Download presentation
Presentation is loading. Please wait.

3
Troubleshooting Issues in CVVH Timothy L. Kudelka RN, BSN Pediatric Dialysis Program C.S. Mott Children’s Hospital University of Michigan

4
Where to Begin? As Nephrologist, Intensivist and Nurses we all need to address the issues of troubleshooting CRRT. Many systems are still adapted (pieced) and others now self-contained with simplified operating interface and build-in software. Troubleshooting issues still remain.
 and others now self-contained with simplified operating interface and build-in software. Troubleshooting issues still remain..")
5
Access If you don’t have it you might as well go home. This is the most important aspect of CVVH therapy. Adequacy. Filter life. Increased blood loss. Staff satisfaction.

6
Troubleshooting Access How can you tell if you have a problem before starting? Check placement first, then use syringe to test resistance and blood return. What if you have problems during treatment? Check line for kink, then assess patients position or need for sedation.

7
Access Clotting or sluggish catheter. tPA (tissue plasminogen activator). (Spry et al., Dialysis&Transplantation. Jan. 2001). Normal saline flush. Reason to replace catheter. Clotted catheter with no response to tPA. Exit site blood leakage with no response to pressure dressing. Severe kinked catheter. Bad re-circulation issues.
. Normal saline flush. Reason to replace catheter. Clotted catheter with no response to tPA. Exit site blood leakage with no response to pressure dressing. Severe kinked catheter. Bad re-circulation issues..")
8
Pressures Arterial or outflow pressures High negative pressure = access problem. High positive pressure = filter problem. Moderate to high positive pressure + high return (venous) pressure = access problem. Venous or return pressures Moderate to high positive pressure + high arterial pressure = filter problem. High return pressure + moderate arterial pressure = access
 pressure = access problem. Venous or return pressures Moderate to high positive pressure + high arterial pressure = filter problem. High return pressure + moderate arterial pressure = access.")
9
Anticoagulation None. Heparin. Bolus 10-20 units/kg then infuse at 10-20 units/kg/hr adjust per ACT.(Heparin induced thrombocytopenia). Citrate. Initiate infusion rate at 1.5x the BFR(in mls/hr). Calcium chloride infusion at 0.16x the citrate rate. (Hypocalcemia,metabolic alkalosis.
. Citrate. Initiate infusion rate at 1.5x the BFR(in mls/hr). Calcium chloride infusion at 0.16x the citrate rate. (Hypocalcemia,metabolic alkalosis..")
10
Suggestion Normal saline flush. Flashlight lines and filter. Correct priming technique. Maintain good BFR. Monitor ACT levels (200-250). Quick response to troubleshooting issues.
. Quick response to troubleshooting issues..")
11
Ultrafiltration How much to ultrafiltrate? Net ultrafiltration should be in the range of 1-2 mls/kg/hr. Neonates u/f rate 0.5-1ml/kg/hr.

12
U/F Issues Attention to intravascular volume. Oncotic pressures. U/F controllers. –Infusion pumps up to 30% inaccurate. (Smoyer et al, CRRT1998) Filter size and life.
 Filter size and life..")
13
U/F Issues Accurate assessment is difficult with less room for error in smaller children. –Bed scales. –Frequent weights or weights of U/F in IV controller U/F method. –Measured volume status. –Monitor sHct. –Vasopressor clearance.

14
Membrane Reactions Bradykinin release syndrome Causes of syndrome ACE inhibitors Low blood ph AN-69 membranes have been associated with “Bradykinin release syndrome” (Brophy et al. AJKD 2001)
.")
15
Membrane Reactions What is the common link? –AN-69 membrane. –Blood prime. –Low ph. (Blood bank blood ph). Technique to reduce membrane reaction.
. Technique to reduce membrane reaction..")
16
Membrane Reactions Correct blood from the blood bank. Bypassing the membrane. Bypass maneuver.

17
Bypass Maneuver To view this dialysis clip, go to the Resources References and Procedures folder, then the UNHS Procedures folder on the CD-Rom.

18
Thermal Issues Patient. –Radiant heat methods. Warming blankets. Overhead warmer. Warm water bottles. –Prevention of heat loss. Environmental conditions. Exposure. (Hats on infants, plastic wrap).
..")
19
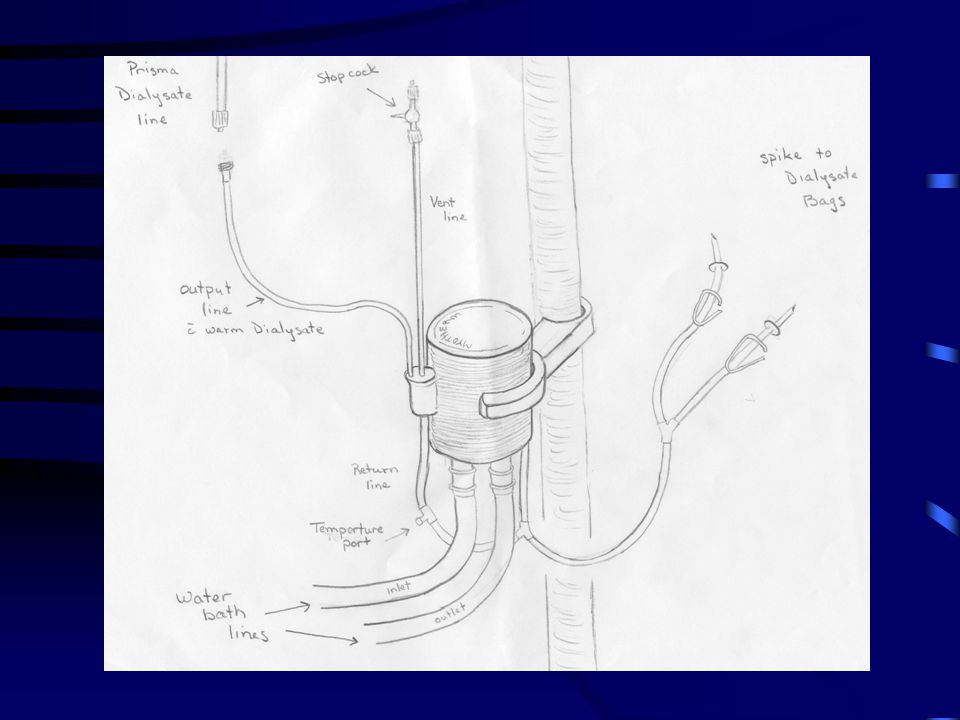
Thermal Issues Circuit –Blood Blood warmers Extracorporeal volume Risk of clotting –Dialysate or replacement fluid Prismatherm ® High volume fluid warmer.

22
Transport Issues Patient that require transport while on CVVH. –Battery pack. –Re-circulation. Blood prime/blood loss. Machine issues. Length of re-circulation. (1-2 hrs).
..")
23
Prescription Need for daily orders. Recommendations on order sheet. Types of solutions. –PD are problematic r/t lactate and high glucose. –Pharmacy made solutions risk of error and expensive. –Bicarbonate based solution-less risk, expense. Nursing orders/labs.

24
Nursing Report Standard forms for documentation. Review of orders. The key to good team work is accurate nursing reporting of problems and troubleshooting techniques.

25
Nursing Training Basic concepts of CRRT. Knowledge of circuit function. Documentation and review of protocols. Troubleshooting issues and techniques. Simulator – for non-stressful practice. One-on-one hands on with experienced staff. Continuous education. Development and implementation of QA tool.

26
Forms Forms available on your CD-ROM

27
Thanks To: Dr. Timothy E. Bunchman MD Dr. Patrick D. Brophy MD University of Michigan Pediatric Dialysis Team. Pediatric Critical Care Nursing. My Wife.

Similar presentations