Download presentation
Presentation is loading. Please wait.

2
Enrollment Reviews – Think Twice David W. Wright

3
No subjects under the age of 18 have been enrolled!!!

5
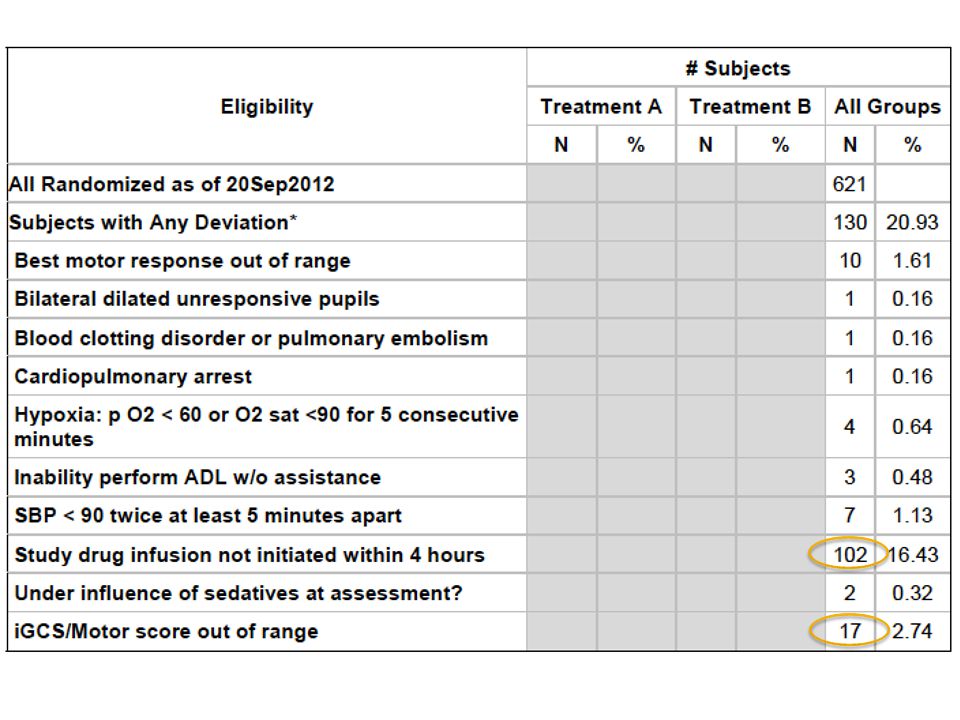
#1 protocol violation (102) Confirm incident time or last know normal Do NOT randomize unless you have at least 20 minutes for pharmacy to mix drug Most are out of our control (pharmacy/OR) Once randomized you should start drug as soon as possible Do not delay starting drug infusion to consent family if they arrive If you don’t have physical documentation (trip sheet) of the time of injury then be diligent about documenting conversations with EMS/Police/Family about time of injury. When monitoring occurs and physical documentation of time of injury differs from what was initially reported verbally, it is still considered a protocol violation

6
Make sure you get a good scene history (if the patient is talking at the scene, they don’t qualify) Get a GCS off sedation shortly before enrollment Alcohol alters mental status! – beware of the GCS 12, ETOH >200

7
TBI must be suspected in order to qualify for the study. For the purpose of this study, the definition of TBI is an alteration in brain function, or other evidence of brain pathology, caused by an external force. It is important to recognize that factors other than TBI may be responsible for alterations in mental state at the time of the injury (e.g. pain, posttraumatic shock, medication, alcohol intoxication/abuse and/or recreational drug use). However, these confounders may be associated with the TBI and must be weighed in light of the history of injury.
. However, these confounders may be associated with the TBI and must be weighed in light of the history of injury..")
9
Scenario 1 20 yo involved in MVC CT negative Head laceration ETOH level 249 combative iGCS E4V1M5 (intubated)
")
10
Is the altered GCS due to alcohol??? Think twice before randomizing a GCS of 11- 12 with ETOH on-board Repeat a GCS just prior to randomizing

11
Scenario 2 40 yo female fell down flight of stairs 2 minute Tonic/clonic seizure enroute to hospital Ativan 2 mg IV given Intubated for airway protection iGCS E1V1M4

12
Is altered GCS due to a post-ictal state? How long did the seizure last? Were benzo’s given that could be affecting GCS?

13
Scenario 3 85 yo ground level fall GCS 4 Cataracts – difficult to see good pupil response Severe edema on CT Neurosurgery will not confirm if will go to OR Family not available Trauma team too busy to discuss

14
What is the pre-injury mRS (functionality)? Co-morbid conditions? Philosophy of treating team/Neurosurgeon? Other injuries? Pupil response? Why did he fall? Is there another issue – like ICH, or MI?

15
Neurosurgery takes to the OR You randomize, but don’t get drug started NS comes out of OR and says, this is not survivable, we just closed him up. Patient unstable, family on the way, NS is going to tell them not survivable DO YOU START THE DRUG?

16
Scenario 4 24 yo M motorcyclist found in ditch on busy highway GCS 7, pupils responsive, no ETOH EMS dispatch was at 01:30 Patient arrived at 0:230

17
Patient in ditch – really visible What is a busy highway? Motorcycle in tree? No witness? Anyone see him before the wreck?

18
Can you find the women and child? The obvious may not be so obvious!

19
If in DOUBT, call the HOTLINE! 1-888-359-2221

Similar presentations