Download presentation
Presentation is loading. Please wait.

1
Vision Loss KHADER M.FARWAN

2
Objectives Review of eye anatomy
Refine history and examination of the eye Work through emergent causes of sudden monocular vision loss in a case-based format

3
Spelling Review Ophthalmology

4
Anatomy Review Function & transperancy Eyeball-ology

5
Anatomy Review

6
Anatomy Review Eyelids Tears Cornea Aqueous Lens Vitreous
Lacrimal gland Cornea – Body (stroma) arranged regular lattice pattern, Deep surface (Endothelium) continually extracts water from stroma Aqueous – transparent blood substitute, from ciliary epithelium, fills ant. Chamber, drained by trabecular meshwork at angle iris-cornea
 arranged regular lattice pattern, Deep surface (Endothelium) continually extracts water from stroma. Aqueous – transparent blood substitute, from ciliary epithelium, fills ant. Chamber, drained by trabecular meshwork at angle iris-cornea.")
7
Anatomy Review Retina Fovea / “Macula”
Central retinal artery supplied by branch of ophthalmic artery (1st major branch of internal carotid) Image: maladies.htm Retina has highest consumption per unit wt of any tissue in body Arteries usually lighter in color, more prominent Veins (?) 3:2 size CRA supplies inner retina
 Image: maladies.htm. Retina has highest consumption per unit wt of any tissue in body. Arteries usually lighter in color, more prominent. Veins ( ) 3:2 size. CRA supplies inner retina.")
8
Anatomy Review Optic nerve or retinal lesions do not respect vertical meridian Defects that clear or start at vertical midline signify lesion at chiasm or beyond Buys them a scan.

9
Vision Loss Categorization Total or Partial One or Both eyes
Sudden or Gradual Painful or Painless Optic neuritis…. One contact in… for example. “what was the circumstance that made you notice?? Perfect not, cover your eye?” esp in older.

10
History Question Danger Signs How long ago? Recent
How sudden? Sudden: ischemia or bleed Course? Worsening Rapid: vascular, inflammatory, demyelinating causes. Slowly progressive is compressive lesion till proven otherwise. Caution, some will be chronic course, only noticed acutely (Eg closed one eye)
")
11
History What do they see? Key symptoms Flashes or floaters
“Curtain” rising or falling Central patch or distortion Key symptoms Pain or headache Nausea / Vomiting Localizing to temporal artery…? 20% have normal ESR!! Do a CRP if suspicious… buys them consult. (NEJM august 2002 giant cell arteritis / pmr). Incr ICP usually transient vis obscuration. Central patch amd w neovascularization/bleed, optic neuritis. What do they see???? Symmetry…
. Incr ICP usually transient vis obscuration. Central patch amd w neovascularization/bleed, optic neuritis. What do they see Symmetry…")
12
History In addition to general Hx/Px:
Usual corrective glasses / contacts? Still in? Previous transient episodes? Trauma? CVS, heme/onc, drug hx… are the contacts in or not?? Soft contacts: 1-2 mm past limbus, folllowing it around! Will stain with fluorescein.

13
Examination Visual acuity Visual field testing Swinging light test
Direct ophthalmoscopy Dilating the eye Tonometry Exam tips. Assume proficiency with testing EOM, fluorescein, slit-lamp, Amsler -> metamorphopsia. Look at dot, do you see all four corners, are all the squares the same, are all lines straight? Grey out/negative scotoma => optic neuritis…. RD, MD

14
Examination Visual acuity Snellen chart 20 feet distance
Credit for a line if most letters correctly identified If acuity poorer than largest letter (eg 20/200), measure distance pt can read it (eg 5/200 at 5 feet)
, measure distance. pt can read it (eg 5/200 at 5 feet)")
15
Examination Visual acuity
Practically, if that poor, acuity described by Finger-counting Hand-motion Light perception

16
Examination Visual acuity To correct refractive error: Use pin hole
Use ophthalmoscope

17
Examination Visual field testing Confrontation
With the patient looking at your nose, ask if your nose and other facial features are seen clearly Inability to clearly see your: Nose => central scotoma Eyes or lips => paracentral scotoma Ears => peripheral visual field defect Finger counting. (Macular=central , peripheral=>retinal detachment?…) (Normal nasal obstruction of field)
 (Normal nasal obstruction of field)")
18
Examination Swinging light test
Relative Afferent Pupillary Defect (RAPD) See “Marcus-Gunn Pupil” Significant retinal or optic nerve disease, in one eye more than the other Very helpful for Ophtho to know in consult Dilates or weaker initial constriction.
 See Marcus-Gunn Pupil Significant retinal or optic nerve disease, in one eye more than the other. Very helpful for Ophtho to know in consult. Dilates or weaker initial constriction.")
19
Examination Direct ophthalmoscopy Close as possible
Remove your glasses Switch viewing eye Start at zero correction Or to correct observer refraction (eg – 4 diopters) Rotate counter-clockwise for near-sighted pt dim environ, sit them up so you’re standing comfortably, use smallest aperature Better use of the ophthalmoscope. Luff A, Elkington A. Practitioner. 236(1511): 161-5
 Rotate counter-clockwise for near-sighted pt. dim environ, sit them up so you’re standing comfortably, use smallest aperature. Better use of the ophthalmoscope. Luff A, Elkington A. Practitioner. 236(1511):")
20
Examination Direct ophthalmoscopy Red Reflex
Compare brightness and color at 1-2 feet Indicates media free of opacity Not always easy to do, helpful if (N) “Eight-ball” Vitreous hemorrhage Move in along line of red reflex Aim for opposite mastoid process Often brings optic disc straight into view Image eg vitreous hem. RD, (not always easy to do… esp w large refractive error VH-diffuse, dark, particulate opacities overlying red reflex, or total loss. Immediate ophtho referral
 Eight-ball Vitreous hemorrhage. Move in along line of red reflex. Aim for opposite mastoid process. Often brings optic disc straight into view. Image eg vitreous hem. RD, (not always easy to do… esp w large refractive error. VH-diffuse, dark, particulate opacities overlying red reflex, or total loss. Immediate ophtho referral.")
21
Examination Direct ophthalmoscopy Place free hand on forehead Comfort
Prevents facial contact Resting own forehead on thumb stabilises image Able to lift upper lid if necessary Comfort Encourage subject to keep breathing during examination Sit patient up, avoid hunching Image

22
Examination Direct ophthalmoscopy Use anti-glare filter
Try red-free filter for better vessel visualization

23
Examination Direct ophthalmoscopy PanOptic Ophthalmoscope
Greater field of view “5x larger view of fundus” USD $400 range Images

24
imc.gsm.com/integrated/ bcs/heent/page14.html
Anatomy Review Optic disc Color: Yellow-orange, central cup whiter Size: Cup less than half diameter of disc Margin: Sharp (may be less sharp nasally) Follow vessels in… mm at 1 m aperture, should be slightly smaller than disc (N) . Can I see the back of the eye?? If not?? Hazy—vitreous hemorrhage, varying focus--RD imc.gsm.com/integrated/ bcs/heent/page14.html
 Follow vessels in… mm at 1 m aperture, should be slightly smaller than disc (N) . Can I see the back of the eye If not Hazy—vitreous hemorrhage, varying focus--RD. imc.gsm.com/integrated/ bcs/heent/page14.html.")
25
imc.gsm.com/integrated/ bcs/heent/page14.html
Anatomy Review Fovea / “Macula” Color: Slightly darker, devoid of retinal vessels Size: Same as disc Location: Temporal and slightly inferior to disc Macula lutea imc.gsm.com/integrated/ bcs/heent/page14.html

26
imc.gsm.com/integrated/ bcs/heent/page14.html
Anatomy Review Vessels Size: 3:2 Vein:Artery Caliber: look for abnormal tortuosity 4 main vascular arcades Superior- & Inferior- Nasal & Temporal Cilioretinal artery Vein:Artery 3:2 ?? Cilio retinal . Look for tortuosity imc.gsm.com/integrated/ bcs/heent/page14.html

27
Examination Direct ophthalmoscopy Four quadrant scan
Follow vessels to periphery (may need to re-focus) Get pt to look at the light to see macula Images
 Get pt to look at the light. to see macula. Images")
28
Examination Dilating the eye Especially important for suspected
Intraocular FB Central retinal artery occlusion Retinal detachment Hesitancy amongst non-ophthalmologists No ophtho would attempt full exam through undilated pupil. But concerns re: RAPD if dilate both

29
Examination Dilating the eye Tropicamide 1%
Mydriasis and glaucoma: exploding the myth. A systematic review. Pandit RJ, Taylor R. Diabet Med Oct;17(10):693-9 “Risk of inducing acute glaucoma following … tropicamide alone close is to zero, no case being identified” Near fatal anticholinergic intoxication after routine fundoscopy. Brunner GA, et al. Intensive Care Med Jul;24(7):730-1.
: Risk of inducing acute glaucoma following … tropicamide alone close is to zero, no case being identified Near fatal anticholinergic intoxication after routine fundoscopy. Brunner GA, et al. Intensive Care Med Jul;24(7):")
30
Examination Dilating the eye Tropicamide 1% Contraindications:
Acute head injury/coma Acute or intermittent angle-closure glaucoma (but NOT chronic open-angle glaucoma) Probably anyone at high risk for above (eg. Older asian lady, severely far-sighted person) “mydriacyl” Asians at risk, far-sighted, => probably shouldn’t be dilating eg. Older asian lady. !!! Van Herrick
 Probably anyone at high risk for above. (eg. Older asian lady, severely far-sighted person) mydriacyl Asians at risk, far-sighted, => probably shouldn’t be dilating eg. Older asian lady. !!! Van Herrick.")
31
Examination Dilating the eye Tropicamide 1%
Onset mins, duration 4-6 h Side effects: blurred vision, light sensitvity Safety: must not drive for 6 h The effect of pupil dilation with tropicamide on vision and driving simulator performance. Potamitis, T., et al. Eye Jun;14 (3A):302-6
:")
32
Examination Tonometry Tonopen
Contraindicated if suspected ruptured globe Ttono = 10 – 21 mm Hg (N) False elevation IOP Blepharospasm (“squeezers”) Avoid pressure on the eye by holding eyelids only against bony orbital rim
 False elevation IOP. Blepharospasm ( squeezers ) Avoid pressure on the eye by holding eyelids only against bony orbital rim.")
33
Case 1 SUDDEN, TOTAL LOSS, ONE EYE
70 yo F with HTN, DM lost vision in one eye over a few minutes earlier this morning. No trauma. No eye pain, or N/V Findings: (N) External eye and EOM, red reflex (N) Acuity on left, only hand motion right RAPD+ (N) Fundoscopy unaffected eye Clues: sudden Monocular – lesion in visual pathway must be anterior to optic chiasm (eye itself or optic nerve)
 External eye and EOM, red reflex. (N) Acuity on left, only hand motion right. RAPD+ (N) Fundoscopy unaffected eye. Clues: sudden. Monocular – lesion in visual pathway must be anterior to optic chiasm (eye itself or optic nerve)")
34
Case 1 Retina pale “Cherry Red Spot” fovea Splinter hemorrhage
?boxcarring here? = segmentation of blood column in retinal arterioles “cherry red spot” may take hrs to develop (up to 24) Clinical Eye Atlas
 Clinical Eye Atlas.")
35
Case 1 Diagnosis? Treatment? Massage eyeball Timoptic drops
Sticking a needle in the eye Clinical Eye Atlas

36
Central Retinal Artery Occlusion
Sudden painless monocular loss of vision May have history of previous transient episodes. “Amaurosis fugax” Greek “amauros: dark, obscure” + “-osis, condition” “fugax, fleeting eg. Fugitive”

37
Central Retinal Artery Occlusion
Retina infarction => pallor, edema, less transparency Irreversible damage begins at 90 mins Animal studies. Thrombolytic studies show reversibility possible after longer periods in humans The longest delay to treatment that has been associated with significant visual recovery is approximately 72 hours Conservative approach is to treat < 24 hrs

38
Central Retinal Artery Occlusion
Macula, thinnest portion, remains visible Cherry red spot may take 24 h to develop Visual acuity may be normal if cilioretinal vessel patent (N) choroidal blood flow to fovea => cherry red spot. If a cilioretinal artery from choroid supplies macula (up to 20% of pts), acuity may be 20/40 rather than 20/400
 choroidal blood flow to fovea => cherry red spot. If a cilioretinal artery from choroid supplies macula (up to 20% of pts), acuity may be 20/40 rather than 20/")
39
Central Retinal Artery Occlusion
Causes Embolic (carotid, cardiac) Thrombosis Temporal arteritis Vasculitis (eg. lupus) Sickle cell disease Trauma Embolic cause in majority. images/521crao1.JPG
 Thrombosis. Temporal arteritis. Vasculitis (eg. lupus) Sickle cell disease. Trauma. Embolic cause in majority. images/521crao1.JPG.")
40
Central Retinal Artery Occlusion
Treatment Attempt moving embolus distally: Digital massage Firm steady pressure x 15 seconds, release, repeat IOP lowering drugs Beta-blockers/CAI/alpha-agonists… +/- Vasodilation techniques Rebreathing to increase PaCO2

41
Central Retinal Artery Occlusion
Treatment Consult ophthalmology immediately Paracentesis anterior chamber ?? HBO, thrombolytics Locate source ESR for temporal arteritis ECG for A. fib Medicine consult (Carotid doppler, ECHO?…)
")
42
How to Tap an Eye Anterior chamber paracentesis
Administer local anesthesia Use a 30-gauge needle on a tuberculin syringe Enter the eye at the limbus with bevel up Ensure that the needle does not damage the lens Withdraw fluid until the anterior chamber shallows slightly ( cc) Administer a topical antibiotic post-procedure
 Administer a topical antibiotic post-procedure.")
43
Central Retinal Artery Occlusion
Complications Vision loss Prognosis poor in most But up to 10% retain central vision (acuity improves to 20/50 or better in 80% of those) Recurrent thromboemboli CVA Further visual loss to same or contralateral eye Progression of temporal arteritis
 Recurrent thromboemboli. CVA. Further visual loss to same or contralateral eye. Progression of temporal arteritis.")
44
Case 2 PARTIAL LOSS, ONE EYE
A 60 yo M with HTN and DM complains of progressive loss of vision in one eye over the last 2 days. No other symptoms Painless uniform dulling of vision. Findings: (N) External eye and EOM Acuity 20/25 OD, 20/200 OS RAPD+ (N) Fundoscopy unaffected eye
 External eye and EOM. Acuity 20/25 OD, 20/200 OS. RAPD+ (N) Fundoscopy unaffected eye.")
45
Case 2 How would you manage this at 2 AM? Immediate ophtho consult
Thrombolytic therapy Decrease the intraocular pressure Globe massage to dissolve clot None of the above Flame hemorrhages.. Wait till AM r/o mechanical cause eg proptosis, trauma, etc… Clinical Eye Atlas

46
Case 2 Unmistakable fundoscopy: “Blood and Thunder” or
“Ketchup fundus” Dilated tortuous veins Flame hemorrhages Disc edema Clinical Eye Atlas

47
Central Retinal Vein Occlusion
Key facts 10 times more common than CRAO Painless monocular loss of vision over hours to days Vision may improve through the day ? CRV impingement by lamina or atherosclerosis of CRA Ischemic vs. non-ischemic types Variability due to ?gravity reducing macular edema ?nocturnal arterial hypotension. Pathogenesis unknown: CRV impingement => turbulence, endothelial damage, throbosis and vein occlusion => different severity If ischemia not a major element then central vision and pupil reaction will be spared.

48
Central Retinal Vein Occlusion
Risk Factors Age > 50 Diabetes HTN Hyperviscosity syndromes Glaucoma Recurrent amaurosis fugax

49
Central Retinal Vein Occlusion
Non-ischemic Good vision RAPD absent Fewer retinal hemorrhages Cotton-wool spots May resolve fully or progress to ischemic type Complete recovery with good visual recovery only in 10%, 20/200 or worse vision in 50%, 1/3 convert to ischemic type

50
Central Retinal Vein Occlusion
Ischemic Severe visual loss RAPD+ Extensive retinal hemorrhage and cotton-wool spots

51
Central Retinal Vein Occlusion
Treatment No known effective treatment or prevention Ophthalmology may consider: ASA Anti-coagulation Fibrinolytics Corticosteroids Anti-inflammatories Generally ASA to all

52
Central Retinal Vein Occlusion
Treatment Medical follow-up to screen for atherosclerosis and other risk factors Ophthalmology assessment to follow for late complications (~ 3 mos)
")
53
Central Retinal Vein Occlusion
Complications Ocular neovascularization Anterior => neovascular glaucoma Posterior => vitreous hemorrhage Poor vision (20/200 or worse in 90%) Secondary glaucoma Tx: photocoagulation
 Secondary glaucoma. Tx: photocoagulation.")
55
Case 3 A 50 yo M presents with a 2 day history of persistent flashing lights and floaters in one eye, as well as a tiny shadow in one corner Findings: (N) External eye and EOM (N) Acuity 20/20 bilaterally (N) Visual field testing RAPD absent (N) Fundoscopy unaffected eye Flashes/floaters in both eyes intracranial, vs monocular sx. CALLL RIGHT AWAY!! Want to know quick so they can tx ASAP
 External eye and EOM. (N) Acuity 20/20 bilaterally. (N) Visual field testing. RAPD absent. (N) Fundoscopy unaffected eye. Flashes/floaters in both eyes intracranial, vs monocular sx. CALLL RIGHT AWAY!! Want to know quick so they can tx ASAP.")
56
Case 3 At 2 AM would you: Send home with GP follow-up
Instill tropicamide and repeat exam Call ophthalmology immediately Keep the patient overnight for ocular U/S C wake ‘em up catch ‘em with macular on

57
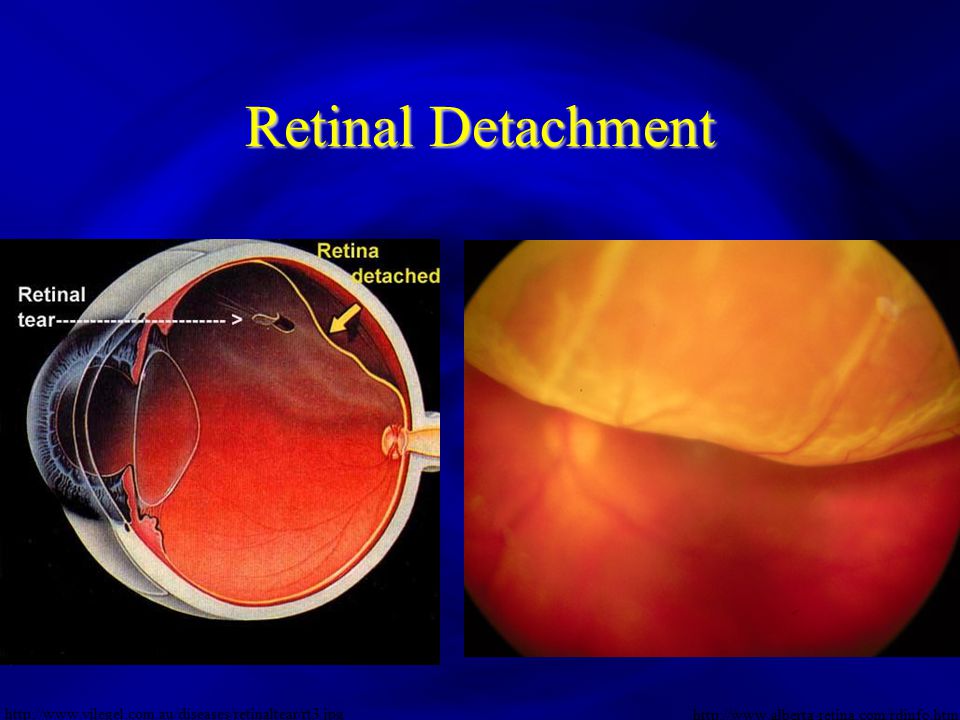
Retinal Detachment Separation of inner sensory layers from underlying RPE Tear in retina Traction Subretinal fluid Mechanical stimulation of retinal tissue. ** constant flashes/floaters… transient, not as urgent

58
Anatomy Review Potential space with no adhesions between layers
Potential space, no adhesions between them. photodynamic_therapy.htm Potential space with no adhesions between layers

59
Retinal Detachment Risk Factors Severe myopia (eg. –12 to –15)
Advanced age Previous cataract surgery Blunt trauma Family history

60
Retinal Detachment History Shower of black spots or floaters
Flashing lights (photopsia) From a “shadow” in periphery to “dark curtain” Wavy distortion of objects (metamorphopsia) Differential diagnosis of flashing lights includes scintillating scotoma of migraine, vitreous detachment, retinal tear, and retinal detachment. Metamorphopsia – from fluid disrupting retinal position in macular area
 From a shadow in periphery to dark curtain Wavy distortion of objects (metamorphopsia) Differential diagnosis of flashing lights includes scintillating scotoma of migraine, vitreous detachment, retinal tear, and retinal detachment. Metamorphopsia – from fluid disrupting retinal position in macular area.")
61
Retinal Detachment Beware! Visual field defects Fundoscopy Late sign
Patients less aware of superior field defects Most common defect is inferiorly (hard to detect because of nose) Fundoscopy Dilated eye exam a MUST (maybe not by us) Detachments start in periphery, difficult to visualize superior field defect indicates an inferior detachment. We don’t look up very often. we’re not going to see small findings if subtle, judgement call, but need ophtho dilated exam by co/ophtho if they can see as good as you out to periphery less worried
 Fundoscopy. Dilated eye exam a MUST (maybe not by us) Detachments start in periphery, difficult to visualize. superior field defect indicates an inferior detachment. We don’t look up very often. we’re not going to see small findings if subtle, judgement call, but need ophtho dilated exam by co/ophtho. if they can see as good as you out to periphery less worried.")
62
Retinal Detachment Beware! Location
Superior field defect indicates an inferior retinal detachment Detachments of the superior retina are far more serious May rapidly extend inferiorly to involve the macula and thereby cause the loss of central vision.

63
Retinal Detachment right
64
Retinal Detachment Treatment
Consult ophthalmology immediately any time of night esp. if “mac on” Prevent worsening RD Bed rest, supine if superior RD Protect eye from trauma (eg. metal eye shield)
")
65
Retinal Detachment Treatment Transient floaters not as urgent
Full exam in clinic likely needed Home with ophtho call and follow-up WARNING: RT ED if FURTHER flashing lights or floaters, LASTING more than seconds

66
Case 4 SUDDEN, TOTAL LOSS, ONE EYE
60 yo F with a unilateral headache for one week lost all vision in her right eye over a few minutes. No trauma, eye pain, or N/V Findings: (N) External eye and EOM (N) Acuity on left, only hand motion right RAPD+ Visual field testing normal (N) Fundoscopy unaffected eye Jaw fatigue on chewing
 External eye and EOM. (N) Acuity on left, only hand motion right. RAPD+ Visual field testing normal. (N) Fundoscopy unaffected eye. Jaw fatigue on chewing.")
67
Case 4 The patient most likely has Papilledema CRAO CRVO
Ischemic Optic Neuropathy (ION) Temporal arteritis Clinical Eye Atlas
 Temporal arteritis. Clinical Eye Atlas.")
68
Pale, swollen optic disc
Case vs Case 1 Lack of cherry red spot, though both have splinter hemorrhages Pale, swollen optic disc Clinical Eye Atlas

69
Anterior Ischemic Optic Neuropathy (AION)
Acute ischemia or infarction optic nerve head Arteritic Non-arteritic Supplied by small posterior ciliary arteries. May be sectoral or all way around

70
Anterior Ischemic Optic Neuropathy (AION)
Sudden unilateral loss of vision May be altitudinal Pallid optic disc swelling “Chalky white” Supplied by small posterior ciliary arteries. May be sectoral or all way around

71
Arteritic (AAION) Association with Temporal Arteritis Suspect if
Age >50 Headache Jaw pain or fatigue on chewing (claudication) Scalp tenderness Puts other eye at up to 50% risk of same
 Scalp tenderness. Puts other eye at up to 50% risk of same.")
72
Arteritic (AAION) Treatment Send ESR and start steroids if elevated
Prednisone mg PO OD Temporal artery biopsy within 1 week

73
Non-Arteritic (NAAION)
Presumably atherosclerotic Treatment Follow-up for atherosclerotic risk factors ASA

75
Case 5 SUDDEN, PARTIAL LOSS, ONE EYE
60 yo M with migraine history complains of painful blurry vision in one eye over a few minutes. No trauma. Unlike past migraines Significant nausea, vomiting, diaphoresis Findings Red eye Only hand motion visual acuity one eye Unable to examine further because of photophobia

76
Case 5 SUDDEN, PARTIAL LOSS, ONE EYE
60 yo M with migraine history complains of painful blurry vision in one eye over a few minutes. Image:

77
Acute Angle Closure Glaucoma
Aqueous humor produced in posterior chamber Blockage of normal drainage and circulation to anterior chamber Increasing IOP worsens outflow as iris pushed forward Often mm Hg Lens thickening with age. At midpoint lens and iris touch.

78
Acute Angle Closure Glaucoma
History Sudden onset Precipitant Bending forward Dark environment Illness or sympathetic overdrive Dilating drops Anticholinergic med (even benadryl!)
")
79
Acute Angle Closure Glaucoma
History Pain (eye, head, ear, sinuses, or teeth) Photophobia Vision: blurry, halos or starbursts around lights Nausea / Vomiting Diaphoresis ** May mimic migraine, heart, or GI disease because of systemic complaints delaying diagnosis
 Photophobia. Vision: blurry, halos or starbursts around lights. Nausea / Vomiting. Diaphoresis. ** May mimic migraine, heart, or GI. disease because of systemic complaints. delaying diagnosis.")
80
Exam Decreased visual acuity Red eye Pupil Sluggish mid-dilated
Can be irregular (eg. slightly oval) Corneal haziness Eyeball firm to palpation Hazy from edema. images/glaucoma.JPG
 Corneal haziness. Eyeball firm to palpation. Hazy from edema. images/glaucoma.JPG.")
81
Acute Angle Closure Glaucoma
Exam Anterior chamber Shallow “Shadow sign” Cells and flare By shining a light across the eye from the side, the normally flat iris is uniformly illuminated; any forward bowing will result in illumination only on the side of the iris closest to the light. The iris lying on the other side of the pupil will appear to be in a shadow

82
Acute Angle Closure Glaucoma
Treatment Immediate ophtho consult Treat pain and nausea Avoid dilating drops! Lower IOP iridotomy

83
Acute Angle Closure Glaucoma
Treatment Block aqueous production Beta blocker (eg. Timolol 0.5% 1 drop) Onset 30 mins, peak 1-2 h Caution if asthma, heart failure, heart block CAI (eg. Acetazolamide 500 mg IV/PO/IM) Avoid in sulfa allergy, renal insufficiency Alpha-2 agonist (eg. Apraclonidine 1 drop) Additive effect Nausea so avoid PO
 Onset 30 mins, peak 1-2 h. Caution if asthma, heart failure, heart block. CAI (eg. Acetazolamide 500 mg IV/PO/IM) Avoid in sulfa allergy, renal insufficiency. Alpha-2 agonist (eg. Apraclonidine 1 drop) Additive effect. Nausea so avoid PO.")
84
Topical Eye Drops Nasolacrimal occlusion Eyelid closure
Simple techniques Decrease systemic absorption (by 60%) Increases bioavailability Improving the therapeutic index of topically applied ocular drugs. Zimmerman TJ, et al. Archives of Ophthalmology. 102(4): , 1984. 2-3 MINS, don’t press on the bone. Equally effective, don’t get a lot of added benefit. Look up, put drop into fornix, lower eyelid
 Increases bioavailability. Improving the therapeutic index of topically applied ocular drugs. Zimmerman TJ, et al. Archives of Ophthalmology. 102(4): , MINS, don’t press on the bone. Equally effective, don’t get a lot of added benefit. Look up, put drop into fornix, lower eyelid.")
85
Acute Angle Closure Glaucoma
Treatment Reduce vitreous volume Hyperosmotic agents (eg. Mannitol 1-2 g/kg IV)
")
86
Acute Angle Closure Glaucoma
Treatment Improve aqueous outflow Supine position May help iris fall back posteriorly +/- Miotic agent (eg. Pilocarpine 1 drop q15 mins) Often requires IOP < 40 mm Hg before effective Beware… WORSENS certain AACG types 40 mm Hg, the perfusion pressure of the iris. Common hx, prone, before going to sleep, => miosis => angle closure. BEWARE PILO = OPHTHO SEEING RIGHT AWAY, HOLD OFF, WORSENS CERTAIN AACG TYPES!!!! EG TOPAMAX
 Often requires IOP < 40 mm Hg before effective. Beware… WORSENS certain AACG types. 40 mm Hg, the perfusion pressure of the iris. Common hx, prone, before going to sleep, => miosis => angle closure. BEWARE PILO = OPHTHO SEEING RIGHT AWAY, HOLD OFF, WORSENS CERTAIN AACG TYPES!!!! EG TOPAMAX.")
88
Case 6 ACUTE, PARTIAL LOSS, ONE EYE
30 yo F with recent URI noticed pain and decreased vision in one eye over a few days. No trauma, or N/V Findings: Red eye and painful EOM RAPD+ (N) Acuity (N) Fundoscopy Clues:
 Acuity. (N) Fundoscopy. Clues:")
89
Optic Neuritis Key Points
Relatively common and important cause of visual loss Usually in young adults, esp. caucasian women Commonly first manifestation of MS Presumably autoimmune reaction with demyelinating inflammation of optic nerve F:M 2:1. Up to 75% of women presenting with ON develop MS

90
Optic Neuritis History
May have preceding viral illness, or previous episodes Usually monocular Pain Variable degree Worse on eye movement Vision loss Exacerbated by heat or exercise (Uhthoff phenomenon) Central scotoma or altered color/brightness/depth perception Pain may precede vision loss
 Central scotoma or altered color/brightness/depth perception. Pain may precede vision loss.")
91
Optic Neuritis Exam Visual acuity variable RAPD +
Field defects (central scotoma, altitudinal, arcs) Fundoscopy Often normal (retrobulbar in 2/3) +/- Pale or swollen disc VA (N) to complete loss
 Fundoscopy. Often normal (retrobulbar in 2/3) +/- Pale or swollen disc. VA (N) to complete loss.")
92
Optic Neuritis Management Consult ophtho and neurology Steroids?
Beck RW, Cleary PA, Anderson MM, et al: A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. N Engl J Med 1992;326: Optic Neuritis Study Group: The 5-year risk of multiple sclerosis after optic neuritis: experience of the Optic Neuritis Treatment Trial. Neurology 1997;49: ONTT – RCT. Tx remains controversial – IV steroids for severe or bilateral visual loss? Solumedrol 250 mg QID x 3/7 with oral taper

93
Optic Neuritis Optic Neuritis Treatment Trial (ONTT) Vision
Speeds recovery No effect on visual outcome at 5 yrs AVOID oral steroids due to increased recurrence Multiple Sclerosis IV steroids may help decrease short-term risk of MS No long term protection ONTT – RCT. Tx remains controversial – IV steroids for severe or bilateral visual loss? Solumedrol 250 mg QID x 3/7 with oral taper

94
Summary Eye Pain RAPD Key findings CRAO No Yes
Pale retina, cherry-red spot CRVO +/- Blood and thunder / “Ketchup” fundus RD May have localized field defect, cloudy veil. But suspect on history AION Swollen pale disc, signs of temporal arteritis Acute Angle Closure Glaucoma Painful red eye, hazy cornea, irregular pupil, “shadow sign”, firm globe Optic Neuritis Painful EOM, young female pt

95
Summary Urgency Can wait till AM? ED Treatment CRAO CALL IMMEDIATELY
Only if subacute (Many days old) Orbital massage Lower the IOP CRVO CALL when convenient Yes, wait ASA RD At their discretion Bed rest supine Eye shield AION CALL if TA, severe sx, uncertain dx, can wait if not TA Steroids if TA Acute Angle Closure Glaucoma CALL IMMEDIATELY No Lower the IOP Treat N/V Optic Neuritis Yes, for ophtho AVOID oral steroids Vitreous hemorrhage
 Orbital massage Lower the IOP. CRVO. CALL when convenient. Yes, wait. ASA. RD. At their discretion. Bed rest supine. Eye shield. AION. CALL if TA, severe sx, uncertain dx, can wait if not TA. Steroids if TA. Acute Angle Closure Glaucoma. CALL IMMEDIATELY. No. Lower the IOP. Treat N/V. Optic Neuritis. Yes, for ophtho. AVOID oral steroids. Vitreous hemorrhage.")
96
THANK YOU

97
Traumatic Optic Neuropathy
Mechanism: Hemorrhage of optic nerve sheath Avulsion optic nerve Most cases retrobulbar (no external or ophthalmoscopic evidence of injury) Difficulties: Poor correlation between severity of impact and degree of visual loss. Visual deterioration immediately or after several hours
 Difficulties: Poor correlation between severity of impact and degree of visual loss. Visual deterioration immediately or after several hours.")
98
Traumatic Optic Neuropathy
Management: Controversial Anecdotal evidence for steroids Role and timing of surgical tx unclear (reserved for those who fail to improve, or deteriorate despite steroids?) Acute visual loss and other disorders of the eyes. Laskowits et al. Neurology Clinics of North America. 16 (2) p May 1998.
 Acute visual loss and other disorders of the eyes. Laskowits et al. Neurology Clinics of North America. 16 (2) p May")
Similar presentations
 Waxman MD PhD>")


















