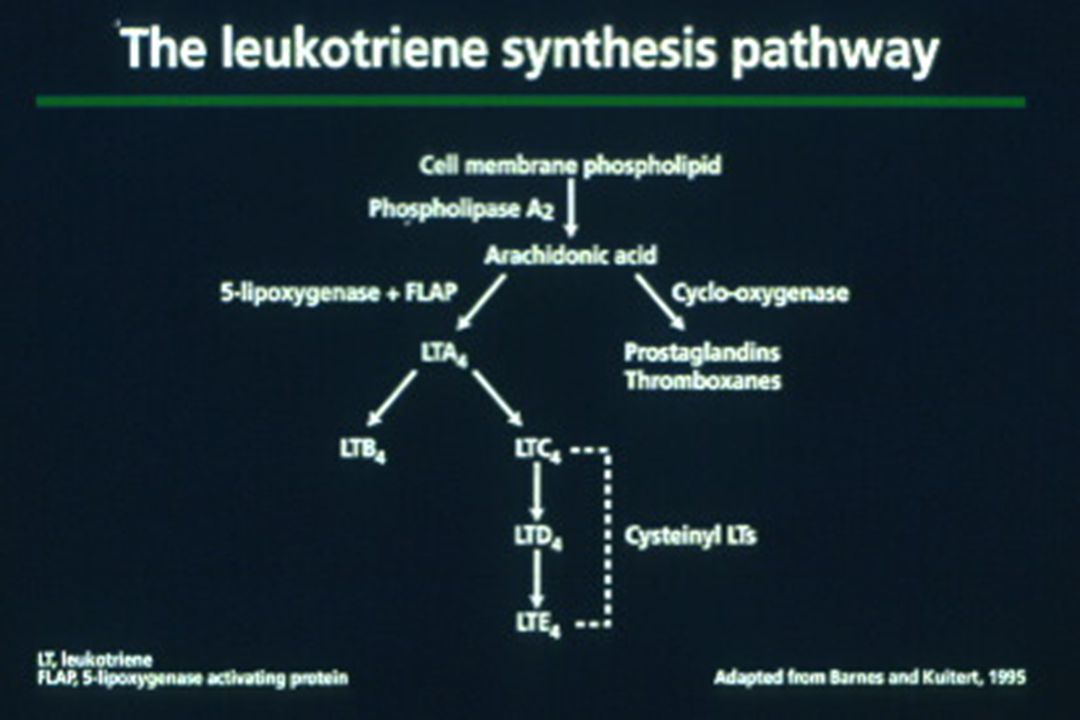
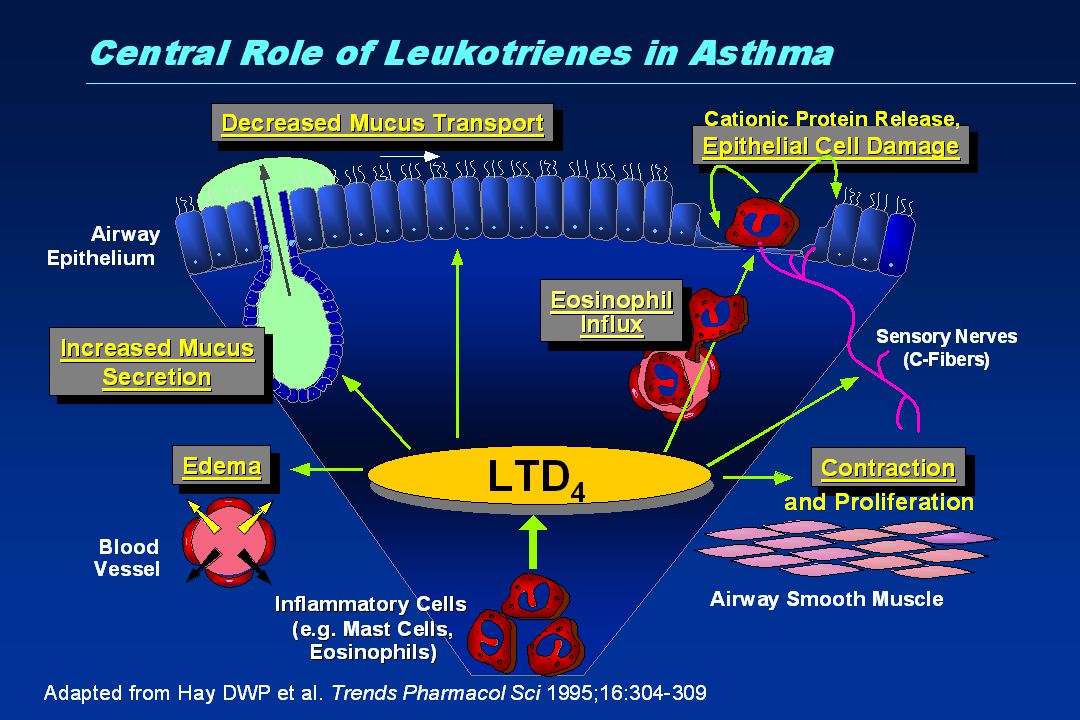
ANTI-INFLAMMATORY: LEUKOTRIENE RECEPTOR ANTAGONISTS Only used in asthma: bronchodilator + anti-inflammatoryOnly used in asthma: bronchodilator + anti-inflammatory Montelukast - oral route,once daily, high therapeutic ratioMontelukast - oral route,once daily, high therapeutic ratio Less potent anti-inflammatory than inhaled steroidLess potent anti-inflammatory than inhaled steroid 2nd line: complimenatary non steroidal ant-inflammatory additive to inhaled steroid 2nd line: complimenatary non steroidal ant-inflammatory additive to inhaled steroid Effective in exercise induced asthmaEffective in exercise induced asthma Also effective in allergic rhinitis ( with anti-histamine )Also effective in allergic rhinitis ( with anti-histamine )
Also effective in allergic rhinitis ( with anti-histamine )")
18
ANTI-INFLAMMATORY: ANTIHISTAMINES H 1 receptor antagonistsH 1 receptor antagonists Oral routeOral route Only of value when known allergenic trigger (e.g. HDM,pollen or cat) -ie in atopic asthmaOnly of value when known allergenic trigger (e.g. HDM,pollen or cat) -ie in atopic asthma 1 st generation :Chlorpheniramine-sedative1 st generation :Chlorpheniramine-sedative 2 nd generation: Cetirizine,Loratadine-non sedative2 nd generation: Cetirizine,Loratadine-non sedative 3 rd generation: Levocetirizine,Desloratadine - non sedative3 rd generation: Levocetirizine,Desloratadine - non sedative More effective in allergic rhinitis than asthmaMore effective in allergic rhinitis than asthma Additive effects when given together with leukotreine antagonistAdditive effects when given together with leukotreine antagonist
 -ie in atopic asthmaOnly of value when known allergenic trigger (e.g. HDM,pollen or cat) -ie in atopic asthma 1 st generation :Chlorpheniramine-sedative1 st generation :Chlorpheniramine-sedative 2 nd generation: Cetirizine,Loratadine-non sedative2 nd generation: Cetirizine,Loratadine-non sedative 3 rd generation: Levocetirizine,Desloratadine - non sedative3 rd generation: Levocetirizine,Desloratadine - non sedative More effective in allergic rhinitis than asthmaMore effective in allergic rhinitis than asthma Additive effects when given together with leukotreine antagonistAdditive effects when given together with leukotreine antagonist.")
19
ANTI-INFLMMATORY Anti-IgE Anti-IgE monoclonal antibody : Omalizumab (Xolair) Omalizumab inhibits the binding to the high-affinity IgE receptor and inhibit mediator release from basophils and mast cells. Injection every 2-4 weeks. For patients with severe persistent allergic asthma despite max therapy –ie step 5. Very expensive. No effect on pulmonary function but reduces exacerbations.

20
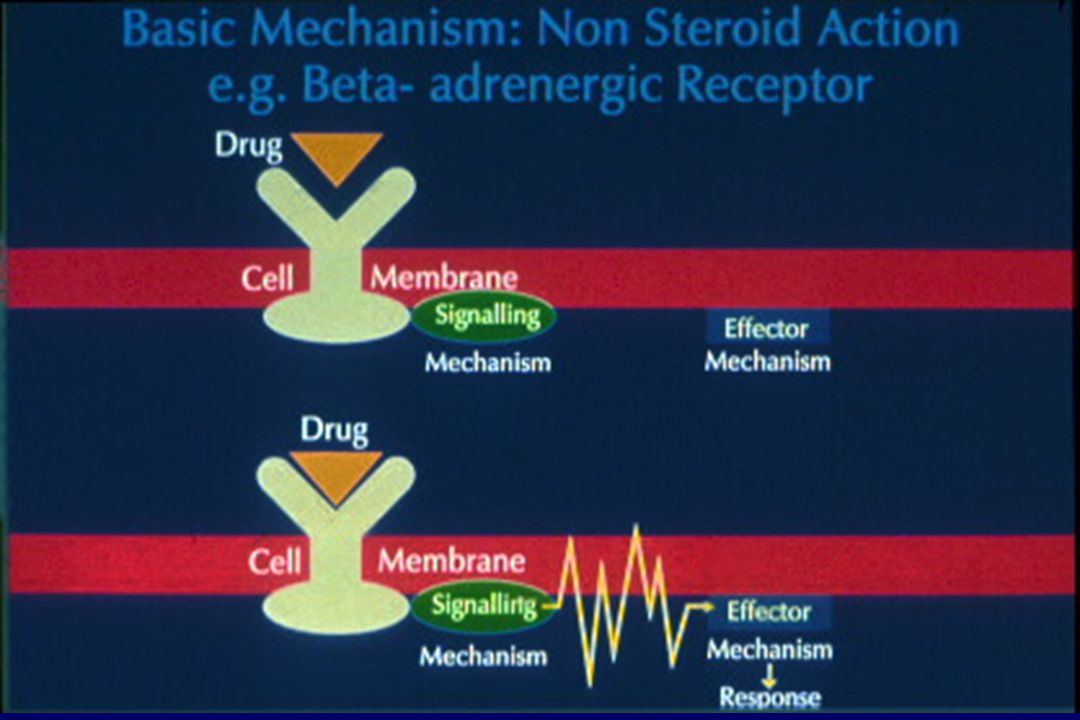
BRONCHODILATORS: 2 -AGONISTS Stimulate bronchial smooth muscle 2 -receptors: cAMPStimulate bronchial smooth muscle 2 -receptors: cAMP Short-acting - salbutamolShort-acting - salbutamol Long-acting – salmeterol / formoterolLong-acting – salmeterol / formoterol Combination inhalers-eg Seretide / SymbicortCombination inhalers-eg Seretide / Symbicort Used in asthma and COPDUsed in asthma and COPD High therapeutic ratio when given by inhaled routeHigh therapeutic ratio when given by inhaled route Systemic 2 effects when given systemically or at high inhaled dosesSystemic 2 effects when given systemically or at high inhaled doses High nebulised doses given in acute attackHigh nebulised doses given in acute attack

21
Muscarinic (cholinergic) receptors sM 1 -receptors enhance the cholinergic reflex sM 2 -receptors inhibit acetylcholine release sM 3 -receptors mediate bronchoconstriction and mucus secretion
 receptors sM 1 -receptors enhance the cholinergic reflex sM 2 -receptors inhibit acetylcholine release sM 3 -receptors mediate bronchoconstriction and mucus secretion")
22
BRONCHODILATORS: ANTICHOLINERGICS Block post junctional end plate M 3 receptorsBlock post junctional end plate M 3 receptors Ipratropium qid, Tiotropium od - inhaled route only - high therapeutic ratioIpratropium qid, Tiotropium od - inhaled route only - high therapeutic ratio Used in COPD - less effective in asthmaUsed in COPD - less effective in asthma High nebulised doses of ipratropium used in acute COPD and in acute asthmaHigh nebulised doses of ipratropium used in acute COPD and in acute asthma

23
BRONCHODILATOR/ANTINFLAMMATORY:METHYLXANTHINES Oral (Theophylline) for maintenance therapyOral (Theophylline) for maintenance therapy SR formulation useful for nocturnal dipsSR formulation useful for nocturnal dips Used as add to inhaled steroid as complimentary non steroidal anti-inflammatoryUsed as add to inhaled steroid as complimentary non steroidal anti-inflammatory IV (Aminophylline) for acute attacksIV (Aminophylline) for acute attacks Non selective phosphodiesterase inhibitor ( cAMP)Non selective phosphodiesterase inhibitor ( cAMP) Adenosine antagonistAdenosine antagonist Low therapeutic ratio - P450 drug interactions (e.g. erythromycin)Low therapeutic ratio - P450 drug interactions (e.g. erythromycin) Used in asthma and COPDUsed in asthma and COPD
Low therapeutic ratio - P450 drug interactions (e.g. erythromycin) Used in asthma and COPDUsed in asthma and COPD.")
24
Anti-inflammatory :PDE4 inhibitors Roflumilast –oral tablet od Indicated for COPD only Minimal effect on FEV1 Reduces exacerbations –additive to LABA or LAMA Adverse effects : Nausea/Diarrhoea/Headache/Weight loss ? Place in COPD guidelines as add on to ICS/LABA/LAMA

25
Mucolytics Oral carbocisteine, erdosteine To reduce sputum viscosity and aide sputum expectoration [and reduce exacerbations ] in COPD Rarely used –only as add on to other treatments
![Mucolytics Oral carbocisteine, erdosteine To reduce sputum viscosity and aide sputum expectoration [and reduce exacerbations ] in COPD Rarely used –only as add on to other treatments](http://images.slideplayer.com/15/4651674/slides/slide_25.jpg "Mucolytics Oral carbocisteine, erdosteine To reduce sputum viscosity and aide sputum expectoration [and reduce exacerbations ] in COPD Rarely used –only as add on to other treatments")
26
TREATMENT OF CHRONIC ASTHMA AIMS: Abolish sympt, min 2 -use, normalise FEV 1, reduce PEF variability, reduce exac, prevent long term airway remodAIMS: Abolish sympt, min 2 -use, normalise FEV 1, reduce PEF variability, reduce exac, prevent long term airway remod Avoid triggersAvoid triggers Suppress inflammatory cascade with inh steroidSuppress inflammatory cascade with inh steroid +/- non steroidal anti-inflamm therapy –eg theophylline,anti- leukotriene,anti-histamine +/- non steroidal anti-inflamm therapy –eg theophylline,anti- leukotriene,anti-histamine Stabilise smooth muscle with LABA –only once optimal anti- inflamm therapy in placeStabilise smooth muscle with LABA –only once optimal anti- inflamm therapy in place

27
TREATMENT OF ACUTE ASTHMA Oral prednisolone (or iv hydrocortisone )Oral prednisolone (or iv hydrocortisone ) Nebulised high dose salbutamol, ± Neb ipratropium, ± iv aminophylline/magnesiumNebulised high dose salbutamol, ± Neb ipratropium, ± iv aminophylline/magnesium 60% O 260% O 2 ITU Assisted mecahnical intubated ventilation if falling PaO 2 and rising PaCO 2ITU Assisted mecahnical intubated ventilation if falling PaO 2 and rising PaCO 2 - never use respiratory stimulant
Oral prednisolone (or iv hydrocortisone ) Nebulised high dose salbutamol, ± Neb ipratropium, ± iv aminophylline/magnesiumNebulised high dose salbutamol, ± Neb ipratropium, ± iv aminophylline/magnesium 60% O 260% O 2 ITU Assisted mecahnical intubated ventilation if falling PaO 2 and rising PaCO 2ITU Assisted mecahnical intubated ventilation if falling PaO 2 and rising PaCO 2 - never use respiratory stimulant")
29
Non-pharmacological intervention: smoking cessation Fletcher et al., 1977 FEV 1 (% of value at age 25) 100 75 50 25 0 255075 Never smoked or not susceptible to smoke Stopped at 65 Stopped at 45 Disability Smoked regularly and susceptible to its effects Death Age (years)
 Never smoked or not susceptible to smoke Stopped at 65 Stopped at 45 Disability Smoked regularly and susceptible to its effects Death Age (years)")
30
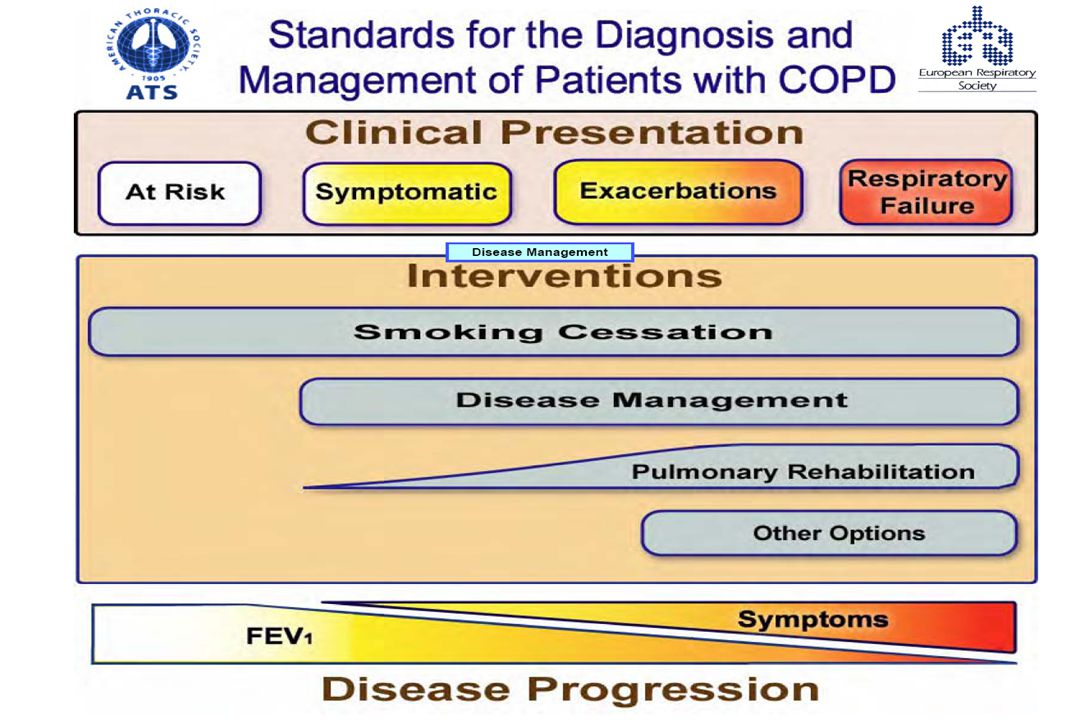
TREATMENT OF STABLE COPD TREATMENT OF STABLE COPD Prevent FEV 1 decline - stop smokingPrevent FEV 1 decline - stop smoking Treat reversible componentTreat reversible component - Inhaled steroid - Short/Long acting beta-2 agonists - Short/Long acting anticholinergics -Theophylline -Theophylline Pulm rehabPulm rehab Vaccination –influenza/pneumococcalVaccination –influenza/pneumococcal Domiciliary O 2 to prevent cor pulmonaleDomiciliary O 2 to prevent cor pulmonale Venesection for polycythaemiaVenesection for polycythaemia Lung volume reduction surgery for highly slected patientsLung volume reduction surgery for highly slected patients

31
TREATMENT OF ACUTE COPD Nebulised high dose salbutamol + ipratropiumNebulised high dose salbutamol + ipratropium Oral prednisoloneOral prednisolone Antibiotic (amoxycillin) if infectionAntibiotic (amoxycillin) if infection 24-28% O 224-28% O 2 Respiratory stimulant (doxapram) to improve ventilationRespiratory stimulant (doxapram) to improve ventilation Non invasive ventilation instead of doxapramNon invasive ventilation instead of doxapram ITU Intubated assisted ventilation only if reversible component (eg pneumonia)ITU Intubated assisted ventilation only if reversible component (eg pneumonia)
 if infectionAntibiotic (amoxycillin) if infection 24-28% O % O 2 Respiratory stimulant (doxapram) to improve ventilationRespiratory stimulant (doxapram) to improve ventilation Non invasive ventilation instead of doxapramNon invasive ventilation instead of doxapram ITU Intubated assisted ventilation only if reversible component (eg pneumonia)ITU Intubated assisted ventilation only if reversible component (eg pneumonia)")
Similar presentations


>")

 SOB Cough Wheezing Tight chest.>")













>")

 Huifang Tang ( 汤慧芳 ) Department of Pharmacology Zhejiang university, school of Medicine>")
