Download presentation
Presentation is loading. Please wait.

1
GI TRACT SURGICAL PATHOLOGY Dr Rasti

2
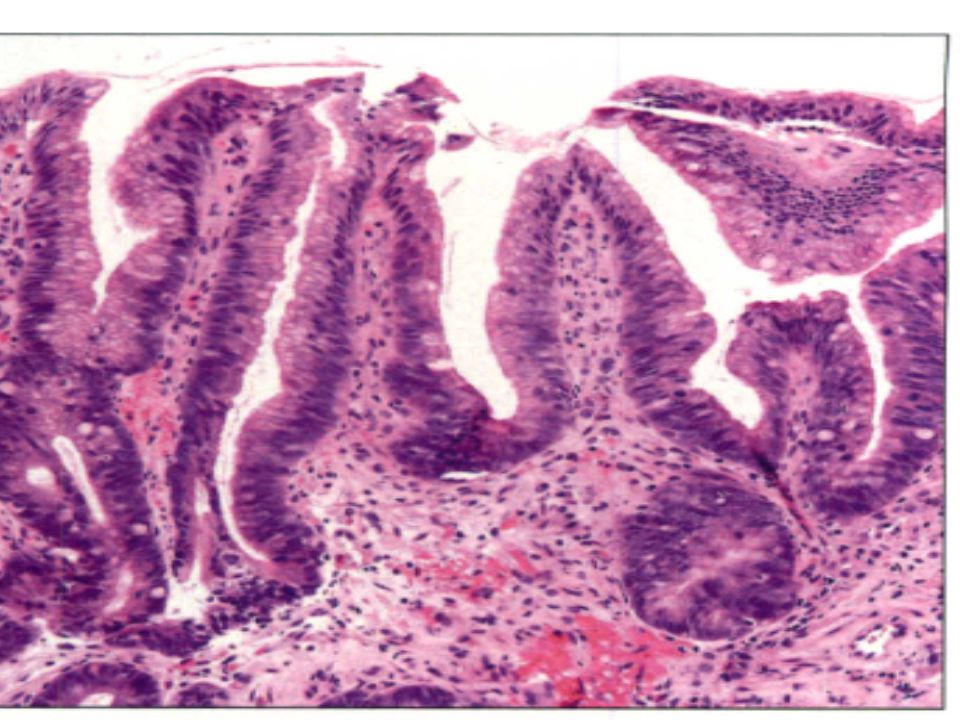
Case 1:lower esopahgus mucosal biopsy (tubular esophagus )
")
4
What is diagosis: 1)Fundal glands intestinal aplasia 2)Barrets esophagus without dysplasia 3)Barrets esophus with low gade dysplasia
Fundal glands intestinal aplasia 2)Barrets esophagus without dysplasia 3)Barrets esophus with low gade dysplasia")
5
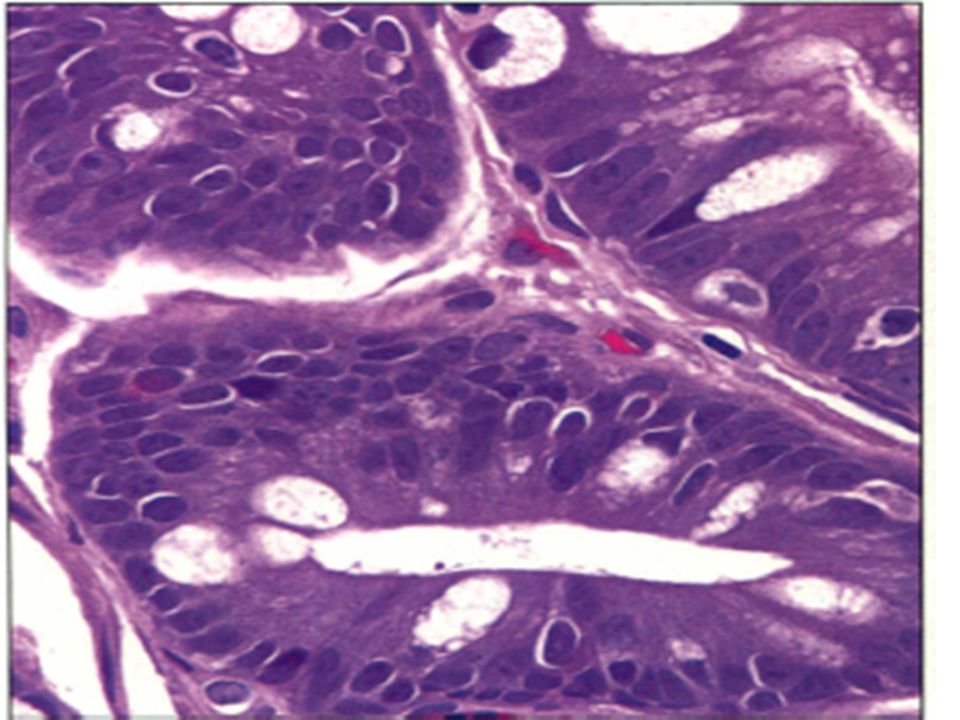
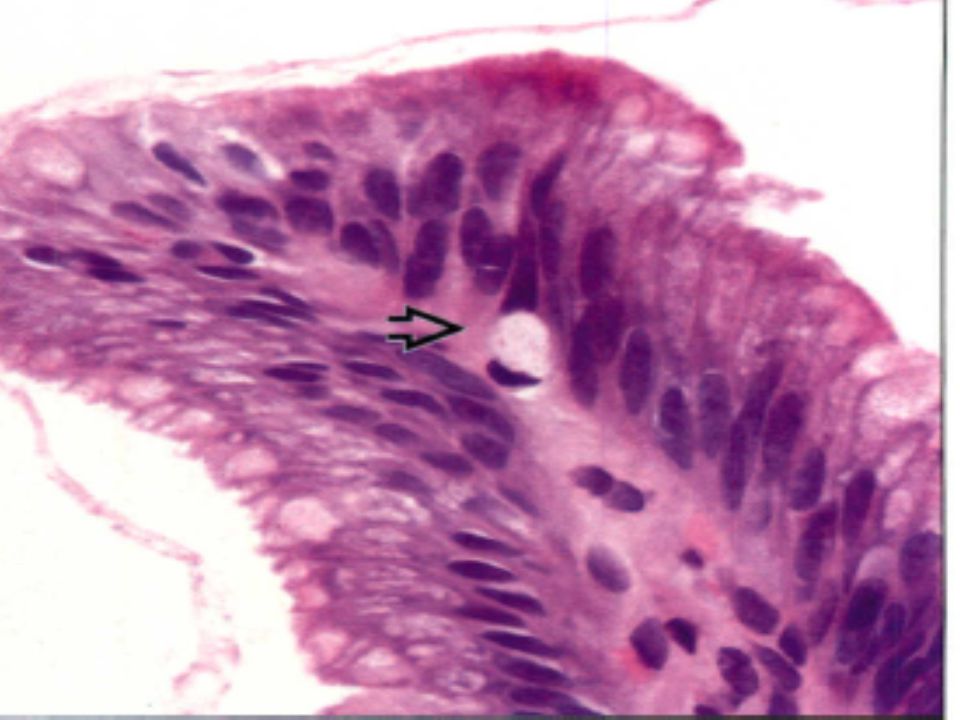
Hematoxylin & eosin shows the deeper portions of glands found in Barrett mucosa. These display some nuclear changes that can be overinterpreted as dysplasia on tangentially embedded samples. Note the prominent goblet cells.

6
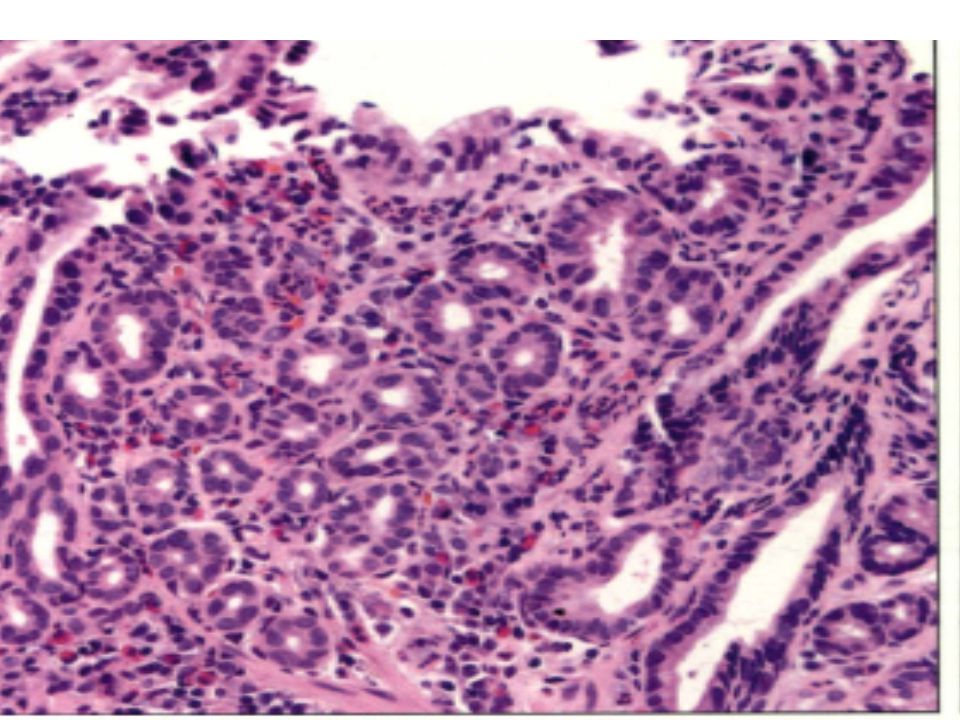
Case 2 lower :esopahgus mucosa

9
Hematoxylin & eosin of mucosa displays features of both squamous and columnar mucosa, which has been termed "multilayered epithelium." It demonstrates mucin profiles like to those of Barrett mucosa. (

10
Lower esophagus mucosa Endoscopic findings are consist with Barret’s esophagus

13
Diagnosis: 1)Barrets with low grade dysplasia 2)barrets IFD 3)Barrets mucosa without dysplasia 4)Regnerative changes
Barrets with low grade dysplasia 2)barrets IFD 3)Barrets mucosa without dysplasia 4)Regnerative changes")
14
These may be reactive (neutrophils in the adjacent squamous mucosa), but the nuclei are hyperchromatic. This might be regarded as IFD by some observers but reactive by others.

16
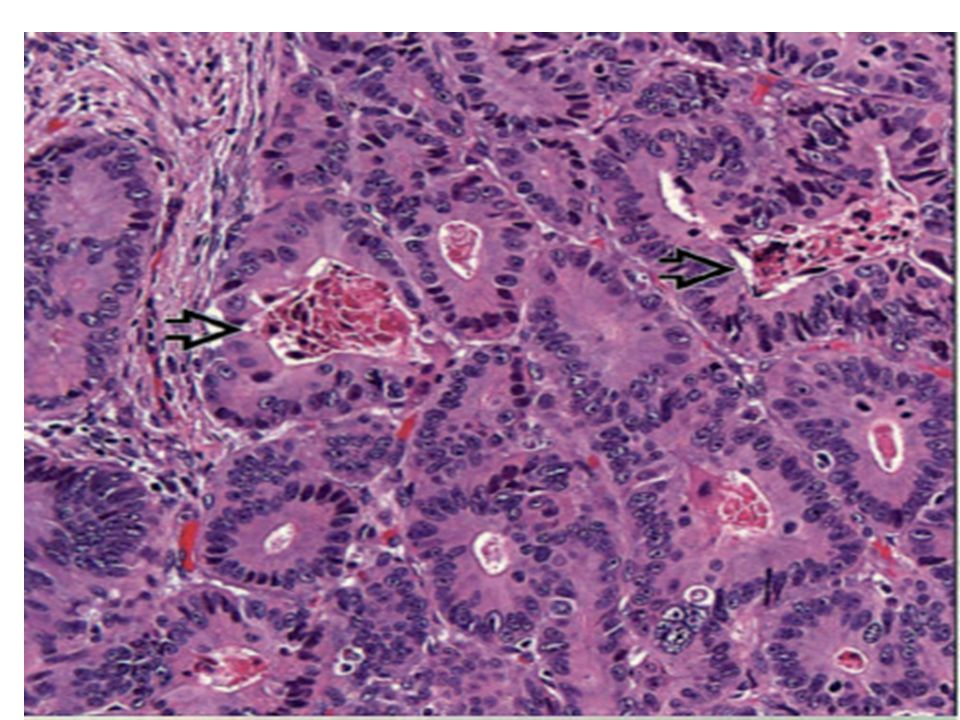
Lower esophagus 1)low garde dysplasia 2)High garde dysplasia 3)IFD
low garde dysplasia 2)High garde dysplasia 3)IFD")
17
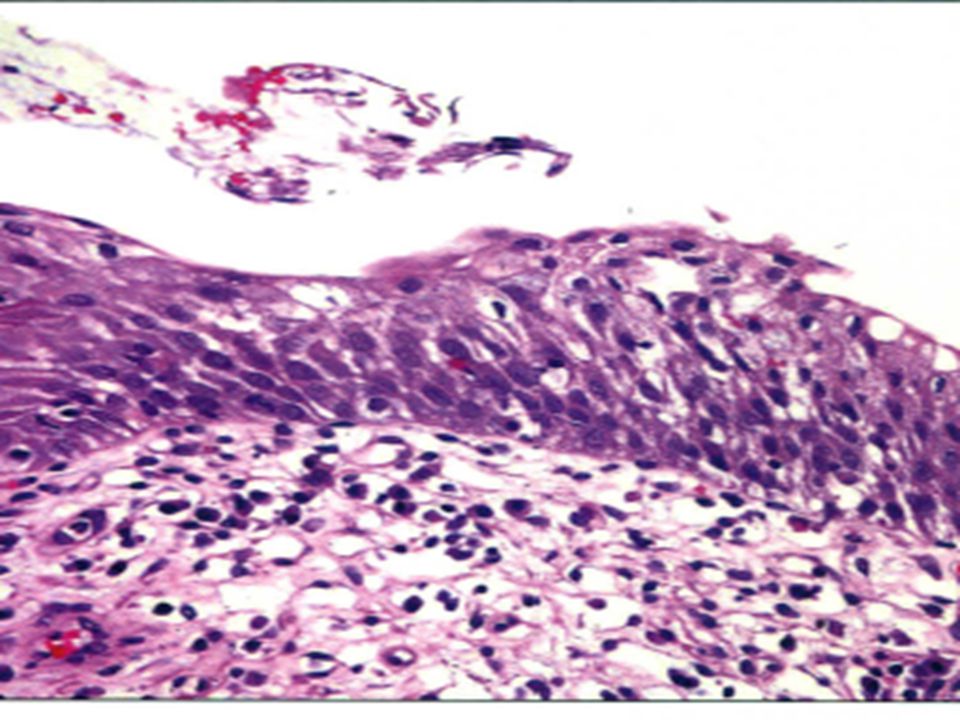
Hematoxylin & eosin shows the architectural appearance of LGD. There is poor surface maturation, but nuclei remain aligned with their long axes perpendicular to the basement membrane (maintained nuclear polarity).
..")
18
Lower esophagus 1)low garde dysplasia 2)High garde dysplasia 3)IFD
low garde dysplasia 2)High garde dysplasia 3)IFD")
20
Hematoxylin & eosin shows LGD at the surface in, Notice the size and chromatin density of the nuclei. These are larger and darker. The inverted goblet cell

21
Lower esophagus 1)low garde dysplasia 2)High garde dysplasia 3)IFD
low garde dysplasia 2)High garde dysplasia 3)IFD")
23
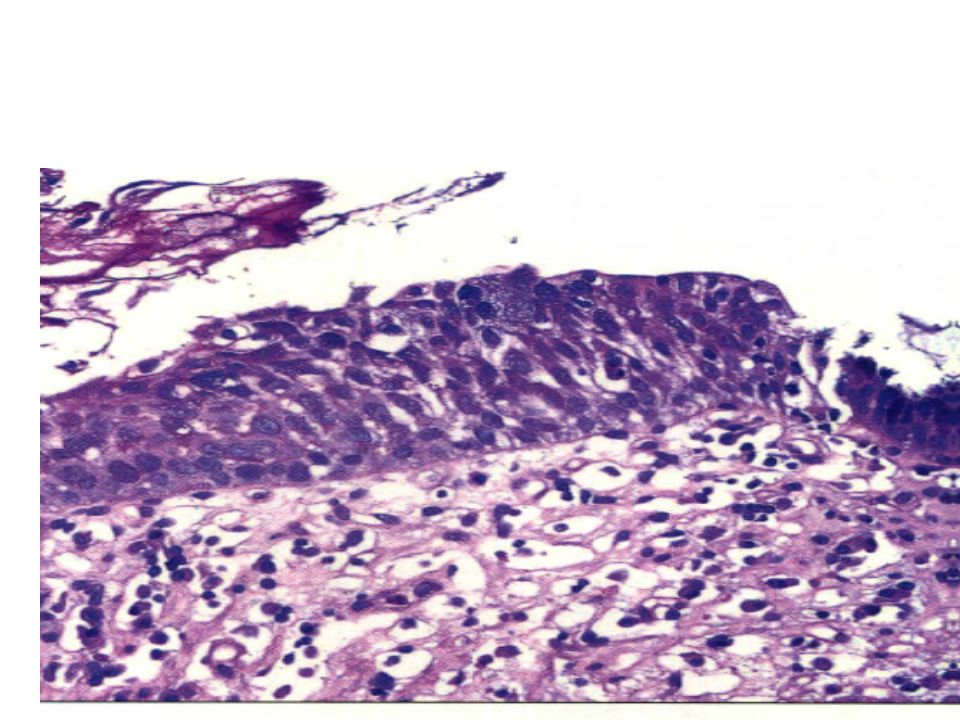
Hematoxylin & eosin high-grade dysplasia shows hyperchromatic glands that are crowded, and there are several markedly enlarged nuclei~. There is no surface maturation, and nuclear polarity is lost at the surface.

24
Lower esophagus 1)low garde dysplasia 2)High garde dysplasia 3)IFD
low garde dysplasia 2)High garde dysplasia 3)IFD")
26
The glands are dysplastic and composed of tiny hyperchromatic cells. This "small cell" pattern is unrelated to endocrine differentiation. There is also prominent inflammation; a subset of HCD cases display prominent inflammation. In such cases, labeling with p53 can be helpful.

27
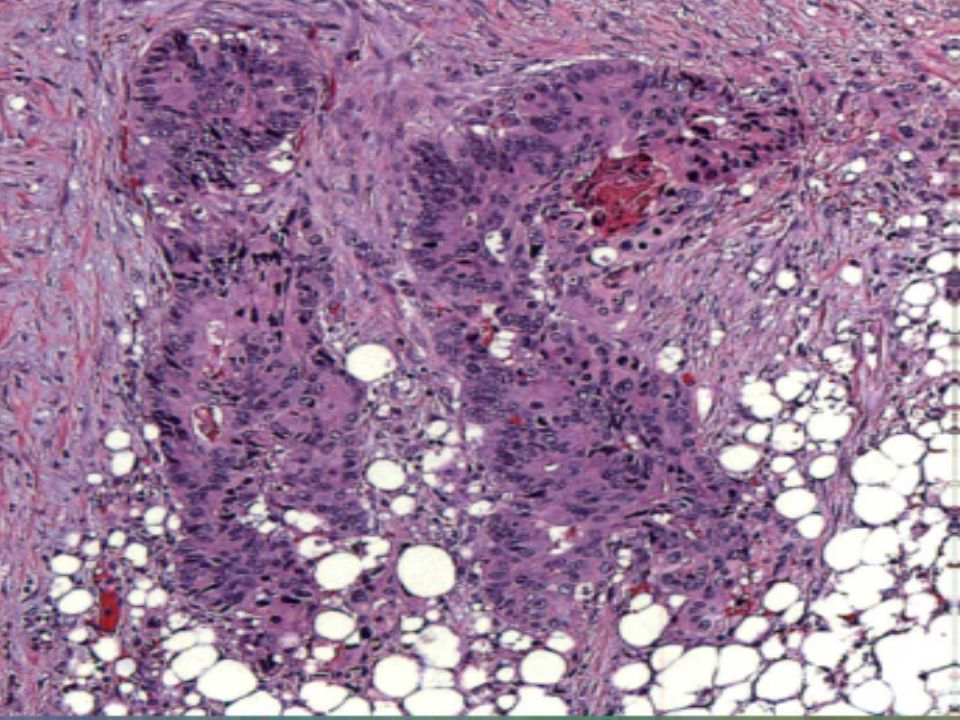
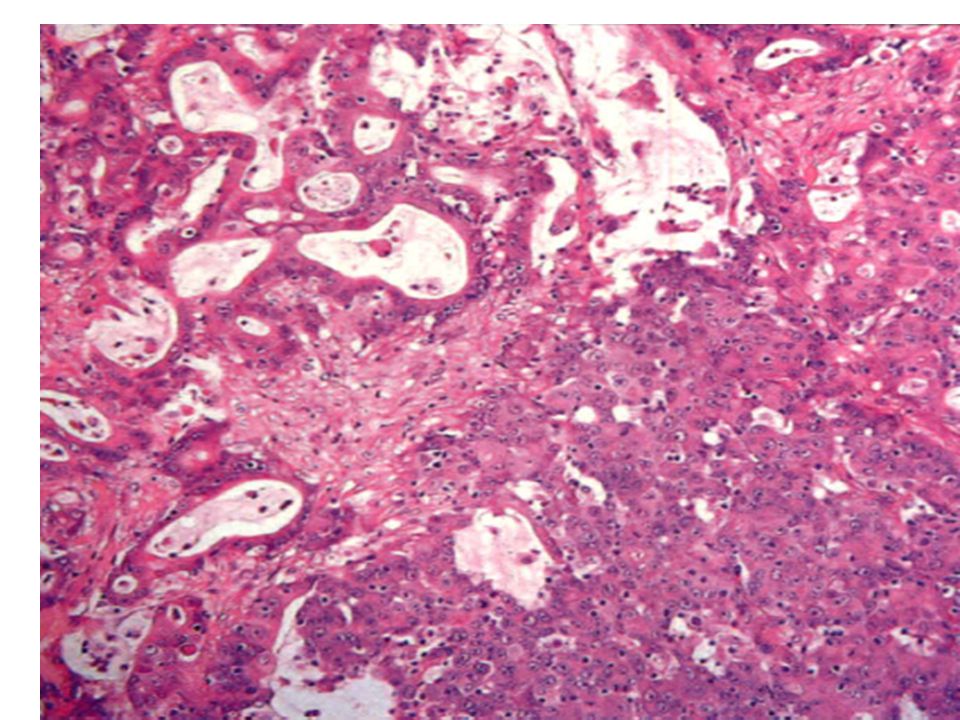
COLORECTALCARCINOMA CRC

29
Hematoxylin & eosin shows a low-power view of moderately differentiated microsatellite stable colorectal adenocarcinoma with dirty or garland necrosis ~

31
Hematoxylin & eosin highpower view shows infiltrative growth pattern and lack of host response, 2 findings more typical of microsate/lite stable tumors than of unstable tumors.

37
poorly differentiated MSI-H colorectal carcinoma with large numbers of tumor infiltrating lymphocytes ~. MSI-H colorectal carcinoma with histologic heterogeneity. mucinous differentiation, poorly differentiated tumor with increased numbers of tumor infiltrating lymphocytes.

38
Molecular Genetics · 85-88% of CRCs are microsatellite stable (MSS)tumors, many arise via mutations in Wnt signaling pathway o Adenoma-carcinoma sequence · ·12-15% of CRCs are microsatellite unstable (MSIH) tumors that arise due to errors in DNA mismatch repair o Serrated pathway: Sessile serrated adenomas give rise to sporadic MSI-H cancers · Methylation of hMLHl key molecular event · Often have BRAF mutation o 10% of MSI-H tumors arise via germline mutations in mismatch repair genes (Lynch syndrome/HNPCC) · serrated lesions) · Lynch tumors are thought to grow much faster o MSI-H tumors have better prognosis than MSS tumors (stage for stage)
tumors, many arise via mutations in Wnt signaling pathway o Adenoma-carcinoma sequence · ·12-15% of CRCs are microsatellite unstable (MSIH) tumors that arise due to errors in DNA mismatch repair o Serrated pathway: Sessile serrated adenomas give rise to sporadic MSI-H cancers · Methylation of hMLHl key molecular event · Often have BRAF mutation o 10% of MSI-H tumors arise via germline mutations in mismatch repair genes (Lynch syndrome/HNPCC) · serrated lesions) · Lynch tumors are thought to grow much faster o MSI-H tumors have better prognosis than MSS tumors (stage for stage)")
39
Microsatellite instability (MSI) is the condition of genetic hypermutability that results from impaired DNA Mismatch Repair (MMR). In other words, MSI is the phenotypic evidence that MMR isn't functioning normally. DNA MMR corrects errors that spontaneously occur during DNA replication like single base mismatches or short insertions and deletions. The proteins involved in MMR form a complex that binds to the mismatch, identifies the correct strand of DNA, then subsequently excises the error and repairs the mismatch. [ [

40
Cells with abnormally functioning MMR tend to accumulate errors rather than correcting those errors. As a result, gene sequences are not preserved faithfully through DNA replication, and novel Microsatellites fragments are created. Microsatellite instability is detected by PCR based assays that reveal these novel microsatellites. Microsatellites

42
COLOSCOPIC BIOPSY

48
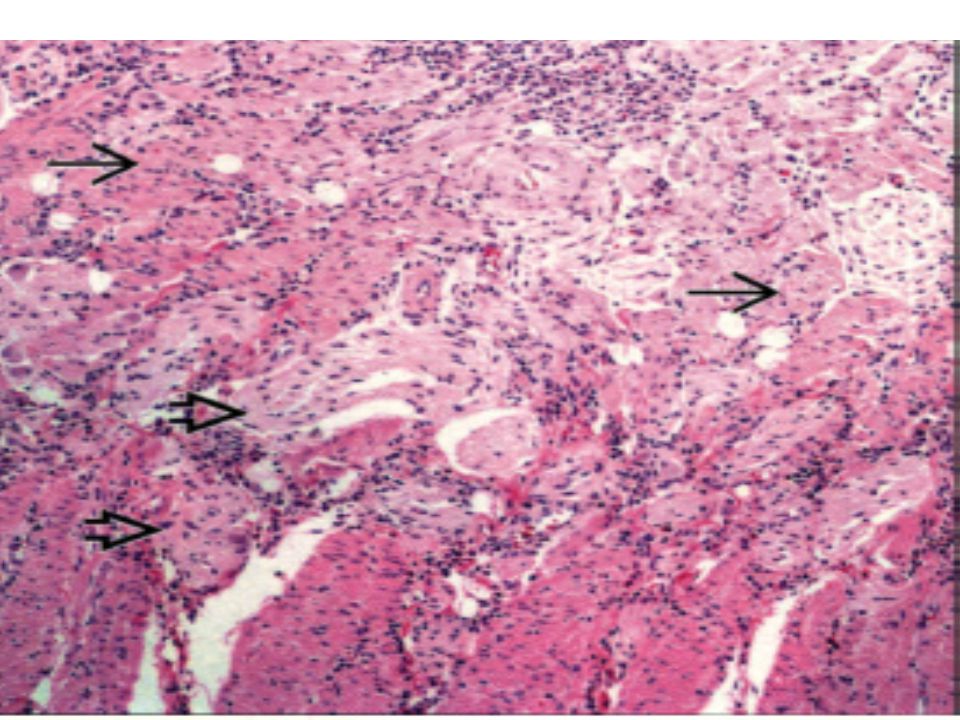
Microscopic Pathology. Basal lymphoplasmacytosis, crypt branching/dropout ·Crypt abscesses, polypoid granulation tissue ·Paneth cell and pseudopyloric gland metaplasia ·Fissuring ulcers to muscularis propria ·.Transmural lymphoid aggregates Submucosal fibrosis, muscle and nerve hypertrophy · Large, well-formed epithelioid cell granulomas o Mostly in submucosa, subserosa;

49
DIFFERENTIAL DIAGNOSIS Ulcerative Colitis · Diffuse, primarily mucosal involvement of colorectum ·Absence of skip lesions (unless treated), transmural inflammation (except near ulcer), granulomas (except due to foreign body or crypt-rupture), upper GI/ileal disease (except nonspecific duodenitis, pediatric UC) · "Backwash" ileitis : Only seen in severe right-sided UC o No severe activity or chronic inflammatory changes Indeterminate Colitis (lC) ·Not a specific disease entity: No diagnostic criteria o Impossible to distinguish CD vs. UC (5-15% of IBD) o Overlapping features of both CD, UC (resections) ·Used by some if insufficient clinical, histologic data o Instead: "Active chronic (ileo)colitis, type unknown" o 80% of IC: Underlying IBD type eventually apparent 5
 o Overlapping features of both CD, UC (resections) ·Used by some if insufficient clinical, histologic data o Instead: Active chronic (ileo)colitis, type unknown o 80% of IC: Underlying IBD type eventually apparent 5.")
51
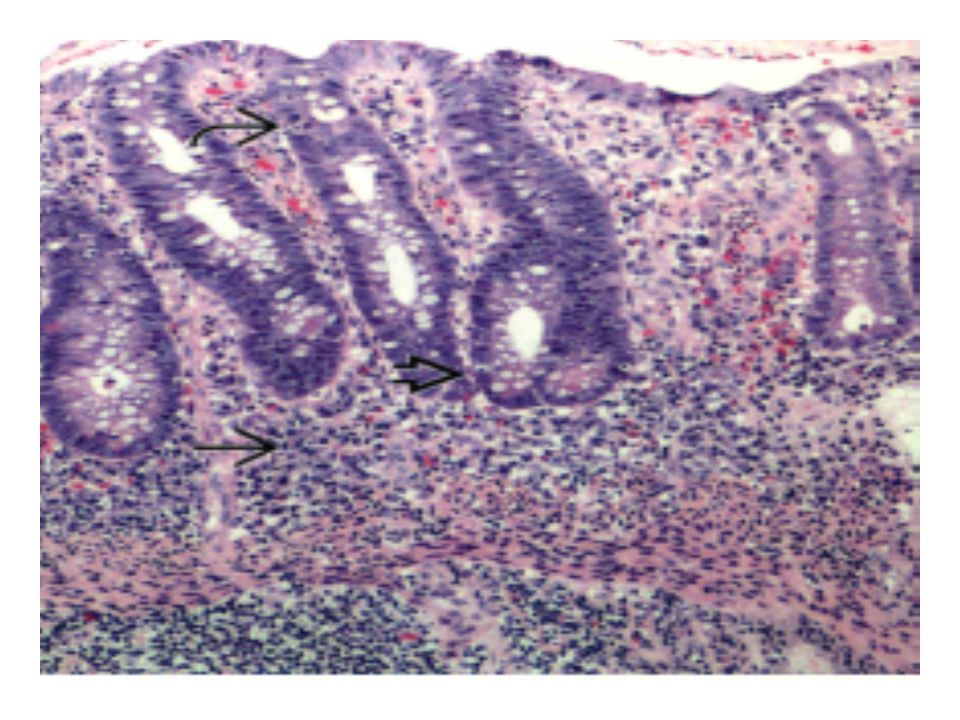
WHAT IS YOUR DIAGNOSIS?

52
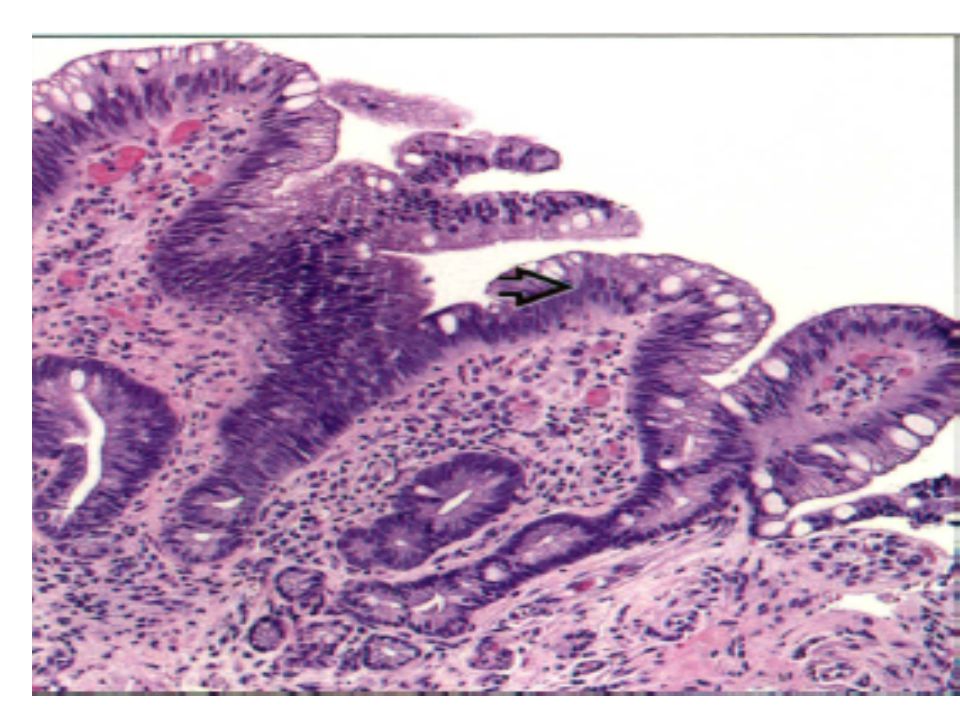
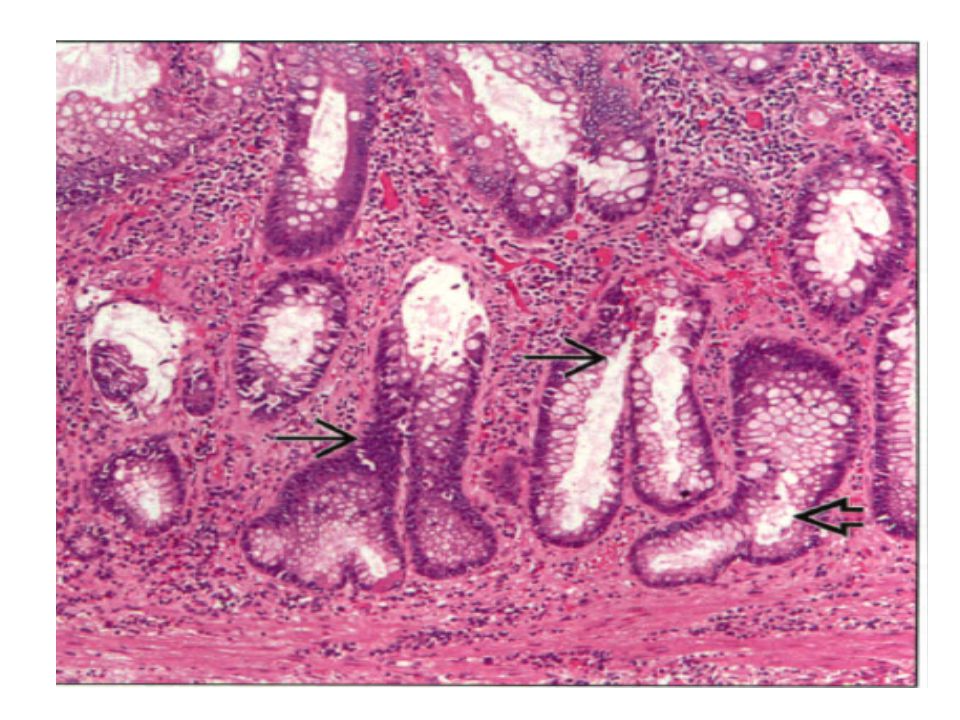
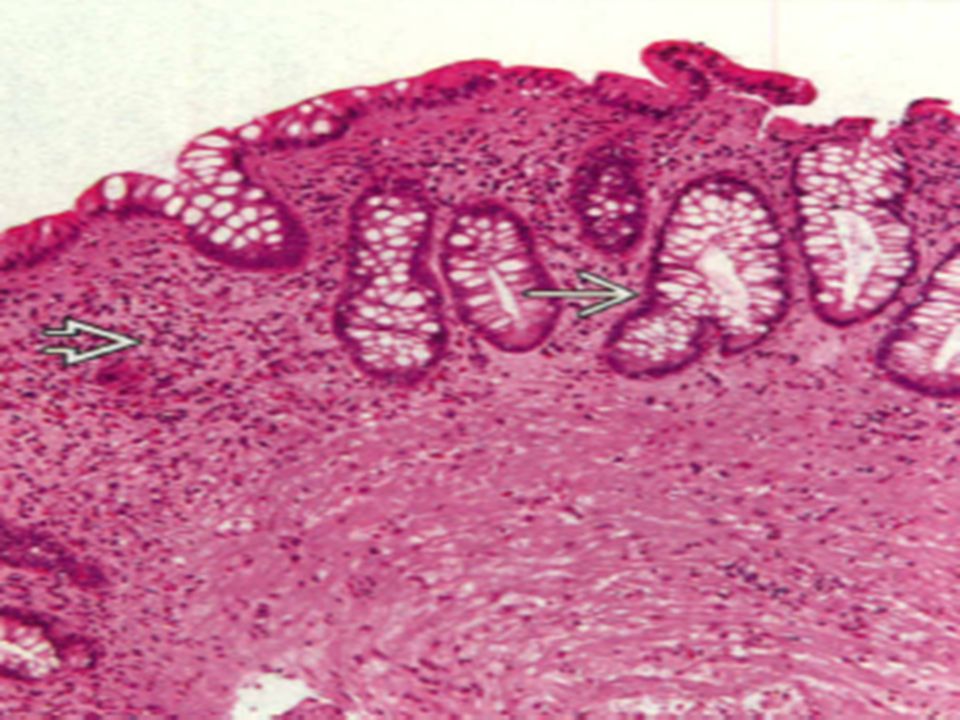
Hematoxylin & eosin shows architectural distortion of the mucosa, indicative of chronic injury. Several abnormally shaped ~ and branched ~ crypts are visible.

54
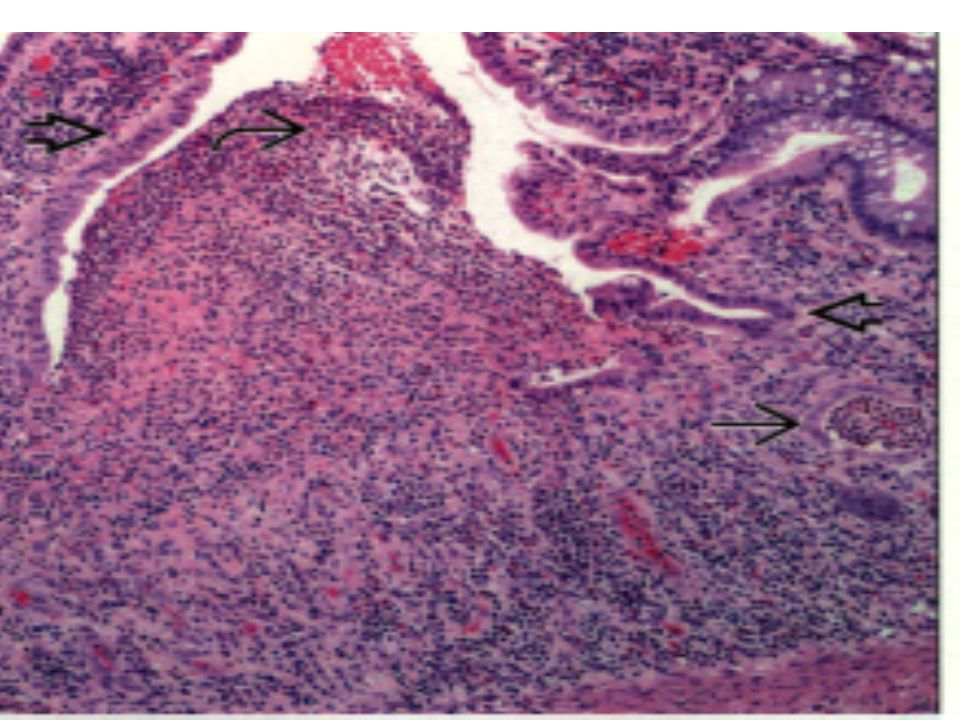
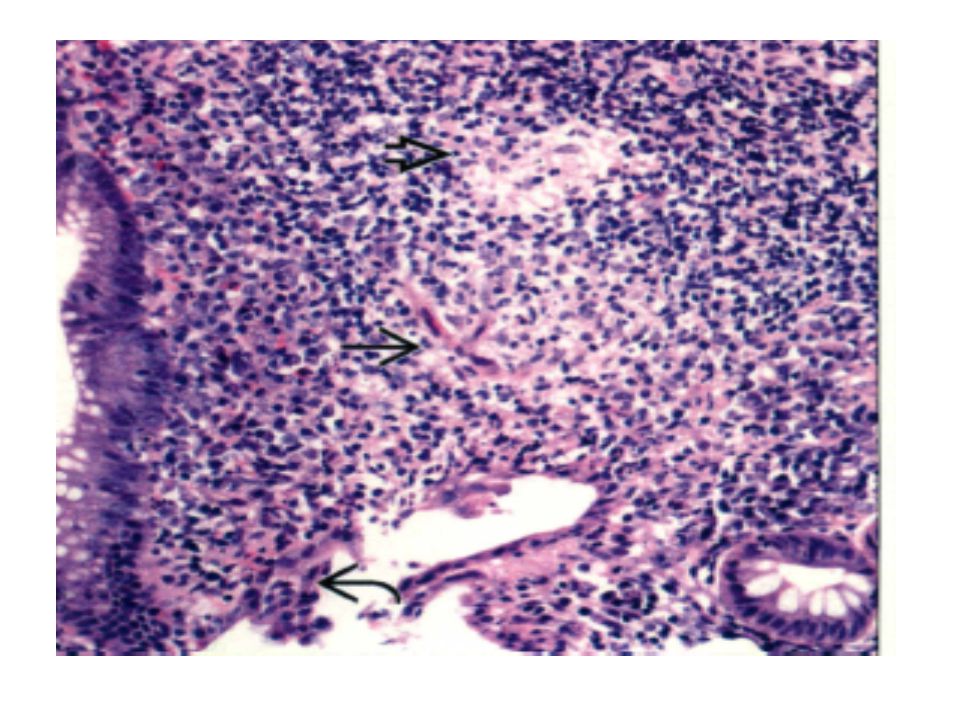
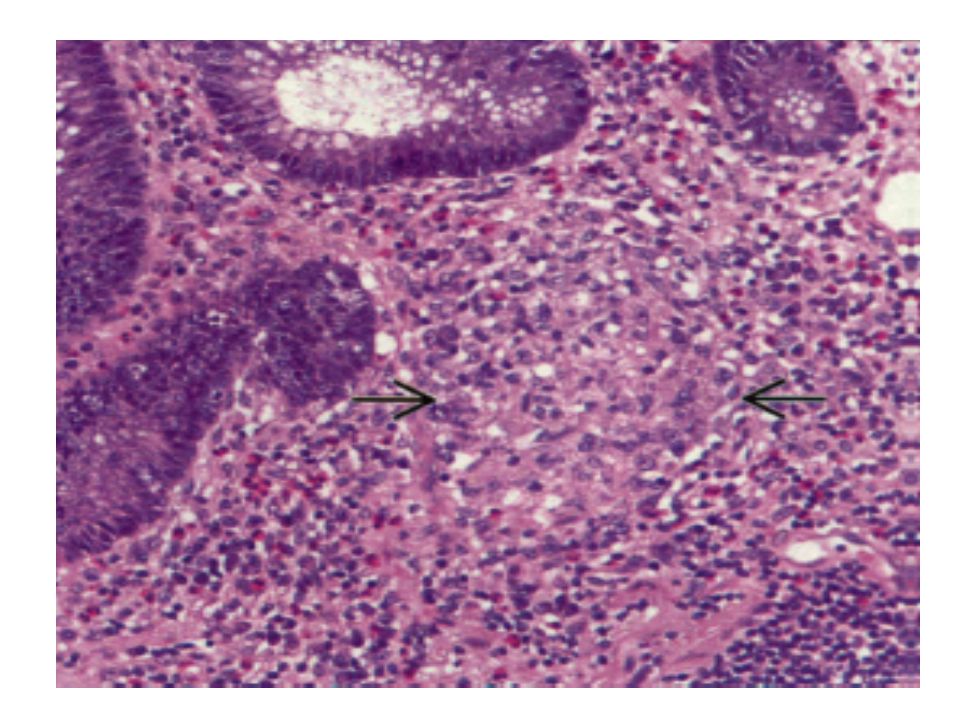
Hematoxylin & eosin shows clustered epithelioid histiocytes ~ resembling a granuloma in the lamina propria. Such "crypt rupture granulomas" are common in areas of ongoing or recent crypt injury and are not specific to Crohn disease.

56
Hematoxylin & eosin shows quiescent chronic colitis. Note the lack of acute inflammation and sparse chronic inflammation. Crypt distortion = and areas devoid of crypts.

59
Collagenous colitis –Microscopic Pathology · –Patchy subepithelial increased collagen –o Most reliable biopsies from transverse colon –Irregular collagen band extends entraps capillaries, –inflammatory cells, and fibroblast nuclei –· Increased intra epithelial lymphocytes (IELs) –o > 10-20 IELs/lOO surface epithelial cells ·Chronic or mixed inflammation in lamina propria –Increased eosinophils (may be marked) ·Detachment of surface epithelial cells from collagen –band ·Normal crypt size and shape; rare distortion
 –o > IELs/lOO surface epithelial cells ·Chronic or mixed inflammation in lamina propria –Increased eosinophils (may be marked) ·Detachment of surface epithelial cells from collagen –band ·Normal crypt size and shape; rare distortion")
60
Diff diagnosis CC · Lymphocytic colitis o No increased subepithelial collagen · Inflammatory bowel disease o Erosion/ulceration, crypt architectural distortion, basal plasmacytosis ·Amyloidosis o Stains with Congo red, not trichrome o Tangential sectioning · Ischemic/radiation colitis o No t intraepithelial or lamina propria lymphocytes · Entities mimicking thickened collagen o Tangential sectioning of tissue, hyperplastic polyp

62
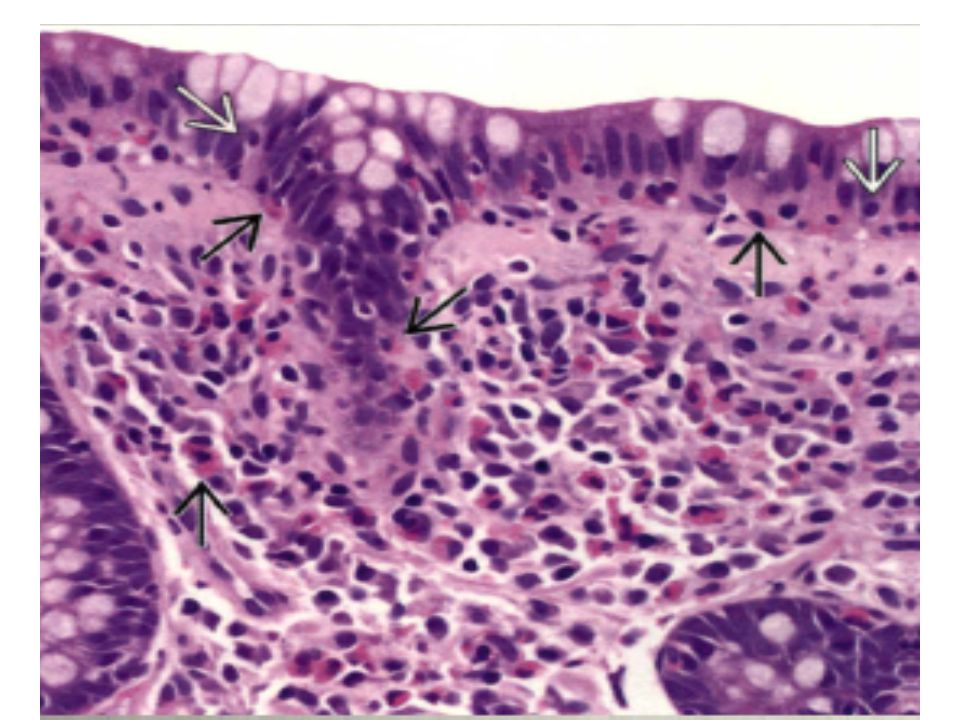
Hematoxylin & eosin shows increased Intraepithelial lymphocytes = and subepithelial collagen and infiltration of surface epithelium and lamina propria by eosinophils ~, not typically seen to this extent in lymphocytic colitis.

64
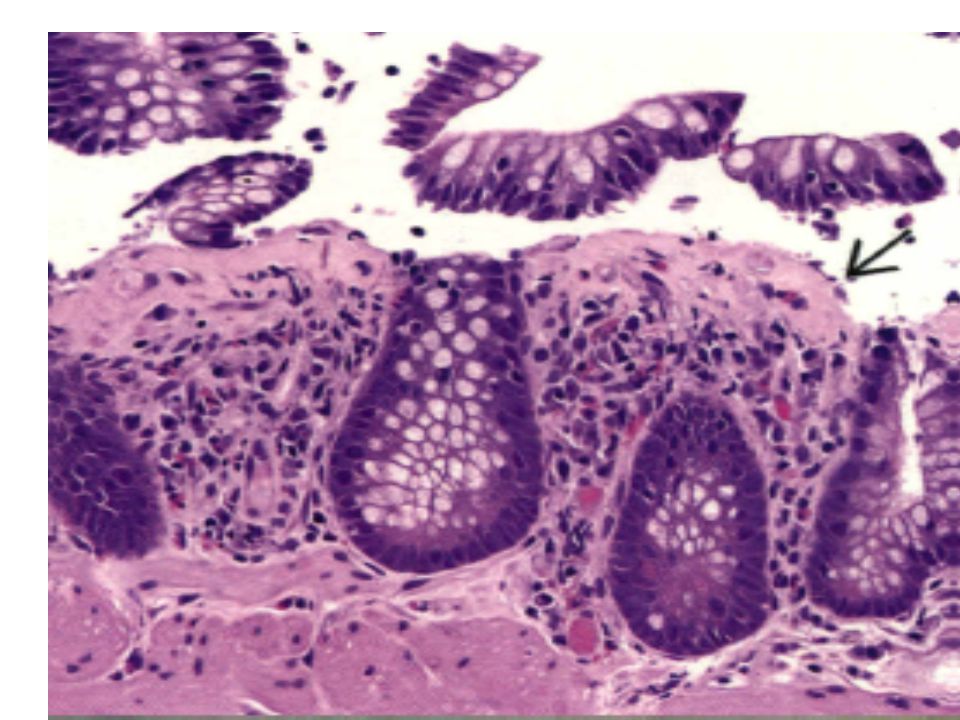
COLLAGENOUS COLITIS Hematoxylin & eosin shows sloughing of surface epithelium from the subepithelial collagen band~, increased chronic inflammation in the lamina propria, and normal crypt architecture.

66
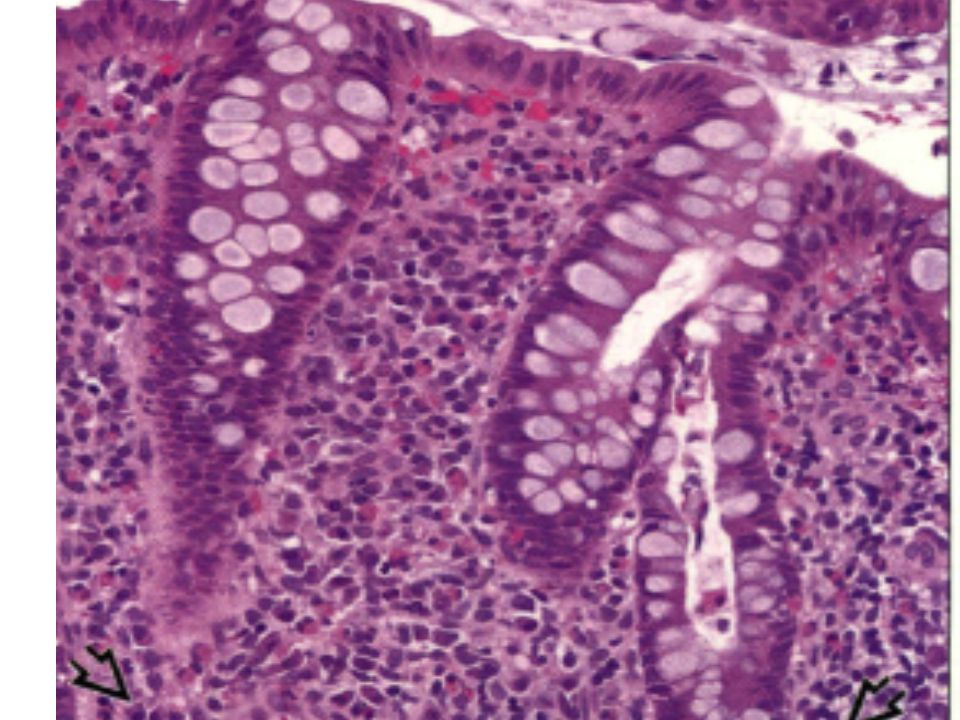
Hematoxylin & eosin shows ulcerative colitis with markedly increased chronic inflammation in the lamina propria, including plasmacytosis at the bases of the crypts ~, architectural distortion (branching crypts), and no increased subepithelial collagen
, and no increased subepithelial collagen")
67
Evidence based pathology How we can increase or evidence ?

68
http://surgpathcriteria.stanford.edu/ http://pathology2.jhu.edu/gicases/

Similar presentations






















>")






>")



 Chapter: The Oral Cavity and the Gastrointestinal Tract.>")