Download presentation
Presentation is loading. Please wait.

1
Journal Club

4
Sudden Unexpected Infant Death (SUID) Sudden unexpected infant deaths are defined as deaths in infants less than 1 year of age that occur suddenly and unexpectedly, and whose cause of death are not immediately obvious prior to investigation. Each year in the United States, more than 4,500 infants die suddenly of no immediately, obvious cause.

5
Sudden unexpected infant deaths (SUID) can be subdivided into: –1- explained SUID : includes deaths for which the medical examiner determines that there is a specific cause –2- unexplained SUID : includes those deaths considered to be sudden infant death syndrome (SIDS) Half of these Sudden Unexpected Infant Deaths (SUID) are due to Sudden Infant Death Syndrome (SIDS).
 can be subdivided into: –1- explained SUID : includes deaths for which the medical examiner determines that there is a specific cause –2- unexplained SUID : includes those deaths considered to be sudden infant death syndrome (SIDS) Half of these Sudden Unexpected Infant Deaths (SUID) are due to Sudden Infant Death Syndrome (SIDS).")
6
5 % 1-5%

7
Sudden Infant Death Syndrome

8
The current definition of SIDS, developed in 1991, is the sudden death of an infant younger than one year that remains unexplained after a thorough case investigation, including a complete autopsy, examination of the death scene, and review of the clinical history. In the United States, SIDS affects 0.57 per 1,000 live births, totaling more than 2,200 deaths per year. In Israel by 2005 SIDS affects 0.36 per 10000 live birth.

9
SIDS remains the third leading cause of death in infancy and the most common cause of death between 1 month and 1 year of age. SIDS usually occurs between the second and fourth months of life. Over 80 percent of SIDS deaths occur between midnight and 6 AM

11
תמותת תינוקות בישראל Because most infant deaths are incompletely investigated, the true incidence of sudden infant death syndrome in Israel is not known.

12
Risk Factors Infant factors : –low birth weight –low Apgar scores –recent viral illness –Native American or African American ancestry –male sex –Prone sleeping Maternal issues : –low socioeconomic status –Smoking –illicit drug use –poor prenatal care –young age –Crowded household –parental unemployment –Single parent

14
Sleeping position is the most easily modifiable risk factor breast-feeding Room-sharing Fan use 0.28(0.10-0.77) 0.55(0.44-0.69)
 0.55( )")
15
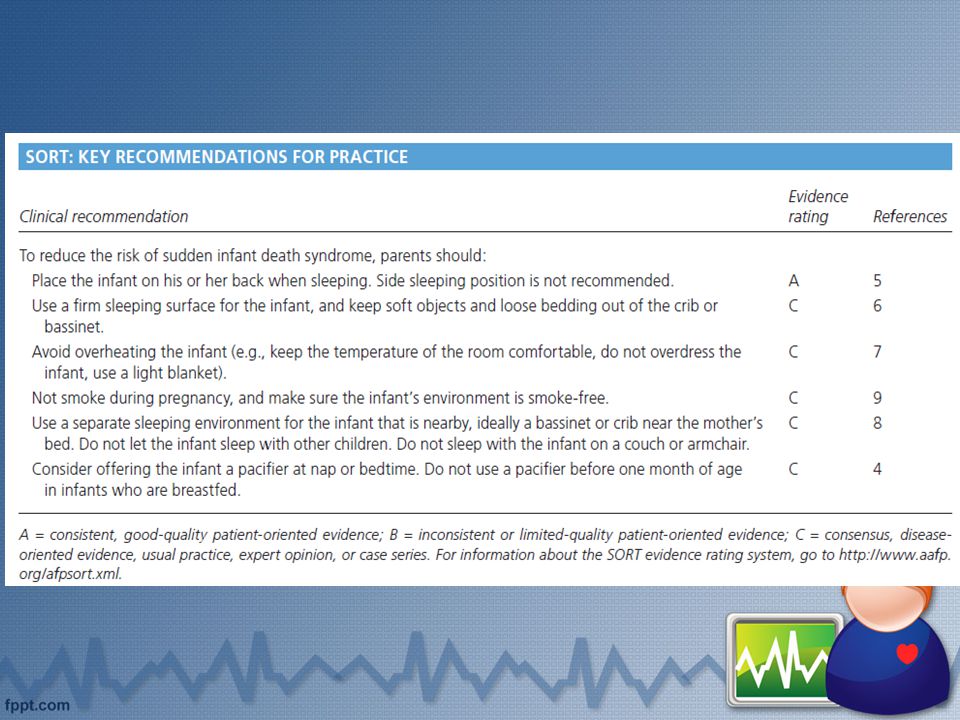
“Back to Sleep” campaign

18
Patient education efforts that recommended the supine sleeping position in the 1990s resulted in a 50 to 70 percent decrease in SIDS rates.

21
Pathophysiology SIDS is a polygenic, multifactorial condition, with genetic, environmental, and behavioral/sociocultural factors as contributors. Failure of arousal mechanisms likely plays an important role in the final pathway to death.

22
Significant controversy revolves around the pathophysiology of SIDS. Three common autopsy findings include unclotted blood in the heart, intrathoracic petechiae and fluid-filled, heavier organs. “Apnea theory” of SIDS was proposed in the 1970s which led to the creation of an apnea monitoring industry.

23
Current literature supports a triple-risk model, which suggests that SIDS is the final common pathway of three coinciding factors: –An underlying vulnerability –Stressed by an exogenous source –Occur during a critical developmental period

25
Current SIDS research topics include investigation of ion channel abnormalities, autonomic nervous system disturbances, and the effects of nicotine on the developing brain. Failure of arousal mechanisms likely plays an important role in the final pathway to death. Serotonin receptor abnormalities have been found throughout the ventral medulla in victims of SIDS.

26
Polymorphisms occurring at higher incidence in SIDS compared to controls: –7 cardiac ion channelopathy genes that are proarrhythmic –3 5-HT genes –8 autonomic nervous system (ANS) development genes –6 genes related to infection and inflammation that are pro- inflammatory –1 gene related to energy production.
 development genes –6 genes related to infection and inflammation that are pro- inflammatory –1 gene related to energy production.")
27
DEFORMATIONAL PLAGIOCEPHALY Deformational plagiocephaly is flattening of the occiput, which affects up to one half of infants who sleep in the supine position. To decrease the risk of skull deformities, infants should have supervised “tummy time,” meaning that when awake, infants should spend as much time as possible on their stomachs.

33
A history of one or more apneic episodes does not increase the risk of SIDS, and the use of home apnea monitors does not lower the risk of SIDS. Pacifier use appears to decrease the risk of SIDS, and the 1995 AAP position statement on SIDS prevention suggests offering the infant a pacifier at nap or bedtime.

36
Investigation of a potential SIDS death should include a thorough death scene evaluation and a complete autopsy, with a radiographic skeletal survey and toxicology studies. A known cause of death is identified by the postmortem examination in approximately 15 percent of suspected SIDS cases. The status of “virtopsy” as a potential alternative to traditional autopsy.

39
Apparent Life-Threatening Events

40
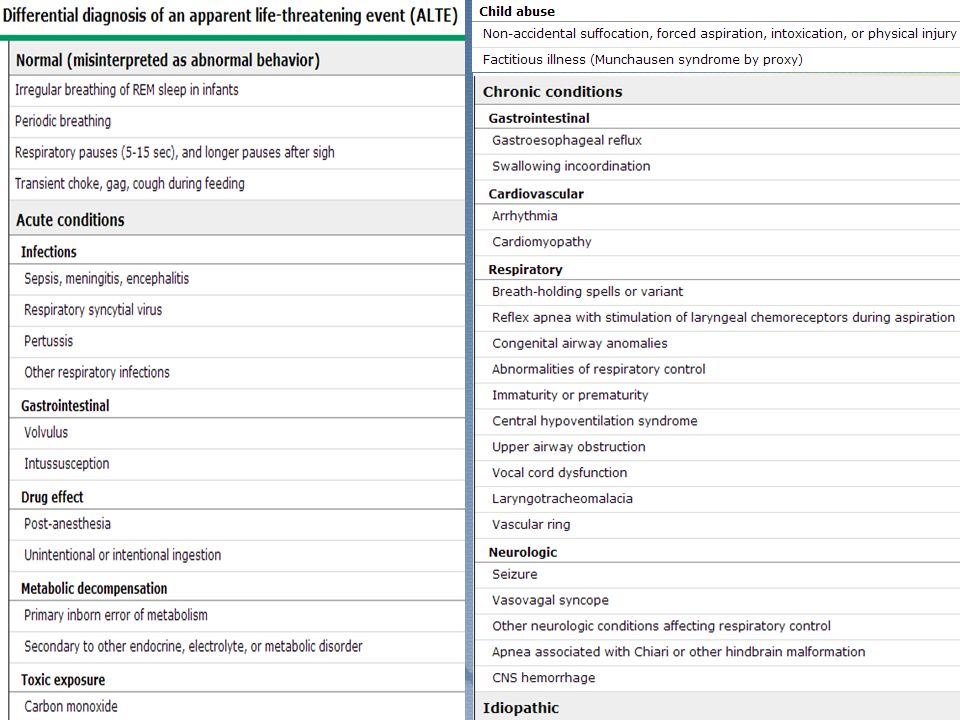
Apparent life-threatening events (ALTEs) are apneic episodes associated with changes in skin color (e.g., cyanosis, pallor, erythema), changes in muscle tone, and choking or gasping. ALTEs are relatively common, occurring in approximately one in 400 infants. Recovery occurs only after stimulation or resuscitation.

41
Risk factors for ALTEs : –history of apnea, cyanosis, or pallor –feeding difficulties –single parenthood –family history of infant death –smoking during pregnancy An etiology for ALTEs is determined in only one half of cases. Over 82 percent of ALTE episodes occur between 8 AM and 8 PM

42
Gastrointestinal etiologies (usually gastroesophageal reflux) account for most cases in which a cause is identified. Respiratory infections. Cardiac disorders, such as valvular disease, arrhythmia, and cardiomyopathy, are responsible for a minority of cases. Neurologic causes, such as malignancy, structural abnormalities of the brain, and seizures, are uncommon, but should be considered.

45
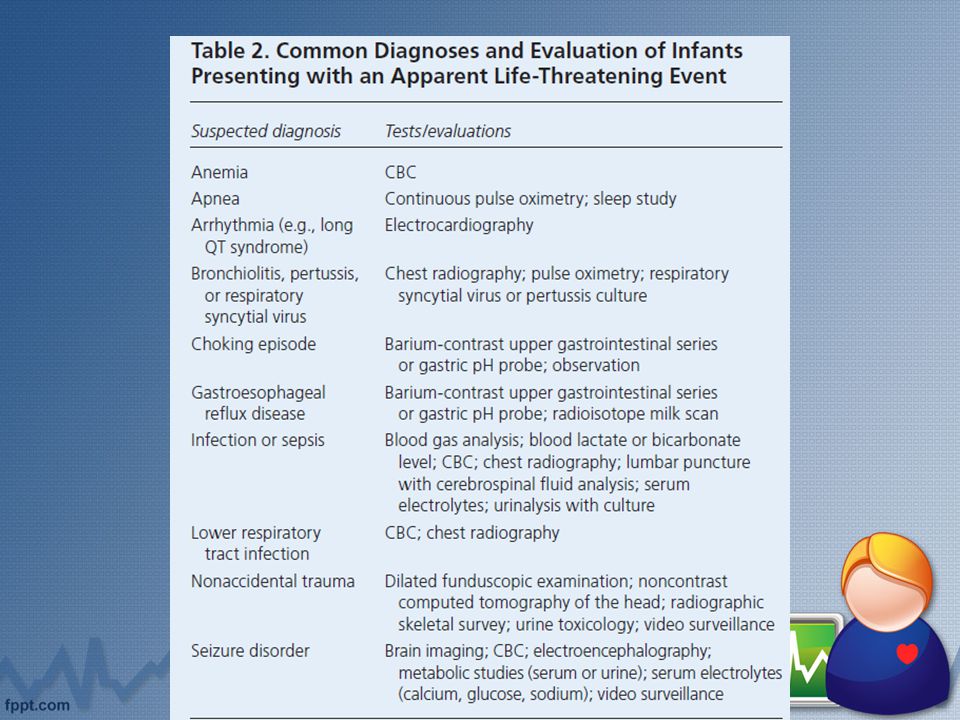
Evaluation The history and physical examination are the most important factors in determining an etiology. In a case series of 243 patients admitted to a single academic medical center, fewer than 6 percent of all tests ordered were useful in making the diagnosis. The only tests found to be of value in detecting causes of ALTEs were: testing for gastroesophageal reflux, urinalysis, neuroimaging, chest radiography, and white blood cell count.

46
If the history and physical examination suggest that the event was not life-threatening, or if a probable explanation for the event is identified then no laboratory evaluation may be required. In some cases, a limited evaluation is performed to confirm the suspected diagnosis. If the detailed description of the event suggests that the child was physiologically compromised, then in-hospital observation with cardiorespiratory monitoring is indicate.

47
The initial laboratory evaluation usually includes: –complete blood count –urinalysis –plasma concentrations of glucose, electrolytes, blood urea nitrogen (BUN), calcium, magnesium –chest radiograph –electrocardiogram –toxicology screen
, calcium, magnesium –chest radiograph –electrocardiogram –toxicology screen")
50
Indications for Home Cardiorespiratory (CR) monitoring Apnea of prematurity Tracheostomy or airway abnormalities Neurologic or metabolic disorders affecting respiratory control Chronic lung disease
 monitoring Apnea of prematurity Tracheostomy or airway abnormalities Neurologic or metabolic disorders affecting respiratory control Chronic lung disease")
51
The End

Similar presentations

































 By: Alex Boreen, Brittany Drees, and Jennifer Klein.>")




