Download presentation
Presentation is loading. Please wait.

1
1 Presentor: R3 彭元宏 Supervisor: 李苑如 醫師

2
Introduction SINCE its introduction in 1980, shock wave lithotripsy has become a common treatment for most renal and ureteral stones. The experience of SWL at several centers resulted in positive urine culture and sepsis after lithotripsy in approximately 5% and 1% of patients To avoid infectious complications in these patients, prophylactic antibiotics were usually administered

3
Introduction The two largest academic associations EAU guideline: Does not recommend the routine use of antibiotic prophylaxis, except for patients with infection risk such as the presence of an indwelling stent, infectious stones, indwelling catheter or nephrostomy tube.

4
Introduction AUA guideline: recommended - Prophylaxis reduced postoperative bacteriuria rates from a median of 5.7% to 2.1%. Pearle et al. Antimicrobial prophylaxis prior to shock wave lithotripsy in patients with sterile urine before treatment: a meta-analysis and cost-effectiveness analysis. Urology 1997

5
Aim To assess the effect of pretreatment antibiotics in patients undergoing SWL, A systematic review and meta-analysis comparing antibiotic prophylaxis with placebo or no treatment in patients with sterile urine before treatment.

6
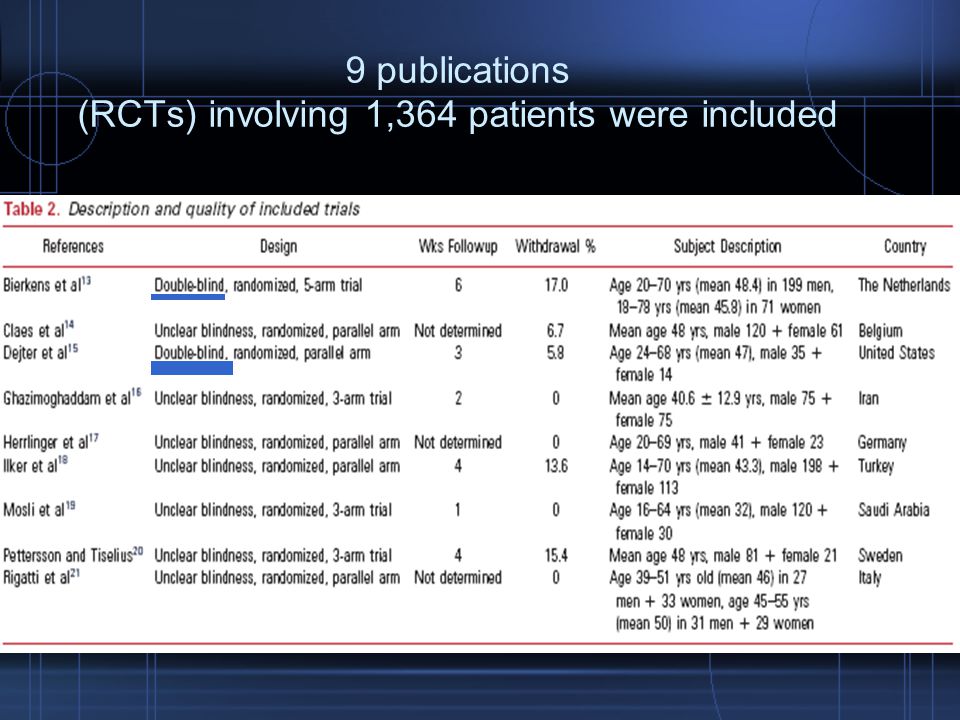
Search Pubmed, Embase (from 1980-2011) Key words: lithotripsy, shock wave lithotripsy, antibiotic, bacteriuria, infection and randomized controlled trial (multiple synonyms for each term) 9 publications (RCTs) involving 1,364 patients
 Key words: lithotripsy, shock wave lithotripsy, antibiotic, bacteriuria, infection and randomized controlled trial (multiple synonyms for each term) 9 publications (RCTs) involving 1,364 patients")
7
Search Inclusion criteria: - adult patients with renal or ureteral calculi with sterile urine before treatment. - SWL was suitable for all patients Exclusion criteria: - patients who had inadvertently taken antibiotics postoperatively - patients with a history of antibiotic administration within the last 10 days before SWL

8
Statistical analysis Relative risk with 95% CI Fixed effects method: not significant heterogeneity Random effects method:significant heterogeneity Heterogeneity assessment: I 2 test and significance set at p<0.05

9
Result

10
9 publications (RCTs) involving 1,364 patients were included
 involving 1,364 patients were included")
13
Fever Positive urine culture Urinary tract infection Preoperative ureteral catheter

14
Fever The difference in fever rate between the 2 groups was not significant (random effects model RR: 0.39, 95% CI 0.07–2.36, p= 0.31)
")
15
Positive urine culture – short term(<2 weeks) No significant differences between the 2 groups in the rate of short-term positive UC (RR 0.67, 95% CI 0.44–1.02, p = 0.06)
 No significant differences between the 2 groups in the rate of short-term positive UC (RR 0.67, 95% CI 0.44–1.02, p = 0.06)")
16
The rate of midterm positive UC (RR 1.24, 95% CI 0.59–2.61, p=0.58) The overall rate of positive UC (RR:0.77, 95% CI 0.54–1.11, p = 0.17) Positive urine culture – mid-term(2wk-2mons)
 The overall rate of positive UC (RR:0.77, 95% CI 0.54–1.11, p = 0.17) Positive urine culture – mid-term(2wk-2mons)")
17
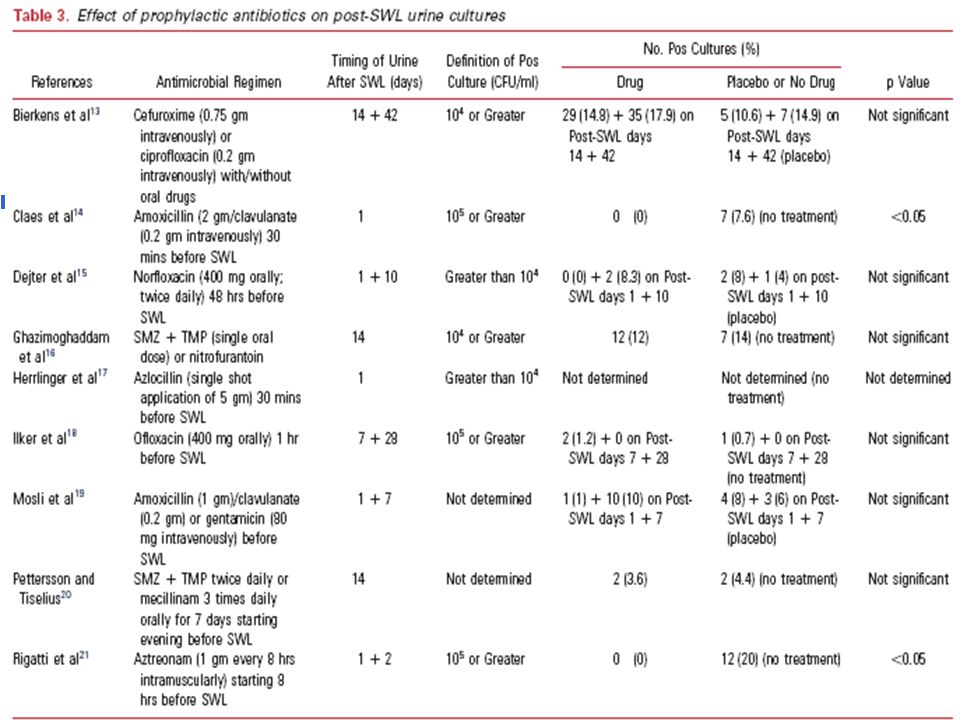
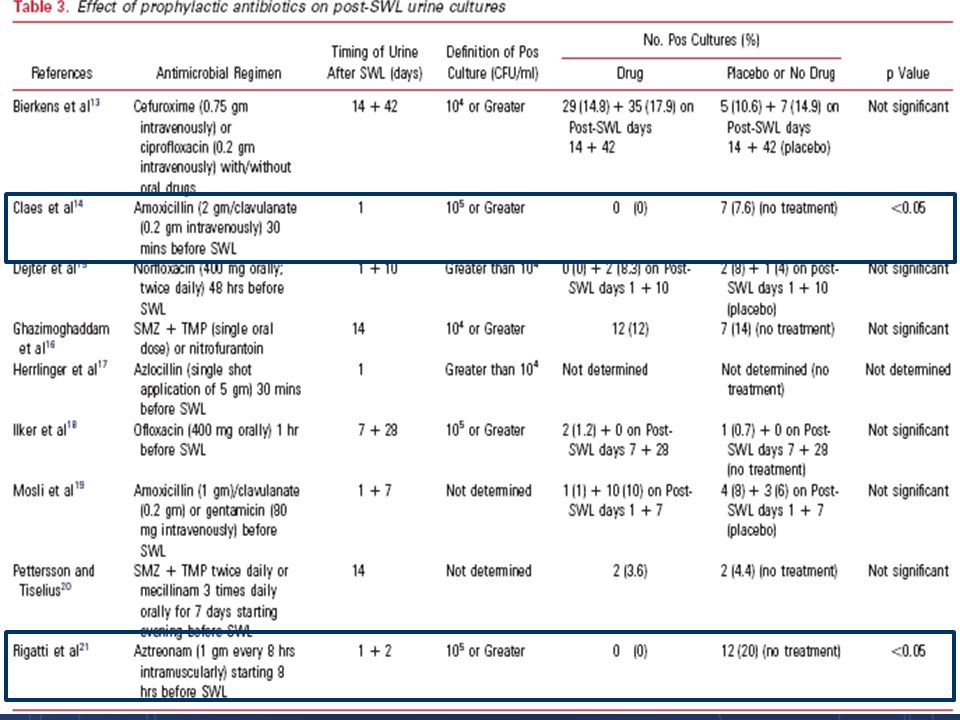
UTI Incidence of positive urine culture(according to 8 RCTs) - Abx prophylaxis: 0% - 17.9% - No medication: 0.7% - 20.0% Definition of UTI: Symptoms + positive bacterial examinaion(bacturia or positive UC) Incidence of UTI: - Abx prophylaxis: 0% - 12% - No medication: 0% - 14%
 - Abx prophylaxis: 0% % - No medication: 0.7% % Definition of UTI: Symptoms + positive bacterial examinaion(bacturia or positive UC) Incidence of UTI: - Abx prophylaxis: 0% - 12% - No medication: 0% - 14%")
18
UTI

19
Preoperative catheter

20
Discussion

21
Antibiotic prophylaxis involves a brief course of antibiotics administered before or at the start of a diagnostic and/or therapeutic intervention, and it is used to minimize possible infectious complications The role of prophylactic antibiotics in patients undergoing SWL for urinary calculi has not been well-defined

22
Discussion EAU guideline: Does not recommend the routine use of antibiotic prophylaxis, except for patients with infection risk such as the presence of an indwelling stent, infectious stones, indwelling catheter or nephrostomy tube. AUA guideline: recommended - Prophylaxis reduced postoperative bacteriuria rates from a median of 5.7% to 2.1%. (Urology 1997)
.")
23
Discussion Pearle and Roehrborn in 1997 included 8 RCTs, 5 RCTs was included to our meta-analysis. Another 3 RCTs excluded. 3 excluded RCTs: the incomplete description of methodology and results. 2 RCTs released after their meta-analysis was compiled and 2 RCTs not detected in their literature search

25
Discussion Released before 1990 With the remarkable technical developments and medical achievements in urology during the last 20 years, older studies from the 1980s might have partly lost their relevance

26
Limitations Most articles in this review were old, released before the year 2000 The numbers of participants in the RCTs were small(Patient numbers: 60-300) There was a trend toward the reduction of overall UTI incidence (RR 0.54, 95% CI 0.29 –1.01, p=0.05) and a short-term positive UC rate (RR 0.67, 95% CI 0.44 – 1.02, p=0.06)
 There was a trend toward the reduction of overall UTI incidence (RR 0.54, 95% CI 0.29 –1.01, p=0.05) and a short-term positive UC rate (RR 0.67, 95% CI 0.44 – 1.02, p=0.06)")
27
Conclusion Prophylaxis could neither decrease the rate of fever and positive urine culture, nor the incidence of UTI Antibiotic prophylaxis appears to be unnecessary for SWL

28
Thanks for your attension 28

Similar presentations

>")

















