Download presentation
Presentation is loading. Please wait.

1
GI Bleeding Mark Topazian, M.D. December 16, 2010

2
Has responded with a disclosure Will discuss off-label/investigative use(s): Sandoz, Ethicon Octreotide, Dermabond Critical Care Grand Rounds Disclosure Summary Mark D. Topazian, MD

3
Planning committee members who have nothing to disclose: Sean M. Caples, DO, Co-Director Juan N. Pulido, MD, Co-Director J. Christopher Farmer, MD Kim Jones, Program Coordinator Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo School of CME), must ensure balance, independence, objectivity and scientific rigor in its educational activities. Course Director(s), Planning Committee Members, Faculty, and all others who are in a position to control the content of this educational activity are required to disclose all relevant financial relationships with any commercial interest related to the subject matter of the educational activity. Safeguards against commercial bias have been put in place. Faculty also will disclose any off label and/or investigational use of pharmaceuticals or instruments discussed in their presentation. Disclosure of this information will be published in course materials so those participants in the activity may formulate their own judgments regarding the presentation. Critical Care Grand Rounds Disclosure Summary Continued
, must ensure balance, independence, objectivity and scientific rigor in its educational activities. Course Director(s), Planning Committee Members, Faculty, and all others who are in a position to control the content of this educational activity are required to disclose all relevant financial relationships with any commercial interest related to the subject matter of the educational activity. Safeguards against commercial bias have been put in place. Faculty also will disclose any off label and/or investigational use of pharmaceuticals or instruments discussed in their presentation. Disclosure of this information will be published in course materials so those participants in the activity may formulate their own judgments regarding the presentation. Critical Care Grand Rounds Disclosure Summary Continued.")
4
Learning Objectives Identify predictors of morbidity and mortality in patients with acute gastrointestinal hemorrhage Describe the management approach to gastrointestinal hemorrhage Understand the evidence basis for pharmacologic and endoscopic therapies Review important recent developments in this field

5
GI Bleeding is an important clinical problem Incidence: 100/100,000/year Mortality: 3% to 10% Silverstein GIE 2002; Cutler DDS 1981; Lanas AJG 2009

6
Risk stratification Pharmacology Interventional Strategies Prevention

7
Risk stratification Pharmacology Interventional Strategies Prevention Rebleeding Mortality Early intervention

8
Risk stratification Pharmacology Interventional Strategies Prevention Rebleeding Mortality Early intervention PPI Octreotide ASA/clopidigrel

9
Risk stratification Pharmacology Interventional Strategies Prevention Rebleeding Mortality Early intervention PPI Octreotide ASA/clopidigrel Endoscopy Angiography

10
Risk stratification Pharmacology Interventional Strategies Prevention Rebleeding Mortality Early intervention PPI Octreotide ASA/clopidigrel Endoscopy Angiography Primary Secondary

11
Predictors of re-bleeding and death Variceal Bleeding Size of the initial bleed Severity of liver disease Infection (SBP) Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata
 Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata")
12
Predictors of re-bleeding and death Variceal Bleeding Size of the initial bleed Severity of liver disease Infection (SBP) Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata
 Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata")
13
Predictors of re-bleeding and death Variceal Bleeding Size of the initial bleed Severity of liver disease Infection (SBP) Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata
 Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata")
14
Predictors of re-bleeding and death Variceal Bleeding Size of the initial bleed Severity of liver disease Infection (SBP) Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata
 Non-Variceal Bleeding Size of the initial bleed Age > 65 years Comorbidities Endoscopic stigmata")
15
Schiller, Truelove, Williams. Hematemesis and melena with special reference to factors affecting outcome, BMJ 1970

16
Bedside estimation of hypovolemia No bedside test is reliable for diagnosis of moderate acute blood loss Supine tachycardia and/or hypotension are specific but insensitive (often absent) in severe acute blood loss (630-1150 ml) 2 signs are sensitive and specific for diagnosis of severe acute blood loss: – Postural pulse increment ≥ 30 bpm – Severe postural dizziness (unable to stand for VS) McGee JAMA 1999
 in severe acute blood loss ( ml) 2 signs are sensitive and specific for diagnosis of severe acute blood loss: – Postural pulse increment ≥ 30 bpm – Severe postural dizziness (unable to stand for VS) McGee JAMA 1999")
17
Bedside diagnosis of hypovolemia No bedside test is reliable for diagnosis of moderate acute blood loss Supine tachycardia and/or hypotension are specific but insensitive (often absent) in severe acute blood loss (630-1150 ml) 2 signs are sensitive and specific for diagnosis of severe acute blood loss: – Postural pulse increment ≥ 30 bpm – Severe postural dizziness (unable to stand for VS) McGee JAMA 1999
 in severe acute blood loss ( ml) 2 signs are sensitive and specific for diagnosis of severe acute blood loss: – Postural pulse increment ≥ 30 bpm – Severe postural dizziness (unable to stand for VS) McGee JAMA 1999")
18
Bedside diagnosis of hypovolemia No bedside test is reliable for diagnosis of moderate acute blood loss Supine tachycardia and/or hypotension are specific but insensitive (often absent) in severe acute blood loss (630-1150 ml) 2 signs are sensitive and specific for diagnosis of severe acute blood loss: – Postural pulse increment ≥ 30 bpm – Severe postural dizziness (unable to stand for VS) McGee JAMA 1999
 in severe acute blood loss ( ml) 2 signs are sensitive and specific for diagnosis of severe acute blood loss: – Postural pulse increment ≥ 30 bpm – Severe postural dizziness (unable to stand for VS) McGee JAMA 1999")
19
Melena, hematemesis, hematochezia Melena implies acute loss of at least 250 ml blood in the UGI tract – Pace of melena Hematemesis implies rapid UGI bleeding – Fatality rate doubled c/w melena Hematochezia is usually due to LGIB – May be due to duodenal ulcer Schiff AJMS 1942, Schiller 1970, Jensen 2005, and others

20
NG aspirate and lavage NG aspirate for diagnosis of upper vs. lower GI bleed – poor specificity (42% - 84%) and sensitivity (54% - 91%) NG lavage for prognosis of UGI bleeding – Failure to clear with > 10 liters lavage predicts ongoing bleeding – Endoscopic findings are better prognosticators Complication rate of NG tube placement is 1% – NG aspiration may promote rebleeding from varices Palamadessi SAEM 2010
 and sensitivity (54% - 91%) NG lavage for prognosis of UGI bleeding – Failure to clear with > 10 liters lavage predicts ongoing bleeding – Endoscopic findings are better prognosticators Complication rate of NG tube placement is 1% – NG aspiration may promote rebleeding from varices Palamadessi SAEM")
21
Blatchford, Lancet 2000

22
Blatchford Score Low risk All of the following: Normal pulse and BP Near-normal BUN and Hb No liver, heart disease High risk 2 or more of the following: BUN > 30 mg/dL Hb < 10 Hypotension Hepatic or cardiac disease

23
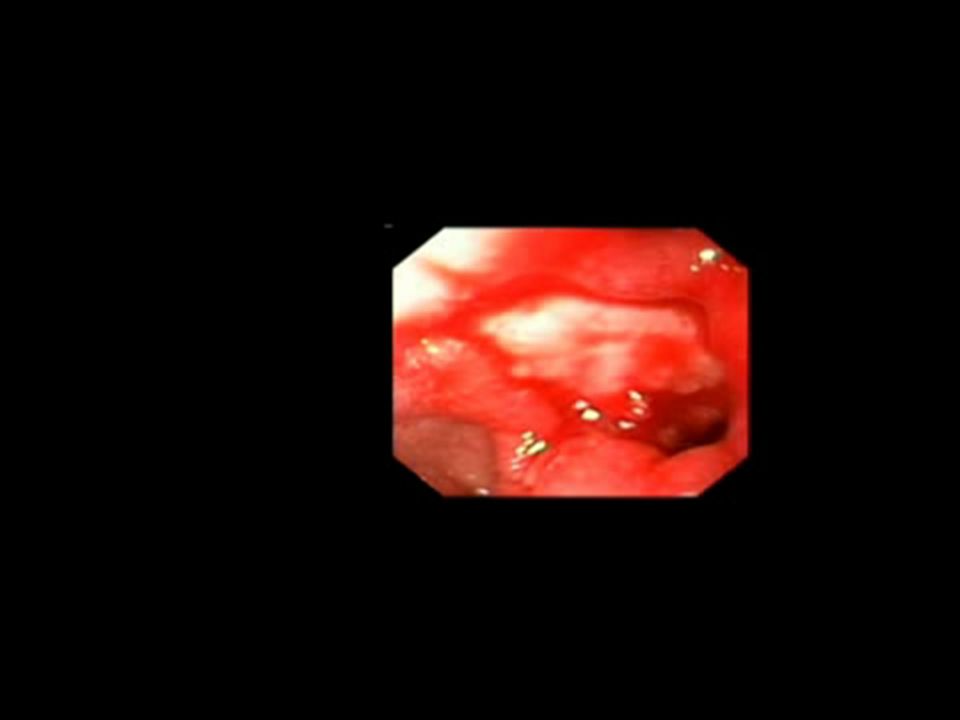
Endoscopic stigmata in peptic ulcers Clean-based ulcer Flat spot Visible vessel Adherent clot Active bleeding

24
Endoscopic stigmata in peptic ulcers Clean-based ulcer Flat spot Visible vessel Adherent clot Active bleeding Rebleeding: 3%

25
Endoscopic stigmata in peptic ulcers Clean-based ulcer Flat spot Visible vessel Adherent clot Active bleeding Rebleeding: 10%

26
Endoscopic stigmata in peptic ulcers Clean-based ulcer Flat spot Visible vessel Adherent clot Active bleeding Rebleeding: 50%

27
Endoscopic stigmata in peptic ulcers Clean-based ulcer Flat spot Visible vessel Adherent clot Active bleeding Rebleeding: 25% - 40%

28
Endoscopic stigmata in peptic ulcers Clean-based ulcer Flat spot Visible vessel Adherent clot Active bleeding Rebleeding: 90%

29
PPI therapy PPI before endoscopy Fewer endoscopic stigmata No effect on rebleeding, surgery, or mortality Sreeharan (Cochrane) 2010; Wu WJG 2010; Wang AIM 2010 ; and others
 2010; Wu WJG 2010; Wang AIM 2010 ; and others")
30
PPI therapy PPI before endoscopy Fewer endoscopic stigmata No effect on rebleeding, surgery, or mortality PPI after endoscopy Improves outcomes in pts requiring endoscopic Rx No difference between high and regular dose Rx Sreeharan (Cochrane) 2010; Wu WJG 2010; Wang AIM 2010 ; and others
 2010; Wu WJG 2010; Wang AIM 2010 ; and others")
31
PPI therapy PPI before endoscopy Fewer endoscopic stigmata No effect on rebleeding, surgery, or mortality PPI after endoscopy Improves outcomes in pts requiring endoscopic Rx No difference between high and regular dose Rx Sreeharan (Cochrane) 2010; Wu WJG 2010; Wang AIM 2010 ; and others PPI dose 1-4x daily dose vs. 2-6x daily dose IV plus cont. infusion

32
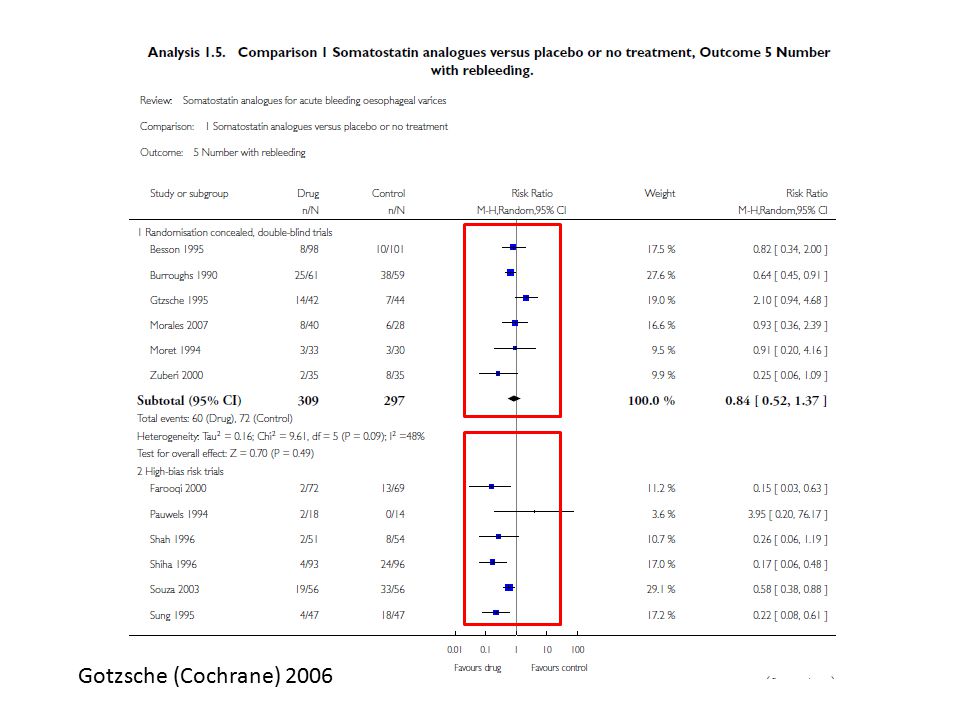
Octreotide therapy Gotzsche (Cochrane) 2006; and others Mechanism Prevents post-prandial increase in mesenteric blood flow
 2006; and others Mechanism Prevents post-prandial increase in mesenteric blood flow")
33
Octreotide therapy Octreotide vs. placebo Less transfusion (0.7 units) Less failure of initial endoscopic Rx (RR 0.7) Balloon tamponade rare No difference in rebleeding or mortality Gotzsche (Cochrane) 2006; and others Mechanism Prevents post-prandial increase in mesenteric blood flow
 Less failure of initial endoscopic Rx (RR 0.7) Balloon tamponade rare No difference in rebleeding or mortality Gotzsche (Cochrane) 2006; and others Mechanism Prevents post-prandial increase in mesenteric blood flow.")
34
Octreotide therapy Octreotide vs. placebo Less transfusion (0.7 units) Less failure of initial endoscopic Rx (RR 0.7) Balloon tamponade rare No difference in rebleeding or mortality How to use octreotide Patients with suspected variceal hemorrhage Bolus of 0 to 50 mcg, infusion of 25 – 250 mcg/hr Begin before endoscopy and continue for 3 – 5 days Gotzsche (Cochrane) 2006; and others Mechanism Prevents post-prandial increase in mesenteric blood flow
 Less failure of initial endoscopic Rx (RR 0.7) Balloon tamponade rare No difference in rebleeding or mortality How to use octreotide Patients with suspected variceal hemorrhage Bolus of 0 to 50 mcg, infusion of 25 – 250 mcg/hr Begin before endoscopy and continue for 3 – 5 days Gotzsche (Cochrane) 2006; and others Mechanism Prevents post-prandial increase in mesenteric blood flow.")
35
Gotzsche (Cochrane) 2006
 2006")
37
Other Drug Rx for Portal HTN Vasopressin – Absence of controlled data – Systemic risks Vasopressin analogues – Terlipressin is effective in European trials Beta blockers – Not used in the acute setting – Decrease risk of rebleeding after discharge

38
Antibiotics Infectious complications increase mortality in cirrhotics Numerous controlled trials of antibiotic Rx Chavez-Tapia (Cochrane), 2010
, 2010")
39
Antibiotics Infectious complications increase mortality in cirrhotics Numerous controlled trials of antibiotic Rx Improvements with antibx: Bacterial infections (RR 0.36) Rebleeding (RR 0.53) Mortality (RR 0.79) Chavez-Tapia (Cochrane), 2010
 Rebleeding (RR 0.53) Mortality (RR 0.79) Chavez-Tapia (Cochrane), 2010")
40
Antibiotics Infectious complications increase mortality in cirrhotics Numerous controlled trials of antibiotic Rx Improvements with antibx: Bacterial infections (RR 0.36) Rebleeding (RR 0.53) Mortality (RR 0.79) Antibiotics used Oral quinolones Quinolones + beta-lactams Cephalosporins Carbapenems Chavez-Tapia (Cochrane), 2010
 Rebleeding (RR 0.53) Mortality (RR 0.79) Antibiotics used Oral quinolones Quinolones + beta-lactams Cephalosporins Carbapenems Chavez-Tapia (Cochrane), 2010")
41
ASA Sung AIM 2010 Should we stop ASA in patients with acute GI bleeding?

42
ASA 156 patients with acute GI hemorrhage ASA for cardiovascular or cerebrovascular disease EGD: stigmata of recent hemorrhage requiring endoscopic Rx Randomized to ASA 80 mg/day or placebo for 8 weeks Sung AIM 2010 Should we stop ASA in patients with acute GI bleeding?

43
ASA 156 patients with acute GI hemorrhage ASA for cardiovascular or cerebrovascular disease EGD: stigmata of recent hemorrhage requiring endoscopic Rx Randomized to ASA 80 mg/day or placebo for 8 weeks ASA Recurrent bleeding: 10% Mortality: 1% (cardiac 1) Placebo Recurrent bleeding: 5% Mortality: 13% (cardiac 5, GI 3, pneumonia 2) Sung AIM 2010 Should we stop ASA in patients with acute GI bleeding?
 Placebo Recurrent bleeding: 5% Mortality: 13% (cardiac 5, GI 3, pneumonia 2) Sung AIM 2010 Should we stop ASA in patients with acute GI bleeding")
44
ASA 156 patients with acute GI hemorrhage ASA for cardiovascular or cerebrovascular disease EGD: stigmata of recent hemorrhage requiring endoscopic Rx Randomized to ASA 80 mg/day or placebo for 8 weeks ASA Recurrent bleeding: 10% Mortality: 1% (cardiac 1) Placebo Recurrent bleeding: 5% Mortality: 13% (cardiac 5, GI 3, pneumonia 2) Sung AIM 2010 Should we stop ASA in patients with acute GI bleeding? Plavix?

45
Clopidogrel Interaction with PPIs Clopidogrel → active metabolite by CYP2C19 Omeprazole is also metabolized by CYP2C19 Omeprazole: ↓ levels of the active clopidogrel metabolite Clopidogrel does not cause peptic ulcer but increases bleeding risk, particularly in patients with a history of peptic ulcer Dikman APT 2009, Siller-Matula 2010, and others

46
Clopidogrel Interaction with PPIs Clopidogrel → active metabolite by CYP2C19 Omeprazole is also metabolized by CYP2C19 Omeprazole: ↓ levels of the active clopidogrel metabolite Dikman APT 2009, Siller-Matula 2010, and others

47
Clopidogrel Interaction with PPIs Clopidogrel → active metabolite by CYP2C19 Omeprazole is also metabolized by CYP2C19 Omeprazole: ↓ levels of the active clopidogrel metabolite Dikman APT 2009, Siller-Matula 2010, and others PPI together with clopidogrel: likely ↑ risk major cardiovascular events likely↓ risk GI bleed Effect may be greatest in slow metabolizers

48
Furuta BJCP 2010

49
Clopidogrel/PPI interaction Possible strategies Avoid PPI when not indicated Sequence CYP2C19 genotype Substitute H2 receptor antagonists Stagger clopidogrel and PPI doses Increase clopidogrel dose Add or substitute ASA Dikman APT 2009, Siller-Matula 2010, Furuta 2010, and others

53
Principles of endoscopic hemostasis Identify and target the point source of bleeding Only treat lesions that have a high likelihood of rebleeding Endoscopic Rx decreases rebleeding rate by > 50% Repeat endoscopic Rx is usually effective in those who rebleed

54
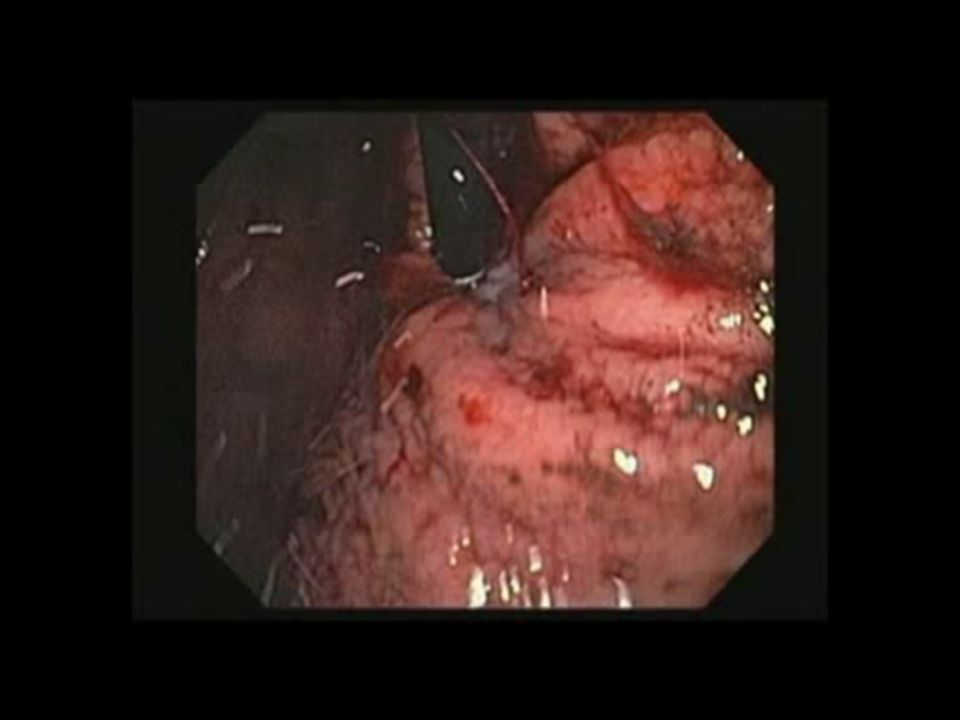
Dieulafoy’s Lesion

55
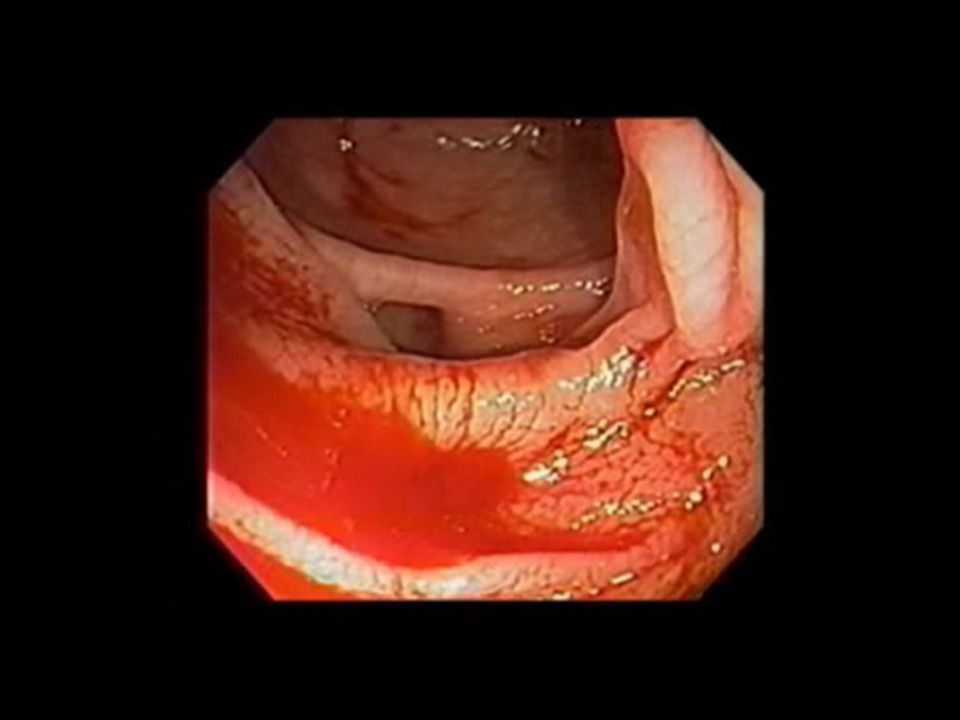
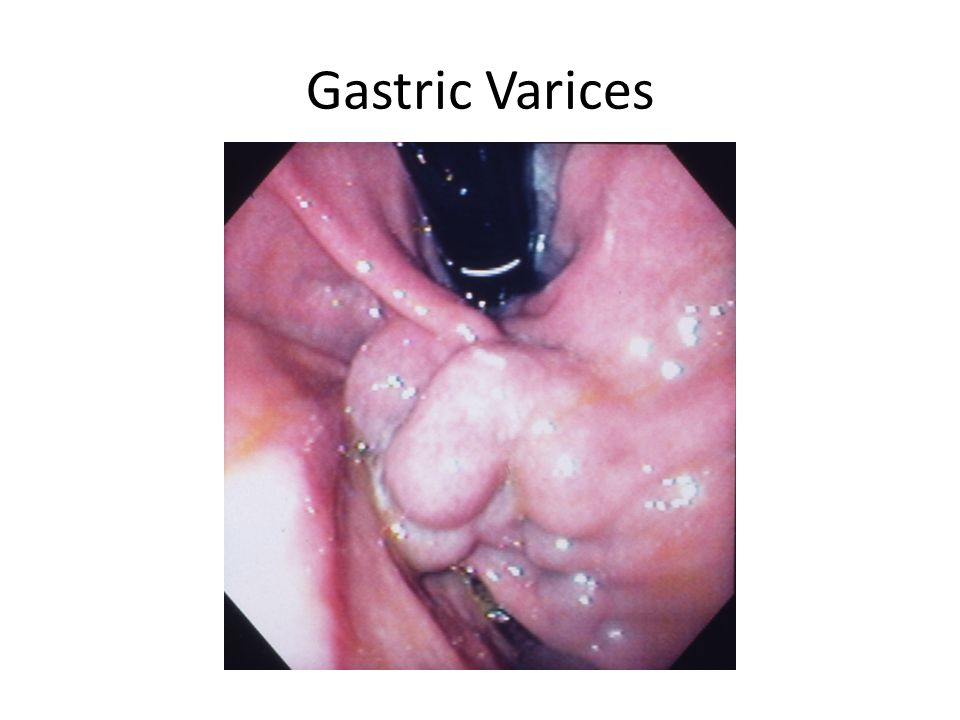
Gastric Varices

57
Minnesota Tube http://img.tfd.com/dorland/thumbs/tube_Sengstaken-Blakemore.jpg

58
http://er119.org/xoops_er119/uploads/photos/95.jpg

62
Early TIPS? TIPS prevents bleeding but is associated with liver failure TIPS is a rescue treatment Garcia-Pagan NEJM 2010

63
Early TIPS? TIPS prevents bleeding but is associated with liver failure TIPS is a rescue treatment 63 patients with variceal hemorrhage Childs-Pugh score of 7 – 13 (B or C) All received endoscopic and pharmacologic Rx Randomized to standard care or early TIPS Garcia-Pagan NEJM 2010
 All received endoscopic and pharmacologic Rx Randomized to standard care or early TIPS Garcia-Pagan NEJM")
64
Early TIPS? TIPS prevents bleeding but is associated with liver failure TIPS is a rescue treatment 63 patients with variceal hemorrhage Childs-Pugh score of 7 – 13 (B or C) All received endoscopic and pharmacologic Rx Randomized to standard care or early TIPS Standard Care Rebleeding (1 year) 45% Death (1 year) 39% Early TIPS Rebleeding (1 year) 3% Death (1 year) 13% Garcia-Pagan NEJM 2010
 All received endoscopic and pharmacologic Rx Randomized to standard care or early TIPS Standard Care Rebleeding (1 year) 45% Death (1 year) 39% Early TIPS Rebleeding (1 year) 3% Death (1 year) 13% Garcia-Pagan NEJM")
65
Stress Ulcer Prophylaxis Cook NEJM 1994, Cook CCM 1999, Lin 2010, and others Pathophysiology Ischemia (Curling’s ulcers) ↑Acid (Cushing’s ulcers)
 ↑Acid (Cushing’s ulcers)")
66
Stress Ulcer Prophylaxis Cook NEJM 1994, Cook CCM 1999, Lin 2010, and others Pathophysiology Ischemia (Curling’s ulcers) ↑Acid (Cushing’s ulcers) Risk factors Mechanical ventilation Coagulopathy Renal failure Burns, Trauma, Transplant
 ↑Acid (Cushing’s ulcers) Risk factors Mechanical ventilation Coagulopathy Renal failure Burns, Trauma, Transplant")
67
Stress Ulcer Prophylaxis Cook NEJM 1994, Cook CCM 1999, Lin 2010, and others Pathophysiology Ischemia (Curling’s ulcers) ↑Acid (Cushing’s ulcers) Risk factors Mechanical ventilation Coagulopathy Renal failure Burns, Trauma, Transplant Rx PPI ≥ H2RA
 ↑Acid (Cushing’s ulcers) Risk factors Mechanical ventilation Coagulopathy Renal failure Burns, Trauma, Transplant Rx PPI ≥ H2RA")
68
Prevention of late re-bleeding Peptic Ulcer Test for h pylori - C13 breath test, bx - confirm eradication Long term antisecretory Rx Gisbert (Cochrane) 2004, Ding WJG 2009, and others
 2004, Ding WJG 2009, and others")
69
Prevention of late re-bleeding Variceal hemorrhage Eradicate varices - Elective band ligation Beta blockers Gisbert (Cochrane) 2004, Ding WJG 2009, and others
 2004, Ding WJG 2009, and others")
Similar presentations














 682-3793; (p) 413-3222.>")


. Presents at 2am with a big haematemesis Unable to give a history.>")
 bleeding refers to any bleeding that starts in the gastrointestinal tract. Bleeding may come from.>")


