Download presentation
Presentation is loading. Please wait.

1
©2014 MFMER | slide-1 Collagen Vascular Diseases and the Lung Clinical Aspects Robert Vassallo, MD Mayo Clinic, Rochester, MN, USA. Pneumotrieste congress 2014

2
©2014 MFMER | slide-2 Disclosures I have nothing to disclose with respect to this presentation.

3
©2014 MFMER | slide-3 Structure of this talk Part 1 – discuss general concepts on management and diagnostic entities that cause ILD in patients with CTD Part 2 – review clinical features of specific CTD- related ILDs

4
©2014 MFMER | slide-4 Connective Tissue Diseases can affect the lung and thorax in multiple ways Interstitial Lung Disease (ILD) Pleural disease Rheumatoid Nodules Airway disease Vasculitis Pulmonary Hypertension Medication-Induced
 Pleural disease Rheumatoid Nodules Airway disease Vasculitis Pulmonary Hypertension Medication-Induced")
5
©2014 MFMER | slide-5 A variety of histopathological patterns may be seen in association with the rheumatic diseases

6
©2014 MFMER | slide-6 Clinical dilemmas regarding diffuse lung involvement due to CTD Should patients with connective tissue disease- associated ILD get a lung biopsy? Does it really make a difference if we know the specific histologic entity? Can we apply what is known about the idiopathic interstitial pneumonias [for example idiopathic pulmonary fibrosis] to equivalent lesions [ie UIP] seen in patients with rheumatic diseases?

7
©2014 MFMER | slide-7 Variety of radiographic patterns

8
©2014 MFMER | slide-8 Challenges in CTD-ILD management Does biopsy help in any way – prognosis, therapy etc. 35-year-old with severe GERD and Raynaud’s 72-year-old with RA

9
©2014 MFMER | slide-9 DIP UIP LIP / FB NSIP AIP Organizing Pneumonia

10
©2014 MFMER | slide-10 Challenges in CTD-ILD management Does histopathology matter?

11
©2014 MFMER | slide-11 Does it really make a difference if we know the specific histologic entity? Not appropriate to extrapolate data on the idiopathic interstitial pneumonias since studies on the IIPs excluded patients with rheumatic diseases. Even though the idiopathic UIP lesion is morphologically and radiographically highly similar to RA-associated UIP, there are distinct differences in the cellular and molecular profile.

12
©2014 MFMER | slide-12 Should all patients with rheumatic disease- associated ILD get a lung biopsy? No! Consider biopsy if: Young patient (<50years) Patients with atypical HRCT Suspect infection Rule out malignant lymphoid process
 Patients with atypical HRCT Suspect infection Rule out malignant lymphoid process.")
13
©2014 MFMER | slide-13 How similar or different are collagen vascular disease-associated UIP and idiopathic UIP?

14
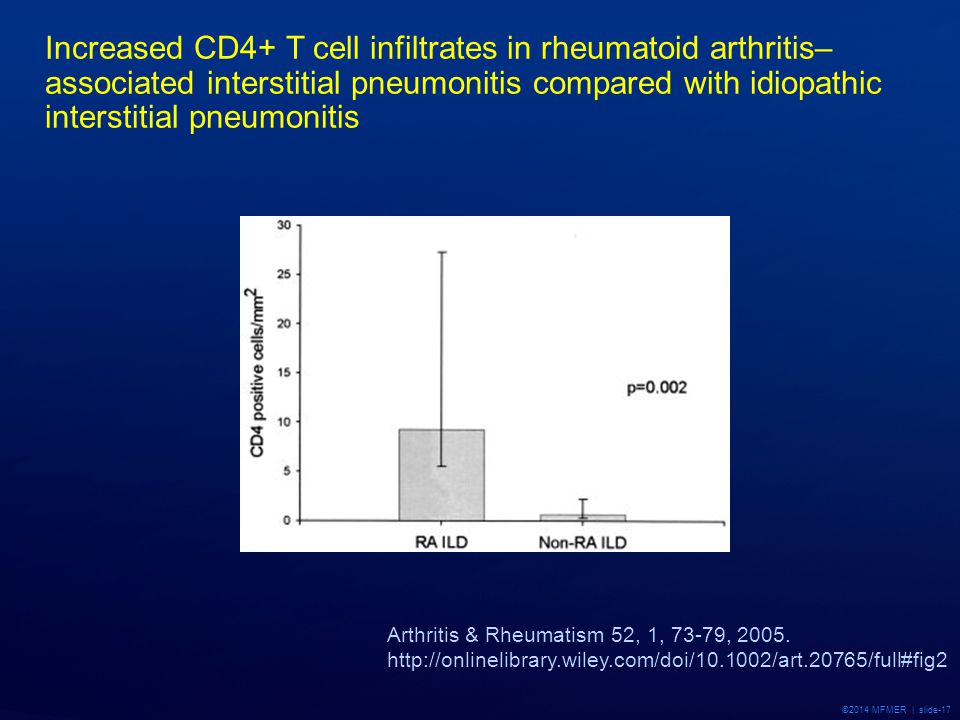
©2014 MFMER | slide-14 Comparing UIP in RA-ILD With IPF Few studies have compared lung biopsies from RA-ILD and UIP pattern with patients with IPF. RA-ILD associated UIP has fewer fibroblast foci when compared with patients with IPF. 1 The number of CD4+ lymphocytes appears to be increased in lung specimens from patients with RA-ILD and UIP pattern vs. patients with IPF. 2 1 Flaherty, Am J Respir Crit Care Med 2003 167 1410-1415. 2 Turesson et al, Arthritis & Rheumatism Vol 52, 2005.

15
©2014 MFMER | slide-15 Hypothesis

16
©2014 MFMER | slide-16

17
©2014 MFMER | slide-17 Increased CD4+ T cell infiltrates in rheumatoid arthritis– associated interstitial pneumonitis compared with idiopathic interstitial pneumonitis Arthritis & Rheumatism 52, 1, 73-79, 2005. http://onlinelibrary.wiley.com/doi/10.1002/art.20765/full#fig2
18
©2014 MFMER | slide-18

19
©2014 MFMER | slide-19

20
©2014 MFMER | slide-20 CD-20CD-138* * CD138 (syndecan) is a heparan sulfate proteoglycan expressed at the pre-B cell stage, lost in mature B cells, and then re- expressed in the mature plasma cell
 is a heparan sulfate proteoglycan expressed at the pre-B cell stage, lost in mature B cells, and then re- expressed in the mature plasma cell")
21
©2014 MFMER | slide-21 Outcomes What do we know about the prognosis of patients with CTD-ILD, and how does it compare with that of the idiopathic interstitial pneumonias?

22
©2014 MFMER | slide-22 CTD-UIP, N=9 IPF/UIP, N=99 (Flaherty et al. Am J Respir Crit Care Med 2003) Prognosis of CTD-related ILD Those with CTD-UIP have better survival compared to IPF/UIP.
 Prognosis of CTD-related ILD Those with CTD-UIP have better survival compared to IPF/UIP..")
23
©2014 MFMER | slide-23 Prognosis of CTD-related ILD (Hubbard et al. Rheumatology 2002) Those with FA- CTD had no better survival than “lone” CFA. Median survival was < 3 yr.
 Those with FA- CTD had no better survival than lone CFA. Median survival was < 3 yr..")
24
©2014 MFMER | slide-24 In this study, the type of ILD, age at diagnosis and %BAL macrophages predicted outcome

25
©2014 MFMER | slide-25

26
©2014 MFMER | slide-26 Survival comparison between idiopathic interstitial pneumonia (IIP) (n = 50) and connective tissue disease- related interstitial lung disease (CTD-ILD) (n = 46) groups. CTD-ILD compared with IIP was associated with a worse prognosis when adjusted for age. (Adjusted for age at Dx) (Kocheril et al. Arth Care Res 2005)
 (Kocheril et al. Arth Care Res 2005).")
27
©2014 MFMER | slide-27 Relevant pathogenetic mechanisms in CTD- ILD Moving towards rationale therapeutics

28
©2014 MFMER | slide-28

29
©2014 MFMER | slide-29 Clinical scenarios and specific diseases

30
©2014 MFMER | slide-30 Rheumatic diseases are multi-system diseases Rheumatoid disease Scleroderma Poly and dermatomyositis MCTD Systemic Lupus Erythematosus Sjogren’s syndrome ANCA associated vasculitis

31
©2014 MFMER | slide-31 A positive serology test (RF, CCP, ANA, etc does not = connective tissue disease!

32
©2014 MFMER | slide-32 Rheumatoid Arthritis Most RA patients with ILD are middle-aged, male, high RF, active joint disease, other extraarticular manifestations. In retrospective, uncontrolled studies, corticosteroids have been reported to improve symptoms, exercise tolerance, radiographic findings, and pulmonary function in patients with RA-associated ILD. However, unclear how many of these “responders” had lesions other than usual interstitial pneumonia.

33
©2014 MFMER | slide-33 How common is diffuse lung disease in RA ? Male smokers are more affected by pleuropulmonary manifestations of RA. Interstitial changes are observed in 80% of lung biopsies, in up to 70% of lung CT and <5% of chest radiographs. Clinically relevant ILD estimated to occur in 17-20 % of RA patients throughout course of the disease [Arthritis Rheum 2010; 62(6) 1583-91].
 ]..")
34
©2014 MFMER | slide-34 Lee, H.-K. et al. Chest 2005;127:2019-2027

35
©2014 MFMER | slide-35 Distinguishing features of RA-ILD Cigarette smoke as a precipitating factor. UIP more prevalent than NSIP (contrast with other CTDs). RA-ILD is more prevalent in males with a 2:1 male to female ratio.
. RA-ILD is more prevalent in males with a 2:1 male to female ratio..")
36
©2014 MFMER | slide-36 * * includes granulomatous reaction; granulomatous vasculitis; lymphoid hyperplasia; and localized pulmonary fibrosis. Distribution of diagnoses on lung biopsy specimens in RA patients with diffuse lung disease Shortness of Breath 2013; 2 (1) 2-9.
")
37
©2014 MFMER | slide-37 Challenges in RA-ILD management What treatment/s to avoid

38
©2014 MFMER | slide-38 Mechanisms of lung disease in RA Why do only some patients develop lung manifestations? RV, 2012

39
©2014 MFMER | slide-39 Lung dominant connective tissue disease

40
©2014 MFMER | slide-40 RA without arthritis Is there such an entity as “Lung dominant CTD”? 77-year-old female referred for evaluation diffuse lung infiltrates. Her troubles began 2 years ago, when she had symptomatic reflux with chest tightness, pressure and recurrent cough. She denied any arthritic joint pain or discomfort. She also denied Raynaud's phenomenon, swallowing difficulties, and skin rashes or skin changes. There has been no skin thickness, vision change, or pleuritic discomfort. Progressive dyspnea: able to walk around the mall but has to stop after a few minutes to rest. She also admits to losing weight over time, although she eats with normal appetite per her report.

41
©2014 MFMER | slide-41

42
©2014 MFMER | slide-42 Bilateral subpleural reticular opacities associated with traction bronchiectasis are present bilaterally. These are more pronounced within the lower lungs. These are at least moderate in overall profusion. A comparison with prior studies is limited given the substantial differences in technique. However, the process appears relatively stable. No definite honeycombing. Labs RF – negative CCP – 128 (strongly positive >60U; negative <20U)
.")
43
©2014 MFMER | slide-43 Fischer et al, Respiratory Medicine, 2012

44
©2014 MFMER | slide-44

45
©2014 MFMER | slide-45 Scleroderma

46
©2014 MFMER | slide-46 Scleroderma Female : Male 4:1 Lung disease is a frequent manifestation, and has replaced renal disease as the leading cause of mortality. The two major types of pulmonary diseases in systemic sclerosis are interstitial lung disease (ILD), and pulmonary hypertension, occurring in up to 50% of patients.
, and pulmonary hypertension, occurring in up to 50% of patients..")
47
©2014 MFMER | slide-47 Copyright ©2007 BMJ Publishing Group Ltd. Changes in Causes of Systemic Scleroderma-related Deaths between 1972 and 2001 GI, gastrointestinal; PAH, pulmonary arterial hypertension; PF, pulmonary fibrosis; SRC, scleroderma renal crisis. Frequency (%) Death (years) 1972 - 761977 - 81 1982 - 86 1987- 911992 - 96 1997 - 2001 0 10 20 30 40 50 P<0.001 (SRC) P<0.001 (PF) SRC PAH GI PF Heart Multi-organ p=0.05 PAH p=0.43 GI p=0.26 Heart Steen, V. D et al. Ann Rheum Dis 2007;66:940-944 SRC PF
 Death (years) P<0.001 (SRC) P<0.001 (PF) SRC PAH GI PF Heart Multi-organ p=0.05 PAH p=0.43 GI p=0.26 Heart Steen, V. D et al. Ann Rheum Dis 2007;66: SRC PF.")
48
©2014 MFMER | slide-48 Pulmonary disease occurs in more than 70% of patients with SSc, second only to the esophagus in frequency of visceral involvement. The presence of ACA has been associated with a lower frequency of radiographic interstitial pulmonary fibrosis and a lesser severity thereof

49
©2014 MFMER | slide-49

50
©2014 MFMER | slide-50 Poly and Dermatomyositis

51
©2014 MFMER | slide-51 Chest CT

52
©2014 MFMER | slide-52

53
©2014 MFMER | slide-53

54
©2014 MFMER | slide-54 Histopatholgical Findings 1. An acute respiratory failure evolving in a few days or weeks with fever, bilateral infiltrates and a negative search for pathogens. Histopathology reveals a DAD [usually poor prognosis despite aggressive treatment]. Some forms are responsive to corticosteroids - NSIP, or organizing pneumonia or acute alveolar hemorrhage with pulmonary capillaritis. 2. A progressive interstitial lung disease with cough and dyspnea. NSIP is the predominant pattern (65-80%, predominantly fibrotic or mixed forms), much more frequent than UIP, organizing pneumonia or LIP pattern.
, much more frequent than UIP, organizing pneumonia or LIP pattern..")
55
©2014 MFMER | slide-55 One-year survival for patients with PM-DM-ILD was 85.8%, 3-yr survival was 74.7%, and 5-yr survival was 60.4%. Survival is better (p < 0.001) for the PM-DM- ILD group when compared with the group with IPF, and is not different from the group with idiopathic NSIP (p = 0.247).
 for the PM-DM- ILD group when compared with the group with IPF, and is not different from the group with idiopathic NSIP (p = 0.247)..")
56
©2014 MFMER | slide-56 Diagnostic studies in Poly / Dermatomyositis CK-MM and CK–MB (most sensitive) LDH (least specific) Aldolase (most specific) Measure before EMG (Normal EMG in 10.7%: EMG supportive, not diagnostic: may direct biopsy sites) Muscle biopsy diagnostic (T cells infiltrate the muscle fasciculi and surrounding individual healthy muscle fibers, resulting in phagocytosis and necrosis)
 LDH (least specific) Aldolase (most specific) Measure before EMG (Normal EMG in 10.7%: EMG supportive, not diagnostic: may direct biopsy sites) Muscle biopsy diagnostic (T cells infiltrate the muscle fasciculi and surrounding individual healthy muscle fibers, resulting in phagocytosis and necrosis)")
57
©2014 MFMER | slide-57 Systemic Lupus Erythematosus

58
©2014 MFMER | slide-58 SLE Pleurisy and Pericarditis DAH Pul HTN

59
©2014 MFMER | slide-59 Sjogren’s syndrome A slowly progressive inflammatory disease affecting primarily the exocrine glands Lymphocytic infiltrates Characteristic autoantibodies - Ro, La Mucosal dryness - eyes, mouth, genital tract

60
©2014 MFMER | slide-60 Sjogren’s syndrome Extra-glandular disease polyarthritis, lungs, kidneys, liver, blood vessels Association with other autoimmune disease RA, SLE, systemic sclerosis, polymyositis

61
©2014 MFMER | slide-61 Grazie

Similar presentations











 How we could do better Dr. D. K. Pillai Wednesday, 13 th August 2014 Medical Update Group at UoM.>")







