Download presentation
Presentation is loading. Please wait.

1
© Continuing Medical Implementation …...bridging the care gap Post Myocardial Infarction Pharmacotherapy

2
© Continuing Medical Implementation …...bridging the care gap Post MI Pharmacologic Intervention ASA & Anti-platelet agents Anti-coagulation - blockers ACE inhibitors Dyslipidemic therapy –Statins –Fibrates

3
© Continuing Medical Implementation …...bridging the care gap ASA & Anti-platelet agents Rationale: Ruptured plaque –platelet activation & aggregation –thrombus core –downstream and upstream propagation –cyclical patency and re-occlusion v.s. persistent thrombus formation

4
© Continuing Medical Implementation …...bridging the care gap Mechanism of Anti-platelet Activity Class I - ASA, NSAIDs & sulfinpyrazone –block CO (cyclo-oxygenase) Class II - Dypyridamole –inhibits phosphodiesterase-mediated breakdown of cyclic AMP –prevents platelet aggregation Class III - thienopyridines (ticlopidine&clopidogrel) –block binding of ADP to platelet receptor P2Y12 therby inhibiting adenylyl cyclase Class IV - antibody, peptide & small molecule IIb/IIIA receptor inhibitors
 Class II - Dypyridamole –inhibits phosphodiesterase-mediated breakdown of cyclic AMP –prevents platelet aggregation Class III - thienopyridines (ticlopidine&clopidogrel) –block binding of ADP to platelet receptor P2Y12 therby inhibiting adenylyl cyclase Class IV - antibody, peptide & small molecule IIb/IIIA receptor inhibitors")
5
© Continuing Medical Implementation …...bridging the care gap Antiplatelet Trialists’ Collaboration: Summary Meta-analysis of 145 trials included about 70,000 high-risk patients Anti-platelet drugs reduced risk of composite outcome of ischemic stroke, MI, or vascular death by 27% in high-risk patients The relative odds reduction was consistent: – Over a wide range of clinical manifestations (ischemic cerebrovascular, coronary, and atherosclerotic peripheral arterial disease) –Across subsets of patients at varying risks within specific clinical disorders Antiplatelet Trialists’ Collaboration. BMJ 1994; 308: 81–106.

6
© Continuing Medical Implementation …...bridging the care gap Anti-platelet Trialists’ Collaboration: Results Anti-platelet Trialists’ Collaboration. BMJ 1994; 308: 81–106. Category of trial Prior stroke/TIA Acute MI Patients with stroke, MI, or vascular death (%) 25 20 Antiplatelet therapy Control 15 10 5 0 Prior MI Other high risk All high risk 22% odds reduction 29% odds reduction 25% odds reduction 32% odds reduction 27% odds reduction
 Antiplatelet therapy Control Prior MI Other high risk All high risk 22% odds reduction 29% odds reduction 25% odds reduction 32% odds reduction 27% odds reduction.")
7
© Continuing Medical Implementation …...bridging the care gap ASA: Efficacy Relative- risk reduction ASA 25% Antiplatelet Trialists’ Collaboration. BMJ 1994; 308: 81–106. ASA reduces the risk of stroke, MI, or vascular death by 25% relative to placebo

8
© Continuing Medical Implementation …...bridging the care gap

12
Unresolved Questions Use in all comers with UAP/NSTEMI? With IIB/IIA inhibitors? How long to use –With PCI? –Without PCI? Cost efficacy? Peri-CABG discontinuation?

13
© Continuing Medical Implementation …...bridging the care gap Oral anticoagulant therapy in patients with coronary artery disease: a meta-analysis.Anand SS; Yusuf S JAMA 1999 Dec 1;282(21):2058-67 44 Trials-23,397 patients oral anticoagulation for at least three months acute MI, unstable angina, CABG high intensity (INR 2.8-4.8) and moderate intensity (INR 2-3) Odds Ratio –death: 22 & 18% –MI: 42 & 52% –CVA: 63 & 53% Bleeding: 6 & 2.4 X No difference in death, MI or CVA v.s. ASA

14
© Continuing Medical Implementation …...bridging the care gap Anti-coagulation Indication post MI: LV thrombus or aneurysm LVEF < 30% CHF History of thrombo-embolism Chronic atrial fibrillation-continue indefinitely

15
© Continuing Medical Implementation …...bridging the care gap LV thrombus or aneurysm Up to 40% large Q-anterior MIs –less in smaller MIs –less post-thrombolysis Odds ratio 0.14 for embolization with anti- coagulation for 6 months v.s no anticoagulation –Embolic potential, prevention and management of mural thrombus complicating anterior myocardial infarction: a meta-analysis.Vaitkus PT; Barnathan ES J Am Coll Cardiol 1993 Oct;22(4):1004-9.
:")
16
© Continuing Medical Implementation …...bridging the care gap SELECTED RANDOMIZED TRIALS OF - BLOCKER THERAPY ADMINISTERED DURING AND AFTER AMI - Blockers Agent# PatientsDurationRRR of Death P Value During MI ISIS IAtenolol160277 days0.85< 0.04 MIAMIMetoprolol577815 days0.870.29 TIMI IIBMetoprolol14346 days1.00.98 After MI NorwegianTimolol188433 months0.61< 0.001 BHATPropranolol383725 months0.72< 0.005

17
ACC/AHA Guidelines

18
© Continuing Medical Implementation …...bridging the care gap Rate of heart failure and 1-year survival for older people receiving low-dose ß-blocker therapy after myocardial infarction. Lancet 2000; 356: 639 - 644 Paula A Rochon, Jack V Tu, Geoffrey M Anderson, Jerry H Gurwitz, Jocalyn P Clark, Paula Lau, John Paul Szalai, Kathy Sykora, C David Naylor 13 623 patients aged 66 years or older discharged from hospital post myocardial infarction No ß-blocker therapy vs received low, standard, or high doses. Of 8232 patients with no previous history of heart failure –ß-blocker therapy was associated with a 43% reduction in subsequent admission for heart failure

19
© Continuing Medical Implementation …...bridging the care gap Rate of heart failure and 1-year survival for older people receiving low-dose ß-blocker therapy after myocardial infarction. Lancet 2000; 356: 639 - 644 Of 4681(57%) patients prescribed ß-blockers –Risk of admission was greater in the high- dose than in the low-dose group !!!!! –Iin the cohort, 2326 (17·1%) died by 1 year –Adjusted risk ratio 0·57 [95% CI 0·48-0·69] compared with patients not dispensed this therapy Compared with those not dispensed ß-blocker therapy, the adjusted risk ratio for mortality was lower for all three doses –low 0·40 [0·34-0·47] –standard 0·36 [0·31-0·42] –high 0·43 [0·33-0·56]
 patients prescribed ß-blockers –Risk of admission was greater in the high- dose than in the low-dose group !!!!. –Iin the cohort, 2326 (17·1%) died by 1 year –Adjusted risk ratio 0·57 [95% CI 0·48-0·69] compared with patients not dispensed this therapy Compared with those not dispensed ß-blocker therapy, the adjusted risk ratio for mortality was lower for all three doses –low 0·40 [0·34-0·47] –standard 0·36 [0·31-0·42] –high 0·43 [0·33-0·56].")
20
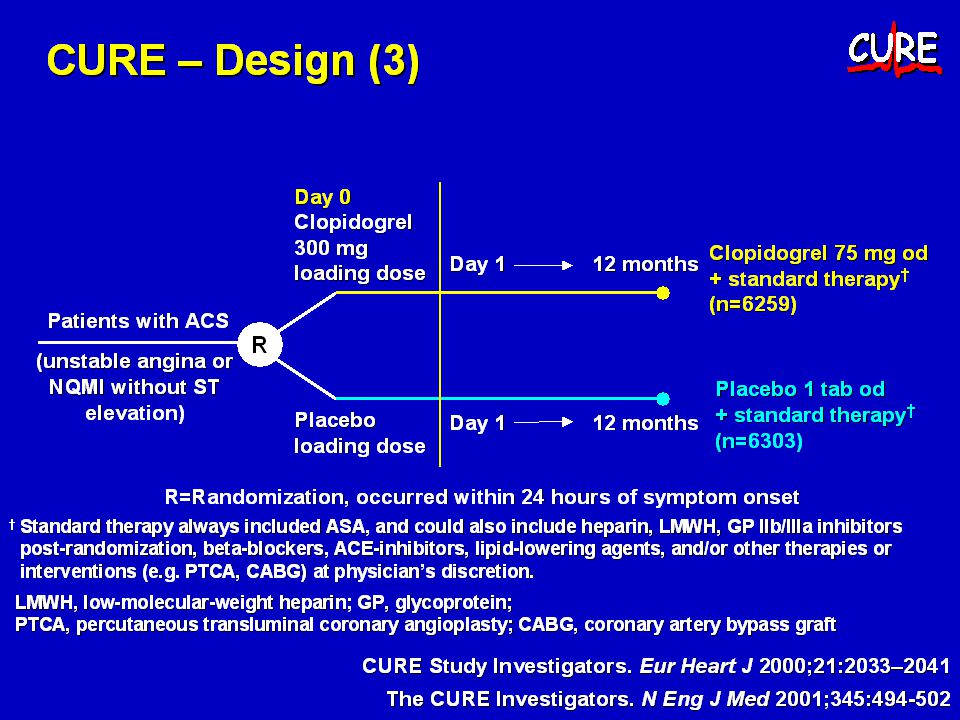
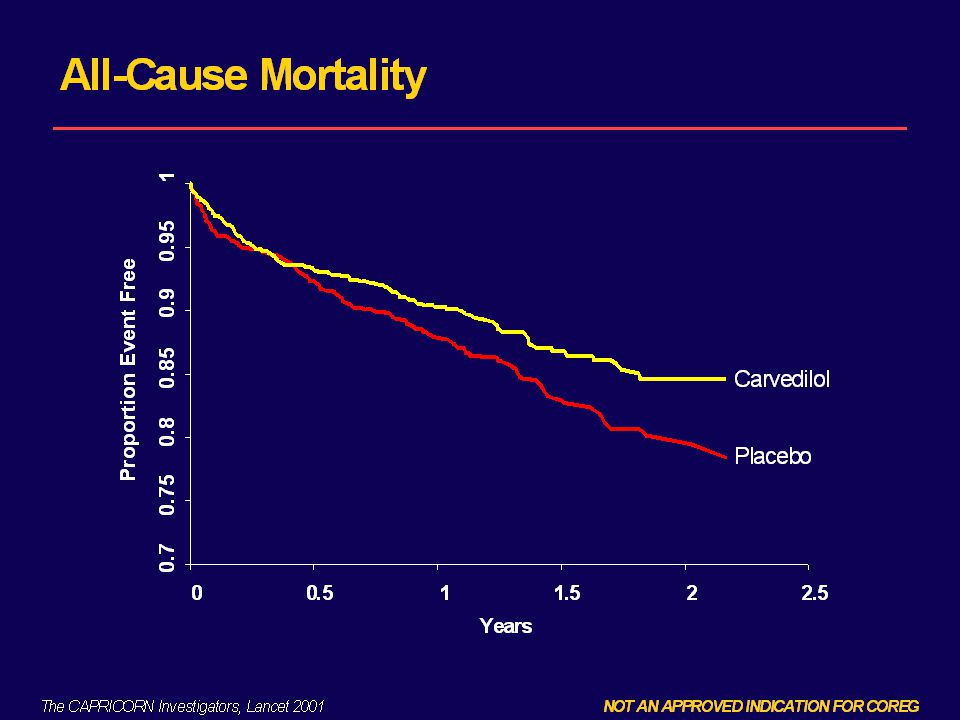
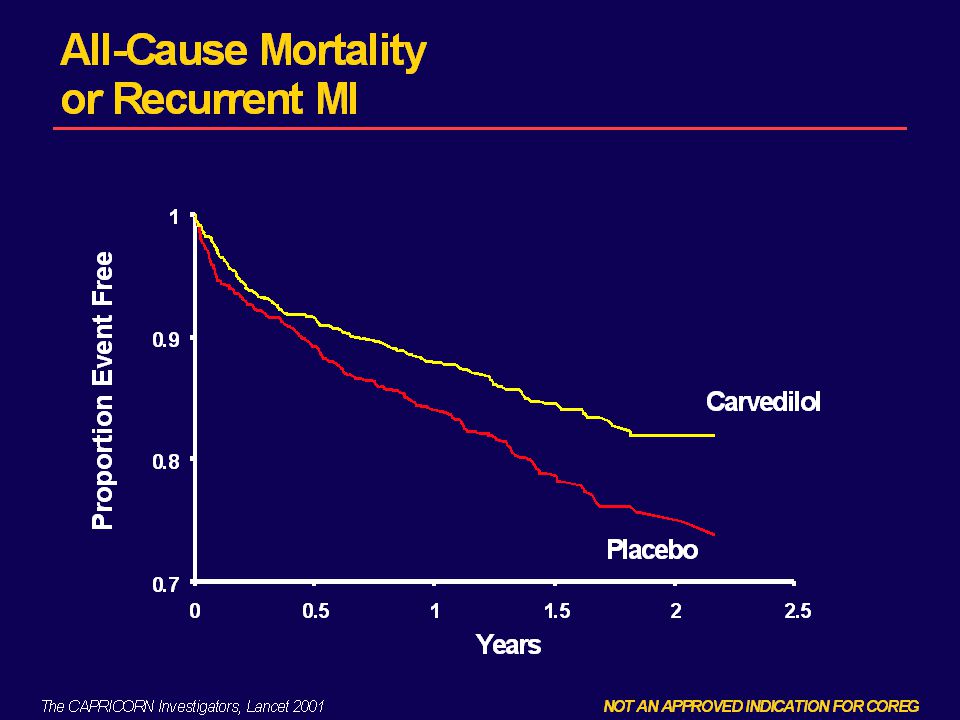
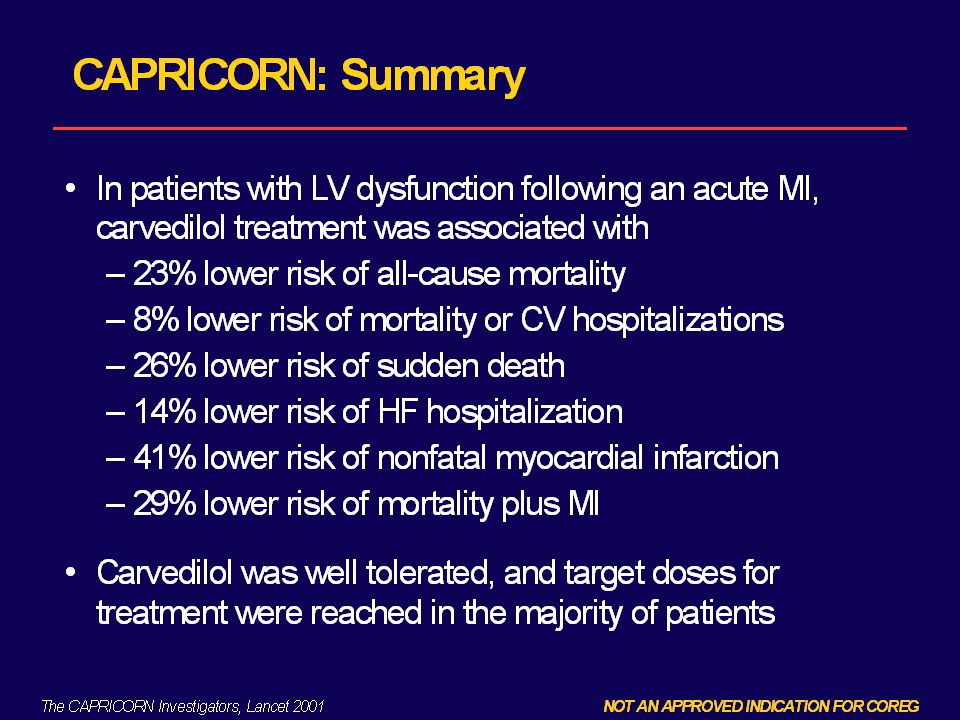
© Continuing Medical Implementation …...bridging the care gap CAPRICORN

21
© Continuing Medical Implementation …...bridging the care gap

26
ACE inhibitors

28
SELECTED RANDOMIZED TRIALS OFACE INHIBITOR THERAPY ADMINISTERED DURING AND AFTER AMI TrialAgent# PatientsDurationRRR of Death P Value During MI & 4-6 weeks after ISIS – 4Captopril5805035 days0.930.02 GIZZI – 3Lisinopril1939442 days0.880.03 Consensus IIEnalaprilat609041-180 days 1.110.26 Post MI LV Dysfunction SAVECaptopril223142 mo.0.810.02 AIRERamipril200615 mo.0.730.002 TRACETrandola- pril 174924-50 mo.0.78< 0.001

29
ACC/AHA Guidelines

33
© Continuing Medical Implementation …...bridging the care gap

38
Statins Post MI

39
© Continuing Medical Implementation …...bridging the care gap Major Statin Trials TrialStatinCholesterol at baseline Total MI or CV Death Secondary Prevention Control % ARRNNT 4SSimva6.721.58.013 LIPIDPrava5.617.23.926 CAREPrava5.413.72.737 Primary Prevention WOSCOPS Prava7.08.42.638 AFCAPS Lova5.73.61.471

40
ACUTE MI GUIDELINES 11/96 Drug Rx Peri MI: Meta-Analyses Beta blocker during MI Beta blocker post MI ACEI during MI ACEI post MI if LV dysfxn Nitrates during MI Ca ++ blockers Magnesium Lidocaine Class I Antiarrhythmics NumberRR Deathp value 28,970 24,298 100,963 5,986 81,908 20,342 61,860 9,155 6,300.87 (.77-.98).77 (.70-.84).94 (.89-.98).78 (.70-.86).94 (.90-.99) 1.04 (.95-1.14) 1.02 (.96-1.08) 1.38 (.98-1.95) 1.21 (1.01-1.44) 0.02 <0.001 0.006 <0.001 0.03 0.41 >0.05 0.04 NEJM 335:1662, 1996
.77 ( ).94 ( ).78 ( ).94 ( ) 1.04 ( ) 1.02 ( ) 1.38 ( ) 1.21 ( ) 0.02 < < > NEJM 335:1662, 1996")
41
© Continuing Medical Implementation …...bridging the care gap Cardiac Rehabilitation Programs Definition –“the enhancement and maintenance of cardiovascular health through individualized programs designed to optimize physical, psychological, social, vocational and emotional status”. 1 May include multifactorial secondary prevention – defined as “the sum total of all interventions, both physiological and behavioral, designed to favorably modify an individual’s lifestyle, and enhance adherence and compliance with long-term behaviors compatible with minimizing disease progression”. 1

42
© Continuing Medical Implementation …...bridging the care gap Benefits 20% reduction in mortality after a three- year follow-up. 16 Improvement in exercise tolerance, blood lipid levels, and psychosocial well-being. 2 A significantly lower incidence of re- hospitalization and visits to the emergency department at three and 12 months compared with controls. 29

43
© Continuing Medical Implementation …...bridging the care gap Needs Only 10-20% of appropriate patients in US currently participate in formal Rehab Secondary prevention population 1999 in Ontario A.Post event (3 o prevention)-95,699 B.Pre-event- 332,362 High risk primary prevention population 2,140,529
-95,699 B.Pre-event- 332,362 High risk primary prevention population 2,140,529")
44
© Continuing Medical Implementation …...bridging the care gap System requirements Assuming –40% participation from secondary prevention A) group –20% participation from secondary prevention B) group Systematic capacity required June 2002 100,000
 group –20% participation from secondary prevention B) group Systematic capacity required June ,000")
45
© Continuing Medical Implementation …...bridging the care gap CCN Network Model Coordinating sites –Regional hub in population areas of > 500,000 In-patient sites –All hospitals with in-patient cardiac services Out-patient sites –Hospital or community based provider –Phase 2&3 care Maintenance sites –Hospital or community based provider –Phase 4 care

46
© Continuing Medical Implementation …...bridging the care gap Guide for Comprehensive Cardiovascular Risk Reduction

47
© Continuing Medical Implementation …...bridging the care gap We can’t do it alone

48
© Continuing Medical Implementation …...bridging the care gap Conclusions Multidisciplinary intervention indicated in all post MI patients Patient education is key to empowerment and motivation Diet, lifestyle,exercise form core component of 2 o prevention strategy In hospital timeframes limits educational opportunity

49
© Continuing Medical Implementation …...bridging the care gap Conclusions Optimization of 2 o prevention pharmacotherapy provides opportunity to recapture lost morbidity and mortality benefit Long term follow-up is necessary to ensure compliance Cardiac rehabilitation (formal or informal) creates the framework for optimal prevention Resources are currently inadequate to meet the demonstrated need
 creates the framework for optimal prevention Resources are currently inadequate to meet the demonstrated need")
Similar presentations







 Clinical events (morbidity.>")








 vs. placebo FU 5 years total cholesterol 25%; LDL.>")
>")








 and Clopidogrel (Plavix™) Benedict R. Lucchesi, M.D., Ph.D. Department of Pharmacology University of Michigan Medical School.>")