Download presentation
Presentation is loading. Please wait.

1
University of DundeeSchool of Medicine Best practice in managing pneumonia: Scottish National Audit Project – Community Acquired Pneumonia (SNAP-CAP) Peter Davey
 Peter Davey")
2
Agenda What is a care bundle? How do care bundles work? How are bundle elements selected? How do you measure bundle implementation? What is a driver diagram?

3
Ventilator Bundle Elevating the head of the patient’s bed Daily "sedation vacations," or gradually lightening the use of sedatives each day Daily assessment of the patient’s readiness to extubate or wean from the ventilator Chlorhexidine oral care

4
PatientMeasure 1Measure 2Measure 3Measure 4All measures? 1Yes 2 NoYes No 3Yes No 4Yes 5 No 6YesNoYesNo 7 Yes No 8Yes 9 No YesNo 10Yes Reliability.90.70.80.60.40 Ventilator Bundle

5
BMJ Dec 20 2003, 327: 1459-61 We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute

6
The Fundamental Question About Cause and Effect Is there any other way of explaining the set of facts before us, is there any other answer equally, or more, likely than cause and effect? Bradford Hill 1966

7
Inference of Causality 1.Strength of association 2.Consistency 3.Specificity 4.Relationship in time 5.Biological gradient 6.Biological plausibility 7.Coherence of evidence 8.Experiment 9.Analogy Bradford Hill 1937

8
Antibiotics within 4h – Statistically significant – Consistent association – Biologically plausible – Biological gradient – Evidence that change influences outcome – Analogy with septic shock Blood culture – Statistically significant – Consistent association – +ve in <10% patients – Does not change practice when +ve – No evidence that change influences outcome Two Quality Indicators for CAP: Should they be in a bundle?

9
Take blood cultures Good Clinical Teams Reduce deaths from CAP Confounding

10
http://www.scottishmedicines.org.uk/smc/7296.221.249.html
12
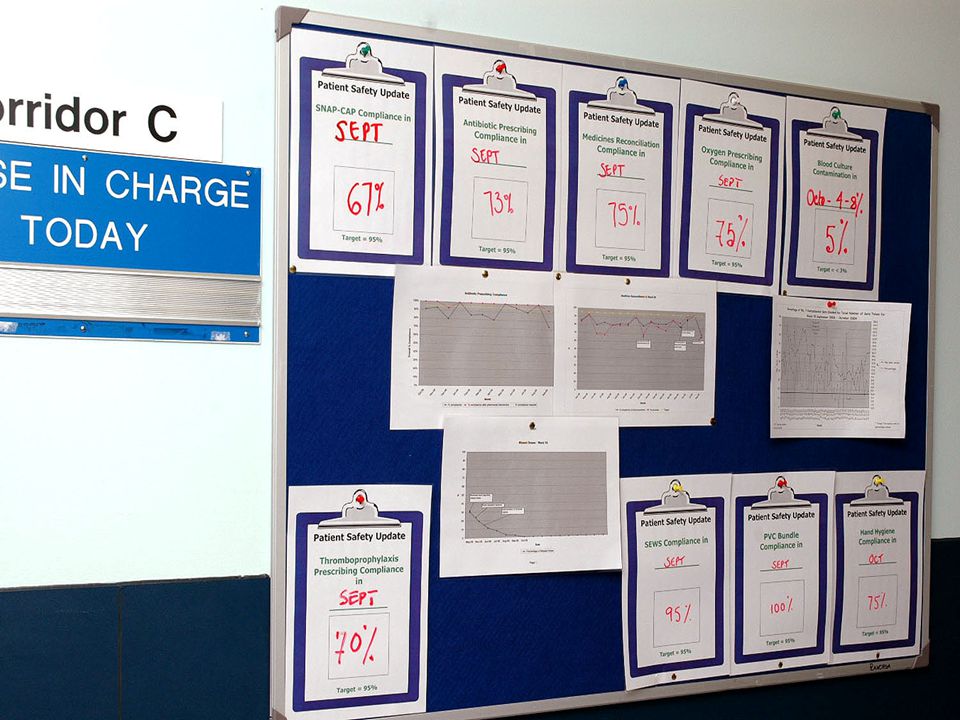
How do bundles work? Commitment to highly reliable processes of care Changing the culture to one that supports improvement

13
Copyright ©2006 BMJ Publishing Group Ltd. Jain, M et al. Qual Saf Health Care 2006;15:235-239 Figure 2 Run chart of number of adverse events in the ICU (adverse events defined in box 1).11
.11.")
16
O 2 Assessment in Severe CAP Blot et al 2007 Crit Care Med 35: 2509-2514

17
What Can We Learn? 1.Test the validity and reliability of the measures and the benefits, harms, and costs of implementation. 2.Does an all-or-none threshold create undue pressure to treat, even when clinically inappropriate? 3.Key end-users must be “at the table” during development and approval of quality metrics 4.Review the validity, reliability, impact, and costs of measures within 1 to 2 years after implementation

21
Acute Medical Admissions Unit ABS Driver Diagram Outcomes Improved outcomes ↓ Mortality ↓ Unnecessary admissions ↓ C difficile infections Primary Drivers Provide reliable timely, care using evidence based therapies Develop infrastructure that enables junior doctors to provide quality care Create a collaborative team culture focused on quality & safety Secondary Drivers Integrate patient and family into care Prescribe oxygen for all patients CURB65 risk score on all CAP patients Prioritise CXR for CAP Give first dose of antibiotics immediately Stratify CAP care by risk Document the diagnosis for every patient Ensure antibiotic treatment is per policy Safety dashboard Support low risk patients for self care at home Clarify care wishes and EOL planning Pre-printed oxygen prescriptions Systems review for prioritisation of CXR Focus induction of new staff on improvement Negotiate administration of first dose in A&E Reliable planning, communication and collaboration of multi disciplinary team Prioritise investigations that influence treatment in the first 4h after admission Maintain quality of care 24-7-12 SNAP-CAP Bundle SNAP-CAP Measure SAPG Indicator

22
Conclusions What is a care bundle? – Few elements, each must be “all or none” – Focused on one key point in patient journey How do care bundles work? – Commitment to reliability – Getting the change package right How are bundle elements selected? – Evidence linking care processes to important clinical outcomes – Observational evidence as well as interventional evidence How do you measure bundle implementation? – Run charts – Statistical process control charts What is a driver diagram? – Connects outcomes to culture and change drivers – Connects drivers with measures for improvement ACTPLAN STUDYDO What are we trying to accomplish? How will we know that a change is an improvement? What changes can we make that will result in an improvement?

23
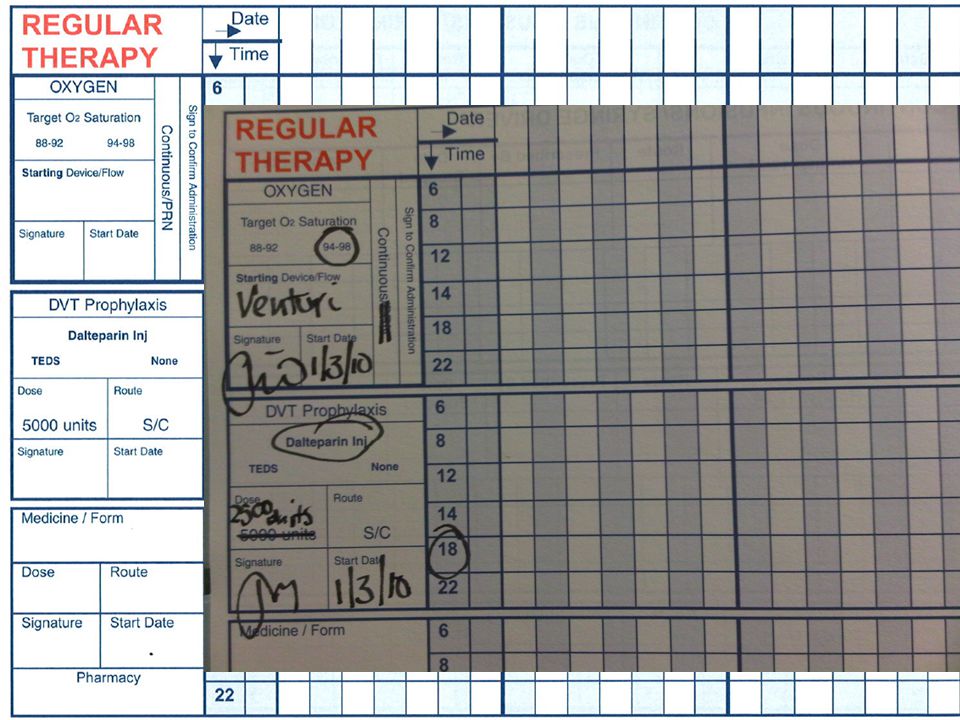
SNAP-CAP Evidence Review Oxygen assessment and appropriate prescribing within 4h (3h?) or oxygen saturations in range? Debatable “all or none” thresholds – Antibiotics within 4h for all CAP patients – Discharge of low risk CURB65 What are the key drivers for change?

Similar presentations








 Consultant Epidemiologist, National.>")




>")








