Download presentation
Presentation is loading. Please wait.

1
Nursing Interpretation of the Electrocardiogram (ECG), Telemetry
By: Teresa Champion MCC NURS 2140

2
OBJECTIVES Describe the configuration of the normal electrocardiogram (ECG). Identify and calculate heart rate, rhythm, PR interval, QRS complex, and QT interval for normal and abnormal cardiac rhythms. Discuss the etiology and significant ECG features of the following dysrhythmia classifications: sinus, atrial, junctional, block, ventricular, and asystole. Interpret the significance of each of the dysrhythmias and formulate nursing responsibilities for each dysrhythmia. Identify normal rhythms and dysrythmias. Identify ECG complexes and artifact. Perform ECG rhythm strips. Identify correct dysrythmia terminology

3
Cardiac Conduction System
3 Main Parts: SA node (Sinoatrial node) AV node (Atrialventricla node) HIS-Perkinje System
 AV node (Atrialventricla node) HIS-Perkinje System.")
4
VIDEO OF CONDUCTION SYSTEM
5
Anatomy of the Heart - CARDIAC CELLS
Two types of cardiac cells Myocardial & Pacemaker cells Automaticity Excitability Conductivity Contractility Automaticity- ability of pacemaker to generate their own impulses Excitability – ability of electrical cell to respond to a stimulus Conductivity – the ability of the cardiac cell to accept and transmit a stimulus Contractility – the ability of the cardiac cells to shorten and cause the muscle to contract

6
Anatomy of Heart – Cardiac Chemistry Function
Electrolytes Affecting Cardiac Function Depolarization/Repolarization Cardiac Output (CO): The amount of blood the heart pumps out to body in 1 min. NORMAL: 5 to 8 L CO= HR x SV (CO can be changed by altering heart rate, stroke vol. or both) Stroke Volume = the amount of blood that the heart ejects in one beat which depends on activity level, physical condition, prior heart disease Electrolytes – positive ion charges are cations (Na++, K+, Ca++, also Mg but not as influential). K+, Calcium and Mg – intracellular and sodium is extracellular. Negatively charged cells are anions (Cl – Chloride) and provides electroneuttrility in r/t sodium. Depolarization – contraction . Sodium and potassium move across cell membrane by active transport (ATP pump) or (Na-K pump) Sodium-potassium adenosine triphosphate pump.
: The amount of blood the. heart pumps out to body in 1 min. NORMAL: 5 to 8 L. CO= HR x SV (CO can be changed by altering. heart rate, stroke vol. or both) Stroke Volume = the amount of blood that the. heart ejects in one beat which. depends on activity level, physical. condition, prior heart disease. Electrolytes – positive ion charges are cations (Na++, K+, Ca++, also Mg but not as influential). K+, Calcium and Mg – intracellular and sodium is extracellular. Negatively charged cells are anions (Cl – Chloride) and provides electroneuttrility in r/t sodium. Depolarization – contraction . Sodium and potassium move across cell membrane by active transport (ATP pump) or (Na-K pump) Sodium-potassium adenosine triphosphate pump.")
7
Cardiac Wave Form on Electrocardiogram (ECG)
P wave PR interval QRS complex J point ST Segment T wave QT Interval R to R Interval U wave (not always present)
")
8
ECG Wave Form

9
ECG Lead Placement in Telemetry
1. The white lead is placed on the right side of the chest. This is usually called the “right arm lead.” 2. The black lead is placed on the left side of the chest. This is called the “left arm lead.” 3. The green lead is placed on the right lower abdomen, it is called the “right leg lead.” 4. The red lead is placed on the right lower abdomen, it is called the “left leg lead.” 5. The brown lead is placed slightly to the right of the midsternum, it is called the “V lead or chest lead.” 6. The grey lead is

10
Lead Placement ECG Telemetry
White lead Black Lead Brown Lead Green Lead Red Lead

11
ECG Graph Paper

12
Heart Rate on ECG Heat Rate Fastest count R waves in 6 second strip and times by 10. Count R waves on a full minute strip for accurate HR for irregular rhythms. Another way is to count the number of small boxes between R waves and divide the total by 1500.

13
Heart Rate on ECG 1 big box (5 small boxes) is equal to a HR of 300
2 big boxes is hr of 150 (300/2) 3 big boxes is hr of 100 (300/3) 4 big boxes is hr of 75 (300/4) 5 big boxes is hr of 60 (300/5) 6 big boxes is hr of 50 (300/6) 7 big boxes is hr of 43 (300/7) 8 big boxes is hr of 38 (300/8)
 3 big boxes is hr of 100 (300/3) 4 big boxes is hr of 75 (300/4) 5 big boxes is hr of 60 (300/5) 6 big boxes is hr of 50 (300/6) 7 big boxes is hr of 43 (300/7) 8 big boxes is hr of 38 (300/8)")
14
Large box estimate of heart rate works with regular rhythms

15
A dysrhythmia is a disturbance of the rhythm of the heart caused by a problem in the conduction system. Categorized by site of origin: atria , AV nodal, ventricular Blocks are interruptions in impulse conduction: 1st, 2nd type 1&2, 3rd or complete heart block

16
P wave Measures:

17
QRS WAVE Measures:

18
QT Wave Measures approx seconds

19
NSR: heart rate is 60-100bpm ST: heart rate 101-180 bpm
Heart rates NSR: heart rate is bpm ST: heart rate bpm SB: heart rate <60 bpm

20
PR interval- 0.12-0.20sec QRS-0.06-0.10sec QT segment 0.36-0.44 sec
Sinus rhythm PR interval sec QRS sec QT segment sec Heart rate

21
Atrial arrhythmias Sinus tachycardia Atrial tachycardia
Sinus bradycardia Premature atrial contraction (PAC) Supraventricular tachycardia Atrial fibrillation Atrial flutter
 Supraventricular tachycardia. Atrial fibrillation. Atrial flutter.")
22
Sinus Tachycardia

23
Atrial Tachycardia

24
Sinus Bradycardia

25
Premature Atrial Contraction (PAC)
Premature depolarization of atrial origin P wave may be buried in T wave A pause follows and SA node will start new cycle of sinus beats Indicates atrial irritability No risk if occasional If 6 or more per minute, indicates atrial tachycardia Treat: digitalis, calcium channel blockers, beta blockers

26
SupraVentricular Tachycardia (SVT)
")
27
Atrial Fibrillation (Afib)
Atrial rate > 400 bpm with a varying Ventricular rate Overall rhythm irregular No P waves, unable to measure PR interval QRS=normal: Twave undeterminable Causes: Rheumatic fever, mitral valve stenosis, cad. HTN, MI, hyperthyroidism, COPD, CHF PP. 1091 Concern with A fib is the development of atrial thrombus and loss of atrial kick from ineffective atrial function. Treatment: Ca channel blockers and anti- arrhythmics to convert, beta blockers to < HR, anticoagulants to prevent embolization. Synchronized cardioversion

28
Atrial Flutter

29
Atrial fib/flutter

30
Other Atrial Dysrhymias
Wolf Parkingson-White Syndrome (WPW) Wandering Atrial Pacemaker (WAP) Sick Sinus Syndrome (SSS) Wolf-parkingson white – genetic AV conduction disorder, characterised by two different conduction pathways, produces delta waves (p waves) dips just before the R wave. Wanderind atrial pacemaker – conduction pathways from 3 different sites above the HIS (can include pacemaker site at SA node, AV junction or ectopic atrial sites. Multi-focal p waves. Sick sinus syndrome – impulse generation disorder, pacemaker disorder, conduction disorders, suseptable to paroxymal or chronic atrial tachycardias. Severe damaged sa node from heart disease. Meds
 Wandering Atrial Pacemaker (WAP) Sick Sinus Syndrome (SSS) Wolf-parkingson white – genetic AV conduction disorder, characterised by two different conduction pathways, produces delta waves (p waves) dips just before the R wave. Wanderind atrial pacemaker – conduction pathways from 3 different sites above the HIS (can include pacemaker site at SA node, AV junction or ectopic atrial sites. Multi-focal p waves. Sick sinus syndrome – impulse generation disorder, pacemaker disorder, conduction disorders, suseptable to paroxymal or chronic atrial tachycardias. Severe damaged sa node from heart disease. Meds.")
31
Management of Atrial Dysrhymias
Assess pt response/Monitor Vital Signs May cause drop in Cardiac Output (CO) Notify MD (Health Care Practitioner) Intervention to convert back to NSR Increase rate – slow rates, Administer drugs (Atropine), Transcutaneous Pacing Control rate – if fast Ventricular Response (ie: A-fib, SVT, Aflutter) Anticoagulate Cardioversion
 Notify MD (Health Care Practitioner) Intervention to convert back to NSR. Increase rate – slow rates, Administer drugs (Atropine), Transcutaneous Pacing. Control rate – if fast Ventricular Response. (ie: A-fib, SVT, Aflutter) Anticoagulate. Cardioversion.")
32
How to treat SVT B-blockers ( to decrease conduction thru AV node: Calcium channel blockers ( to decrease conduction thru AV node) Radio frequency ablation SVT converted with Adenosine given rapid IV Push stimulates vagal response.
 Radio frequency ablation. SVT converted with Adenosine given rapid IV Push stimulates vagal response.")
33
Atrial Fibrillation - - 5 to 6 times more likely to have stroke - - atrial rate: 300 to 600 times/minute --prolonged A-Fib may stretch & weaken heart muscle - - symptoms: lightheaded, very tired, SOB, diaphoretic, chest pain,

34
A Fib electrical cardioversion:
High risk of forming clots & causing stroke Anticoagulants taken before treatment and 3-4 weeks post treatment If life-threatening, may need Heparin IV before cardioversion Best time: recent A fib

35
Ventricular arrythmias
Junctional rhythms AV blocks Premature ventricular contraction (PVC) Ventricular Tachycardia (V-tach) Ventricular Fibrillation (V-Fib) Torsade de Pointes (TdP) Pulseless electrical activity (PEA) Asystole
 Ventricular Tachycardia (V-tach) Ventricular Fibrillation (V-Fib) Torsade de Pointes (TdP) Pulseless electrical activity (PEA) Asystole.")
36
Junctional Escape Rhythm

37
Accelerated Junctional Rhythm

38
AV Blocks First degree block Second degree block Type I (Wenchebach)
Second degree block Type II (Mobitz II) Third degree block Bundle branch block
 Third degree block. Bundle branch block.")
39
First degree heart block
AV node delays the impulse from the SA node for abnormal length of timeDocument the dysrhythmia Monitor for progression to slower heart rate or worsening block If progression noted, monitor pt, notify physician Causes: CAD, MI, drugs that act on AV node (digitalis) Characteristics: PR interval >0.20 seconds Not serious but may progress to 2nd degre Rate is usually WNL Rhythm is regular Pwaves are normal in size and shape The PR interval is prolonged (>0.20 sec) but constant
 Characteristics: PR interval >0.20 seconds. Not serious but may progress to 2nd degre. Rate is usually WNL. Rhythm is regular. Pwaves are normal in size and shape. The PR interval is prolonged (>0.20 sec) but constant.")
40
Second degree heart block type 1 (Mobitz I or Wenchebach)
Pwaves are normal in size and shape; Some pwaves are not followed by QRS PR interval: lengthens with each cycle until it appears without QRS Complex then the cycle starts over QRS is usually narrow RISK: often a temporary block after MI May progress to complete(3rd degree)block TREATMENT: freq. none needed slow vent rate: ATROPINE will increase AV conduction EPINEPHRINE To increase rate of SA node AV node delays progression of SA node impulse for longer than normal Some of the SA impulses never reach ventricles P waves regular Progressive lengthening of PR interval until one P wave is not conducted CAUSE: ischemia or injury to AV node
block. TREATMENT: freq. none needed. slow vent rate: ATROPINE will increase AV conduction. EPINEPHRINE To increase rate of SA node. AV node delays progression of SA node impulse for longer than normal. Some of the SA impulses never reach ventricles. P waves regular. Progressive lengthening of PR interval until one P wave is not conducted. CAUSE: ischemia or injury to AV node.")
42
Second degree heart block type 2 (Mobitz II)
Ventricular rate is usually slow Rhythm is irregular Pwaves are normal in size and shape (more pwaves than QRS) PR interval is within normal limits QRS is usually wide RISK: unpredictable & may suddenly advance to complete hrt block Especially common after inferior infarction A DANGEROUS WARNING DYSRHYTHMIA TREATMENT: if vent rate slow, atropine or epinephrine may need temporary pacer Determine width of QRS WATCH for widening QRS complex *width of QRS indicates location in the conduction system of the block the wider the complex, the lower in the bundle branch system the block will be. IF QRS WIDENS, NOTIFY PHYSICIAN IMMEDIATELY. Prepare for insertion of pacer Assess vitalsAtrial rate 60 to 100 More P waves than QRS complexes Ventricular response 2:1 or 3:1 No change in PR intervals of conducted P waves CAUSES: disease of AV node, AV junctional tissue, or His-Purkinje system, inferior MI
 PR interval is within normal limits. QRS is usually wide. RISK: unpredictable & may suddenly advance to complete hrt block. Especially common after inferior infarction. A DANGEROUS WARNING DYSRHYTHMIA. TREATMENT: if vent rate slow, atropine or epinephrine. may need temporary pacer. Determine width of QRS. WATCH for widening QRS complex. *width of QRS indicates location in the conduction system of the block. the wider the complex, the lower in the bundle branch system the block will be. IF QRS WIDENS, NOTIFY PHYSICIAN IMMEDIATELY. Prepare for insertion of pacer. Assess vitalsAtrial rate 60 to 100. More P waves than QRS complexes. Ventricular response 2:1 or 3:1. No change in PR intervals of conducted P waves. CAUSES: disease of AV node, AV junctional tissue, or His-Purkinje system, inferior MI.")
43
3rd degree heart block or complete heart block
More atrial waves than ventricular No conduction of atrial impulses Atrial/ventricles beat independently RISKS: bradycardia which produces a decrease in CO leading to hypotension & myocardial ischemia TREATMENT; pacer NURSING INTERVENTION; monitor , hemodynamics , prepare for pacer Ventricular rate is regular but there is no correlation between p-waves and QRS P waves are normal in size and shape No true PR interval

44
Premature ventricular conduction (PVC)
uniform=go the same direction multifocal= go in different direction R on T=when the pvc fall on the preceding twave couplet= 2 pvcs together bigeminy= pvc every other beat trigeminy=pvc every third beat

45
PVC Unifocal Multifocal

46
PVC: ventricular origin
Complex is wide followed by compensatory pause An irritable focus in ventricle initiates a contraction before normally expected beat. Acute MI most common cause QRS is wide and bizarre Risks: increasing myocardial irritability, leading to increased freq. of PVCs Can occur as bigeminy (every other beat) or short runs
 or short runs.")
47
Ventricular tachycardia
Monomorphic: beats are same size and shape Polymorphic: different size and shape

48
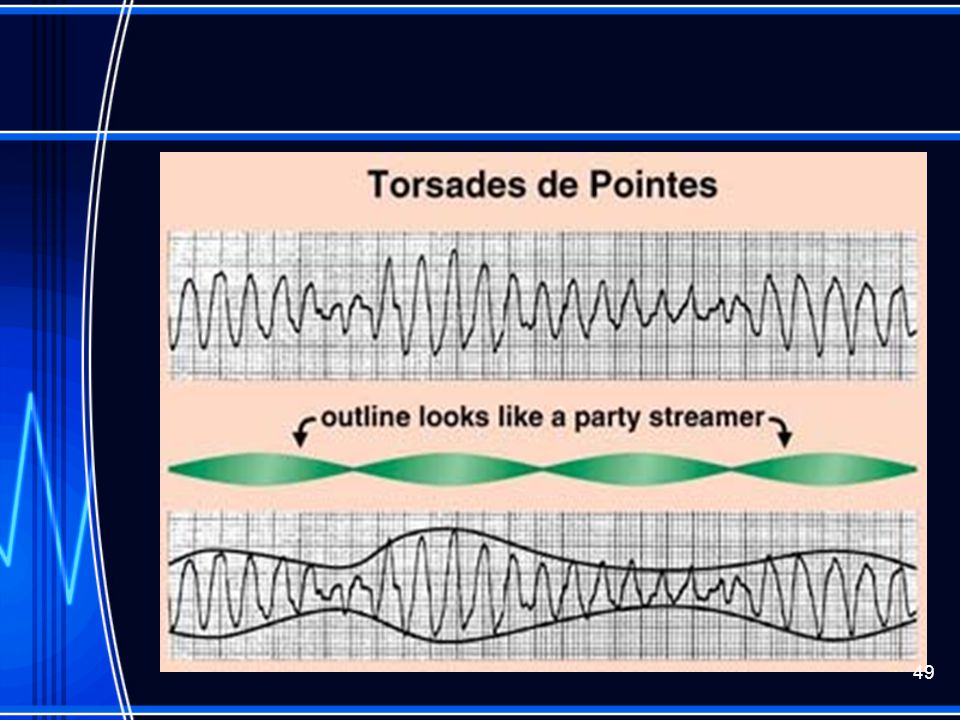
Torsades de pointe This is a polymorphic VT
Usually electrical imbalance in r/t NA+ or K+

50
V-tach Advanced irritability of ventricles due to ASHD, CHF, acute MI electrolyte imbalance. Hypoxia, acidosis, occasionally drugs RISKS: low to no Cardiac output Nursing Interventions: monitor, if pt unconscious, immediately defibrillate

51
Torsade de pointes Will see prolonged QT interval when in sinus rhythm
Will see prominent U wave If lasts >10 seconds pt will progress to unconsciousness, life threatening with ineffective cardiac output TREATMENT: IV magnesium

52
Ventricular Fibrillation (Course)
Rate can not be determined because of no identifiable waves Rapid chaotic rhythm with no pattern No p waves No PR interval No QRS

53
Ventricular Fibrillation (Fine)
")
54
Vtach/Vfib Both can be life threatening VT= V HR 100-250 bpm
Causes: AMI, CAD, hypokalemia, dig toxic S/S: palpitations, dizzy, angina, <LOC Treatment: assess for pulse, if none, defibrillate VF=Rate undeterminable Cause: same Treatment: CPR, Defibrillate

55
V-fib May occur after MI Extensive ventricular irritability
Very little or no cardiac output (No Pulse) Death within 4 to 8 minutes TREATMENT: immediate defibrillation immediate defibrillation at 200 J (100J) if unsuccessful, repeat at 300 J (150J) If unsuccessful, repeat at 360 J (200J) CPR If do not know type of defibrillator start at 200J
 Death within 4 to 8 minutes. TREATMENT: immediate defibrillation. immediate defibrillation at 200 J (100J) if unsuccessful, repeat at 300 J (150J) If unsuccessful, repeat at 360 J (200J) CPR. If do not know type of defibrillator start at 200J.")
56
Asystole

57
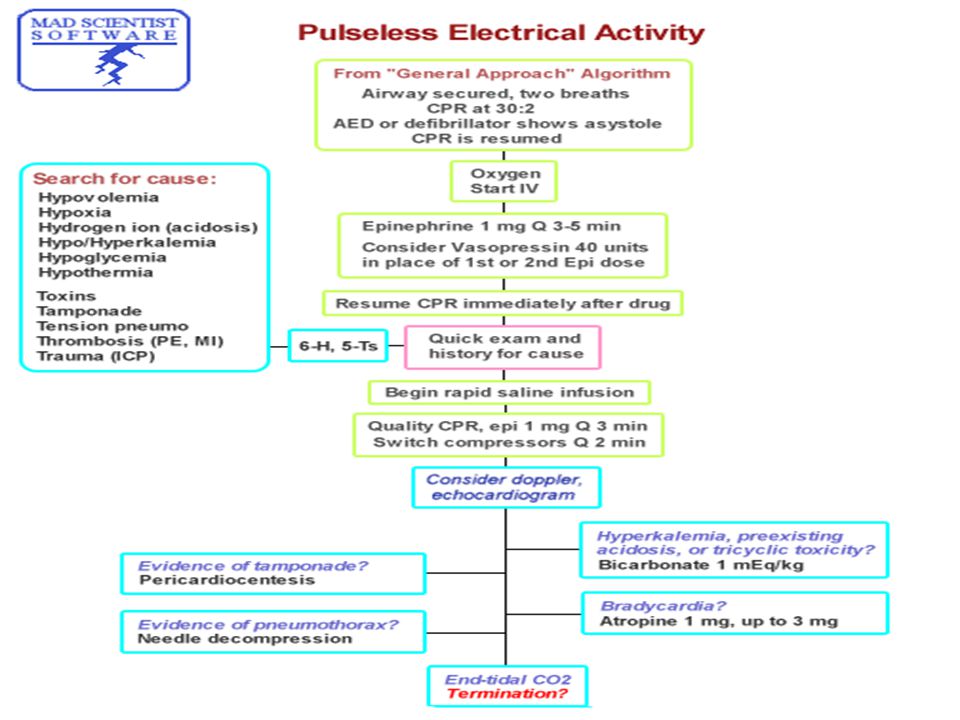
Pulsless Electrical Activity (PEA)
")
58
Asystole and PEA CPR Oxygen
Epinephrine 1 mg IV/IO (repeat 3-5 minutes) May give Vasopressin 40U IV/IO to replace 1st or 2nd dose of epinephrine Consider Atropine 1 mg IV/IO Repeat every 3 to 5 min (up to 3 doses)
 May give Vasopressin 40U IV/IO to replace. 1st or 2nd dose of epinephrine. Consider Atropine 1 mg IV/IO Repeat every 3 to 5 min (up to 3 doses)")
59
Paced beat Pacer spike should fall before the P wave unless a dual
Chamber pacemaker; if it does not there could be a problem

60
ARTIFACT

Similar presentations