Download presentation
Presentation is loading. Please wait.

1
Rob Sheehan-Dare Leeds Centre for Dermatology
Actinic Keratosis Rob Sheehan-Dare Leeds Centre for Dermatology

2
Pre-Cancerous Lesions
Actinic Keratoses Intra-epithelial Squamous Cell Carcinoma Lentigo maligna Skin Cancer Basal Cell Carcinoma Squamous Cell Carcinoma Melanoma Lymphoma

3
What are Actinic keratoses?
Epidermal dysplasia Associated with UV exposure Sun exposed sites Elderly Outdoor occupations Warmer climates Lighter skin types Immunosuppression

4
What are Actinic keratoses?
Histologically Epidermal cell disorganisation Acanthosis Reduced granular layer Parakeratosis Hyperkeratosis

6
What is risk of malignancy?
?Less than 1:1000 per year Increased by Immunosuppression Increased numbers of lesions Co-factors (radiation, exposure to tar) Prior Squamous cell carcinoma Some lesions resolve spontaneously Most SCC’s are well differentiated
 Prior Squamous cell carcinoma. Some lesions resolve spontaneously. Most SCC’s are well differentiated.")
7
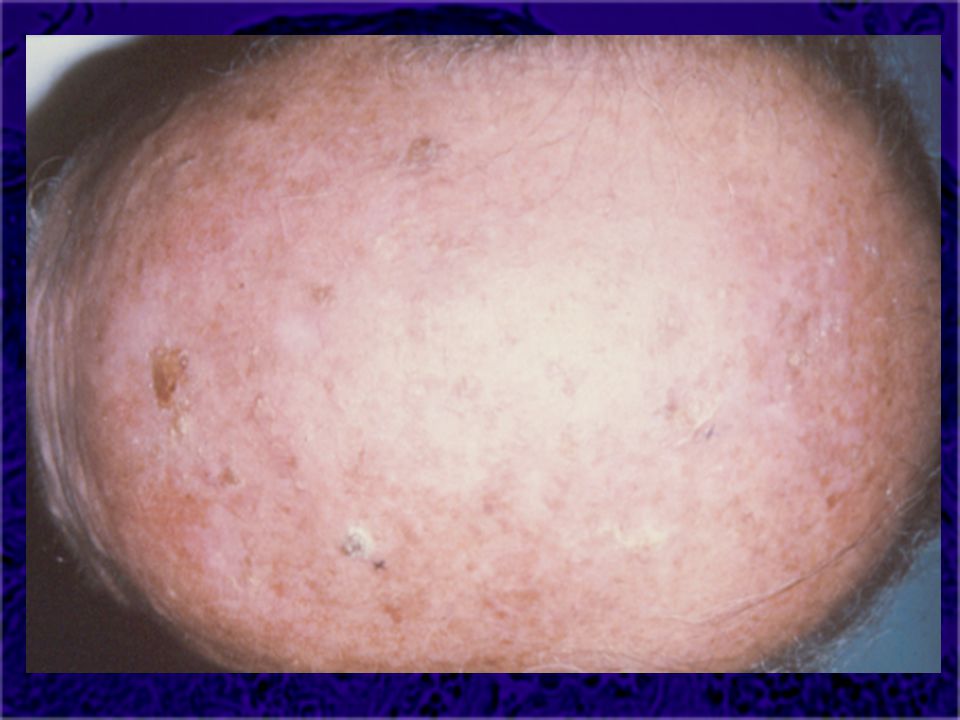
What do they look like? Clinically
Adherent scale (variable but always) Erythema (often) Light pigmentation (sometimes) Merge with surrounding skin Usually not indurated
 Erythema (often) Light pigmentation (sometimes) Merge with surrounding skin. Usually not indurated.")
11
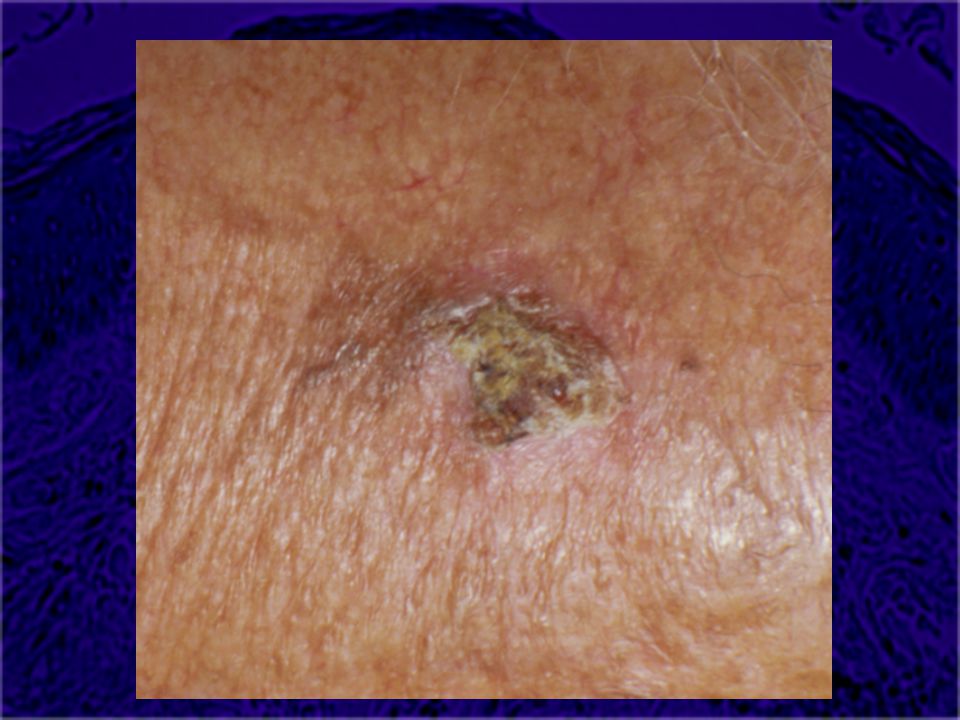
Diagnostic difficulties
Cutaneous horn Hypertrophic actinic keratoses Inflammatory lesions Often in immunosuppressed

12
What to treat Lesions in immunosuppressed patients
Lesions at high risk sites (e.g. lip) Where previous history of SCC Inflamed Actinic keratoses Lesions in younger age group Symptomatic lesions
 Where previous history of SCC. Inflamed Actinic keratoses. Lesions in younger age group. Symptomatic lesions.")
13
How to treat Cryotherapy Curettage & cautery 5-fluorouracil cream
Diclofenac gel Imiquimod cream Photodynamic therapy

14
Cryotherapy Destruction by cold injury Cotton bud or cryospray
20-30 second freeze Moderate pain Immediate blistering Heals in 10 days Suitable for small/few lesions Suitable where compliance poor

17
Curettage and cautery Physical removal/thermal injury
Requires local anaesthesia Moderate pain Eschar Heals in 10 days Suitable for solitary/few lesions Suitable for cryo resistant lesions Suitable for hyperkeratotic lesions Suitable where histology required

18
5-fluorouracil cream Inhibits DNA synthesis by inactivating thymidine synthase 4 weeks treatment Inflammatory reaction (moderate-severe) Little pain Interrupted treatment may be required Suitable for multiple/extensive lesions Suitable for compliant patients
 Little pain. Interrupted treatment may be required. Suitable for multiple/extensive lesions. Suitable for compliant patients.")
19
Diclofenac gel Inhibits Cyclo-oxygenase (COX-2) 8 weeks treatment
Mild-moderate inflammatory reaction No pain Long term benefits uncertain Suitable where intolerance to other treatment

20
Imiquimod cream Toll-like receptor 7 agonist induces apoptosis
4-8 weeks treatment Inflammatory reaction (moderate-severe) Little pain Interrupted treatment may be required Suitable for multiple/extensive lesions Suitable for compliant patients
 Little pain. Interrupted treatment may be required. Suitable for multiple/extensive lesions. Suitable for compliant patients.")
21
Photodynamic therapy ALA induced protoporphyrin IX synthesis sensitizes cells to photodynamic effect 1-2 prolonged treatments Moderate pain Inflammatory reaction (moderate-severe) Heals in 10 days Suitable for multiple/extensive lesions Suitable where compliance poor
 Heals in 10 days. Suitable for multiple/extensive lesions. Suitable where compliance poor.")
22
Treatment summary Cryotherapy small/few lesions
5-fluorouracil larger/multiple lesions Curettage for hyperkeratotic lesions Solaraze for patients with poor tolerance Imiquimod cream or PDT for resistant lesions

23
“They look benign , but keep out of the sun”

Similar presentations







SCC-in-situ (also called) Bowen’s disease.>")















