Download presentation
Presentation is loading. Please wait.

1
The Genetics of Cancer: Is Personalization of Cancer Treatment Possible? Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center

2
Disclosures Board of Directors: Clovis Oncology, Loxo Oncology Scientific Advisory Board: Sanofi, Ziopharm, Oncoceutics, Raze, X4 Therapeutics Consultant: GSK, Novartis, Roche, Merck, Amgen, Array, Cerulean, Momenta

3
Somatic mutation burden by cancer type Alexandrov et al. Nature 2013

4
Mutation patterns sort into distinct subgroups Alexandrov et al. Nature 2013

5
BRAF, NRAS and NF1 define mutually exclusive subsets of melanoma Cancer Genome Atlas Research Network et al. TCGA symposium 2012 200

6
50% 25% 10% Melanoma: the model of MAP kinase dependence Sullivan RJ & Flaherty KT. CCR 2014

7
Recurrent concomitant mutations in BRAF mutant melanoma Cancer Genome Atlas Research Network et al. TCGA symposium 2012 AKT3 MDM2 BRAF MITF

8
Tumor regression V600E BRAF mutant melanoma patients (vemurafenib) RECIST 30% Decrease Sosman J et al. NEJM 2012

9
BRAF vs. BRAF/MEK combination in V600E BRAF mutant melanoma patients Maximum percent reduction from baseline measurement Best confirmed response Complete response Partial responseProgressive disease Stable disease Dabrafenib monotherapy Dabrafenib 150 mg BID/Trametinib 2 mg QD Long G et al. ESMO 2012

10
Tumor regression to erlotinib in EGFR mutant NSCLC Rizvi N et al. CCR 2011

11
Tumor regression to crizotinib in ALK translocated NSCLC Camidge R et al. Lancet Oncol 2012

12
BRAF inhibition in V600E BRAF melanoma & colon cancer Kopetz, ASCO 2010 melanomacolorectal Sosman J et al. NEJM 2012

13
Feedback mechanisms in the MAP kinase pathway Mendoza et al. Trends Biochem Sci. 2011

14
Vemurafenib (BRAFi) or dabrafenib/trametinib (BRAF/MEKi) in BRAF mutant colorectal cancer Kopetz, ASCO 2010Corcoran ASCO 2012
 or dabrafenib/trametinib (BRAF/MEKi) in BRAF mutant colorectal cancer Kopetz, ASCO 2010Corcoran ASCO 2012")
15
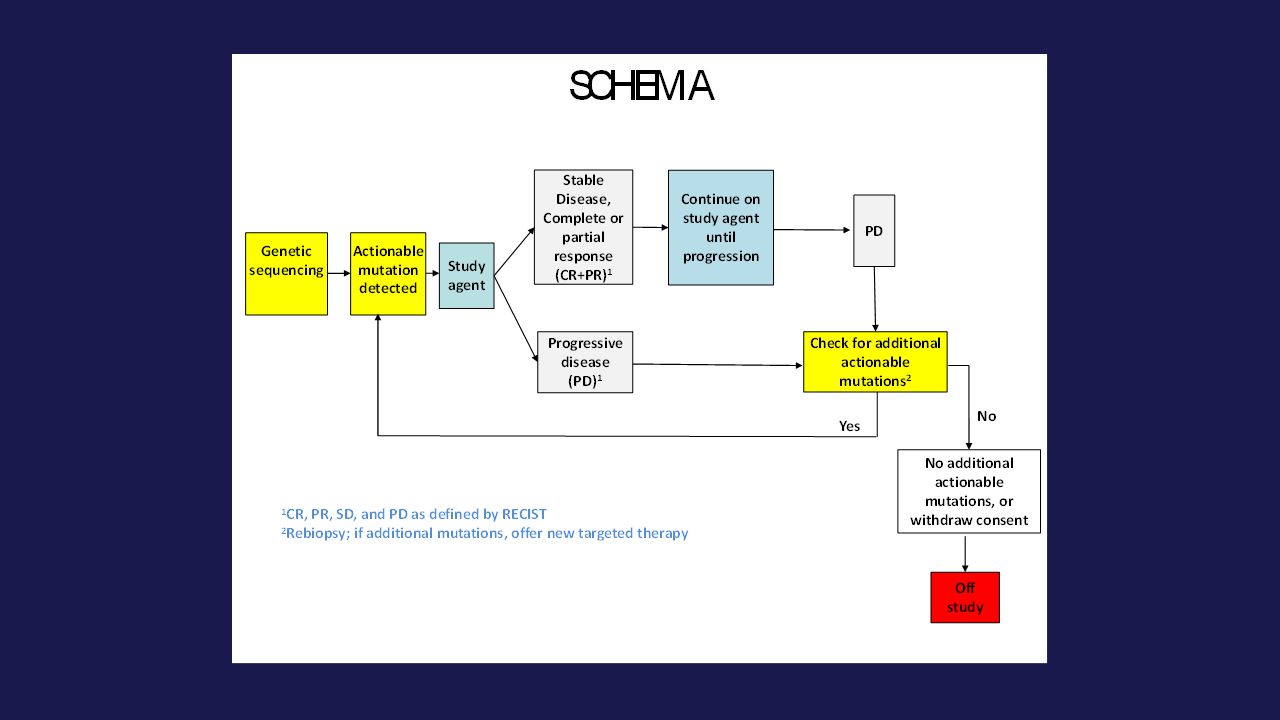
NCI MATCH Identify mutations/amplifications/translocations in patient tumor sample - eligibility determination Assign patient to relevant agent/regimen Need to sequence large numbers of tumors and need to have large numbers of targeted treatments Tumor biopsies & sequencing at progression to illuminate resistance mechanisms –De-identified samples submitted to central labs –Whole-exome sequencing (research purposes)
")
17
Eligibility Patients with solid tumors or lymphomas whose disease has progressed following at least one line of standard systemic therapy (or with tumors that do not have standard therapy) –Exclude histologies that had been approved by the FDA or had shown lack of efficacy with an agent Tumor accessible to biopsy and patient willing to undergo biopsy Adults Performance status ECOG 0-1 Adequate organ function
 –Exclude histologies that had been approved by the FDA or had shown lack of efficacy with an agent Tumor accessible to biopsy and patient willing to undergo biopsy Adults Performance status ECOG 0-1 Adequate organ function")
18
Patient population considerations Target: at least 25% of total enrollment to be patients who have “rare” tumors “Common” defined as breast, NSCLC, colon, prostate

19
Statistical Design Statistical Considerations (within each drug-by-mutation category) Primary Endpoint: Overall Response Rate 5% vs. 25% One stage design 31 evaluable patients per arm

20
CLIA lab network Genetic platform: Ion Torrent PGM Ampliseq custom panel –About 200 genes –SNV, indel, CNV, targeted translocations Validation within and across sites: same SOP Selected IHC, FISH Competitively chosen lab sites: –MDAnderson (Hamilton) –MGH (Iafrate) –Yale (Sklar)
 –MGH (Iafrate) –Yale (Sklar)")
21
Tumor Biopsy Prior to study entry a biopsy (4 cores) FFPE, shipped to MDACC Adjacent section H&E stained, examined by pathologist for tumor content, % necrosis, inflammation, and scanned into high resolution image database RNA and DNA extracted from the same tissue section Planned research assays: –If sufficient DNA is available, whole-exome sequencing can be performed for research –RNA will be used for research grade gene expression profiling by either whole-transcriptome or miRNA microarray analysis Biopsy on progression
 FFPE, shipped to MDACC Adjacent section H&E stained, examined by pathologist for tumor content, % necrosis, inflammation, and scanned into high resolution image database RNA and DNA extracted from the same tissue section Planned research assays: –If sufficient DNA is available, whole-exome sequencing can be performed for research –RNA will be used for research grade gene expression profiling by either whole-transcriptome or miRNA microarray analysis Biopsy on progression")
22
MATCH Assay Workflow and Turnover Time 22 Tissue Fixation Path Review Nucleic Acid Extraction Library/Template Prep Sequencing aMOI Report Review Sanger Verification Biopsy Received 3 DAYS 1 DAY 3 DAYS 10-14 days Final Report Tumor content >50% DNA yield > 20 ng Library yield > 20 pM Test fragments Total read Reads per BC Coverage NTC, Positive, Negative Controls

23
Rules of evidence for “actionable” variants Level 1: Credentialed for selection of an FDA approved drug Level 2a: Eligibility trial for an ongoing trial Level 2b: N-of-1 response (with mechanistic basis) Level 3: Preclinical data with known PK/PD –Selective activity in biomarker-defined model –Functional evidence that alterations in target lead to upregulation & dependence –Functional evidence of pathway activation as consequence of loss of function in tumor suppressor
 Level 3: Preclinical data with known PK/PD –Selective activity in biomarker-defined model –Functional evidence that alterations in target lead to upregulation & dependence –Functional evidence of pathway activation as consequence of loss of function in tumor suppressor")
24
First round of committed agents DrugMolecular Targets AfatinibEGFR activating (non NSCLC) AfatinibHER2 kinase activating AMG 337MET amplification AMG 595EGFR vIII AZD 9291EGFR T790M (non NSCLC) CrizotinibALK fusions CrizotinibROS translocations Dabrafenib + TrametinibBRAF V600E (nonmelanoma) GDC 0032PIK3CA ampl/mut; WT RAS, No PTEN loss GSK2636771PTEN Mut, PTEN IHC+ GSK2636771PTEN Mut, PTEN IHC – GSK2636771PTEN wt, PTEN IHC - JNJ 493Ampl FGFR 1,2, or 4; FGFR mut MLN 0128mTOR mut MLN 0128TSC1 or TSC2 mut SunitinibKIT mutations TDM-1HER 2 ampl (non breast or gastric) TrametinibBRAF nonV600E or fusions TrametinibNF1 mut (arm1) GNAQ,GNA11 mut (arm 2) Trastuzumab/pertuzumabHER2 ampl (non breast or gastric) VismodegibSMO or PTCH mut VS 6063NF2 loss
 AfatinibHER2 kinase activating AMG 337MET amplification AMG 595EGFR vIII AZD 9291EGFR T790M (non NSCLC) CrizotinibALK fusions CrizotinibROS translocations Dabrafenib + TrametinibBRAF V600E (nonmelanoma) GDC 0032PIK3CA ampl/mut; WT RAS, No PTEN loss GSK PTEN Mut, PTEN IHC+ GSK PTEN Mut, PTEN IHC – GSK PTEN wt, PTEN IHC - JNJ 493Ampl FGFR 1,2, or 4; FGFR mut MLN 0128mTOR mut MLN 0128TSC1 or TSC2 mut SunitinibKIT mutations TDM-1HER 2 ampl (non breast or gastric) TrametinibBRAF nonV600E or fusions TrametinibNF1 mut (arm1) GNAQ,GNA11 mut (arm 2) Trastuzumab/pertuzumabHER2 ampl (non breast or gastric) VismodegibSMO or PTCH mut VS 6063NF2 loss")
25
Logistics Master Protocol with Multi-arm phase II trials IND for protocol template –Arms could be added or deleted without affecting other arms Single agents or combinationsf where recommended phase 2 dose is known FDA Approved (for a different indication) or investigational agents Central IRB 2400 NCTN sites CLIA lab network: validated assay
 or investigational agents Central IRB 2400 NCTN sites CLIA lab network: validated assay")
26
NCI: Developing a National Strategy for Precision Medicine NCI-MATCH Clinical trial (Genotype to Phenotype) –Screen for molecular features that may predict response to a drug with a given mechanism of action Genomics of Exceptional Responders (Phenotype to Genotype) –Tumor from patients who had an exceptional response to a drug for which predictive biomarkers are not known
 –Screen for molecular features that may predict response to a drug with a given mechanism of action Genomics of Exceptional Responders (Phenotype to Genotype) –Tumor from patients who had an exceptional response to a drug for which predictive biomarkers are not known")
27
Acknowledgements MATCH trial leadership: NCI - Alice Chen, Barb Conley, Mickey Williams ECOG-ACRIN - Peter O’Dwyer, Stan Hamilton

Similar presentations


 Design. Prospective Co-Development of Drugs and Companion Diagnostics 1. Develop a completely specified genomic classifier of the.>")








 1 Concordance of HER2 Central Assessment.>")

 Comparing BRAF Inhibitor.>")


 in Metastatic Castration-Resistant Prostate Cancer (mCRPC): Results from a Phase II Randomized Discontinuation Trial Hussain M et.>")
 in Non-Small Cell Lung Cancer (NSCLC) Victor.>")

