Download presentation
Presentation is loading. Please wait.

1
The Art and Science of Insulin
Thomas Repas D.O. Diabetes, Endocrinology and Nutrition Center, Affinity Medical Group, Neenah, Wisconsin Member, Inpatient Diabetes Management Committee, St. Elizabeth’s Hospital, Appleton, WI Member, Diabetes Advisory Group, Wisconsin Diabetes Prevention and Control Program Website:

2
Overview ! Goals and Purpose of Insulin Therapy
Barriers to the use of Insulin Current Concepts in Insulin Therapy Basal/Bolus Insulin Sliding Scales Insulin Pump Therapy Future of Insulin Conclusion !

3
Purpose of Insulin Therapy
Prevent and treat fasting and postprandial hyperglycemia Permit appropriate utilization of glucose and other nutrients by peripheral tissues Suppress hepatic glucose production Prevent acute complications of uncontrolled diabetes Prevent long term complications of chronic diabetes

4
The Goal of Insulin Therapy: Attempt to Mimic Normal Pancreatic Function
Schade, Skyler, Santiago, Rizza, “Intensive Insulin Therapy,” 1993, p. 131.

5
Barriers to the Use of Insulin
WHAT!? Did you say INSULIN?! Barriers to the Use of Insulin

6
Patient Concerns About Insulin
Fear of injections Perceived significance of need for insulin Worries that insulin could worsen diabetes Concerns about hypoglycemia Complexity of regimens

8
Help Patient Accept and Prepare for Insulin Therapy
Address patient concerns Dispel fear by countering misconceptions Review rationale for insulin use Explain that insulin Can be incorporated into lifestyle Causes only modest weight gain Is a common course of treatment for this progressive disease Promise patient support and close follow-up Monitoring can prevent hypoglycemia Today’s technology can facilitate daily injections and readings When initiating insulin therapy, it is important to offer reassurance about the risk-benefit ratio of using insulin for type 2 diabetes: Intensive treatment with insulin actually improves the insulin sensitivity of peripheral tissues, at least in the short term, by reducing the glucotoxic effects of hyperglycemia. Sustained intensive insulin treatment reduces the risk of several complications, including cardiovascular events.

9
Barriers to Insulin Therapy : Common Medical Concerns
Insulin therapy in type 2 diabetes might cause: Worsening Insulin Resistance? More Cardiovascular Risk? Weight Gain ? Hypoglycemia? Slide 6-8 Barriers to Insulin Therapy Common Concerns Insulin has been used therapeutically in patients with diabetes for more than 70 years and has an almost unlimited power to reduce plasma glucose. The major barriers to insulin use are a perceived increase of cardiovascular risk, weight gain, and the risk of hypoglycemia. Although a true cause/effect relationship has not been established between hyperinsulinemia and atherosclerosis, the development of weight gain during exogenous insulin therapy is a well-known phenomenon. The cycle of worsening insulin resistance, greater insulin requirements, and hyperinsulinemia is typical in diabetes. Central obesity, hypertension, and dyslipidemia are strongly associated with hyperinsulinemia and contribute substantially to the cardiac risk profile. Whether therapy with insulin actually increases (or decreases) cardiovascular risk is currently debated. The risk of mild to severe hypoglycemic reactions is increased with intensive insulin therapy and is dependent on numerous factors, including duration of diabetes, duration of insulin therapy, and degree of glycemic control, as well as prior hypoglycemic episodes. The following slides will present some of the published data bearing on these concerns. 6-8
 cardiovascular risk is currently debated. The risk of mild to severe hypoglycemic reactions is increased with intensive insulin therapy and is dependent on numerous factors, including duration of diabetes, duration of insulin therapy, and degree of glycemic control, as well as prior hypoglycemic episodes. The following slides will present some of the published data bearing on these concerns")
10
% of Matched Control Values
Insulin Sensitivity in Glucose Clamp Studies: Improved by Insulin Treatment Baseline After Insulin 100 87 80 80 67 57 60 53 % of Matched Control Values Glucose Disposal 40 40 Slide 6-9 BARRIERS TO INSULIN THERAPY Insulin Sensitivity in Glucose Clamp Studies Improved by Insulin Treatment Because insulin dosage correlates with insulin resistance in epidemiologic studies, and because insulin can cause weight gain that is also associated with insulin resistance, it has been feared that treatment with insulin may worsen insulin resistance. Three studies done with similar methods have directly tested this concern. Each study shown here examined the insulin sensitivity of peripheral tissues, mainly muscle, using the glucose-insulin clamp method, before and after restoration of good glycemic control in type 2 diabetes patients with aggressive insulin treatment. In each case the treatment period was short (2 to 4 weeks) and relatively high insulin dosage was required (>100 U daily). The figure shows the insulin sensitivity of tissues before and after treatment, expressed as a percentage of the mean value for insulin sensitivity of a nondiabetic control group that was matched in age, gender, and weight to the diabetic subjects. The three studies had remarkably similar results, with insulin sensitivity before treatment reduced by half, compared to the nondiabetic values, indicating marked insulin resistance. After treatment, insulin sensitivity improved toward the nondiabetic values, though some insulin resistance persisted, as would be expected. This improvement is presumably due to reduced “glucotoxicity” accompanying improved control of plasma glucose. Whether the improvement of insulin sensitivity persists when insulin treatment is continued was not tested in these studies. However, these studies show that, at least in the short term, successful insulin treatment reduces rather than worsens insulin resistance. Scarlett JA, Gray RS, Griffin J, Olefsky MJ, Kolterman OG. Insulin treatment reverses the insulin resistance of type II diabetes mellitus. Diabetes Care. 1982;5: ; Andrews WJ, Vasquez B, Nagulesparan M, et al. Insulin therapy in obese, non-insulin-dependent diabetes induces improvements in insulin action and secretion that are maintained for two weeks after insulin withdrawal. Diabetes. 1984;33: ; Garvey WT, Olefsky JM, Griffin J, Hamman RF, Kolterman OG. The effect of insulin treatment on insulin secretion and insulin action in type II diabetes mellitus. Diabetes. 1985;34: 20 Scarlett Andrews Garvey Scarlett, et al. Diabetes Care. 1982;5: ; Andrews, et al. Diabetes. 1984;33: ; Garvey, et al. Diabetes. 1985;34: 6-9
 and relatively high insulin dosage was required (>100 U daily). The figure shows the insulin sensitivity of tissues before and after treatment, expressed as a percentage of the mean value for insulin sensitivity of a nondiabetic control group that was matched in age, gender, and weight to the diabetic subjects. The three studies had remarkably similar results, with insulin sensitivity before treatment reduced by half, compared to the nondiabetic values, indicating marked insulin resistance. After treatment, insulin sensitivity improved toward the nondiabetic values, though some insulin resistance persisted, as would be expected. This improvement is presumably due to reduced glucotoxicity accompanying improved control of plasma glucose. Whether the improvement of insulin sensitivity persists when insulin treatment is continued was not tested in these studies. However, these studies show that, at least in the short term, successful insulin treatment reduces rather than worsens insulin resistance. Scarlett JA, Gray RS, Griffin J, Olefsky MJ, Kolterman OG. Insulin treatment reverses the insulin resistance of type II diabetes mellitus. Diabetes Care. 1982;5: ; Andrews WJ, Vasquez B, Nagulesparan M, et al. Insulin therapy in obese, non-insulin-dependent diabetes induces improvements in insulin action and secretion that are maintained for two weeks after insulin withdrawal. Diabetes. 1984;33: ; Garvey WT, Olefsky JM, Griffin J, Hamman RF, Kolterman OG. The effect of insulin treatment on insulin secretion and insulin action in type II diabetes mellitus. Diabetes. 1985;34: Scarlett. Andrews. Garvey. Scarlett, et al. Diabetes Care. 1982;5: ; Andrews, et al. Diabetes. 1984;33: ; Garvey, et al. Diabetes. 1985;34:")
11
Cardiovascular Risk Mortality After MI Reduced by Insulin Therapy in the DIGAMI Study
Standard treatment IV Insulin 48 hours, then 4 injections daily .7 All Subjects .7 Low-risk and Not Previously on Insulin (N = 620) (N = 272) .6 .6 Risk reduction (28%) Risk reduction (51%) .5 P = .011 .5 P = .0004 .4 .4 .3 .3 Slide 6-11 BARRIERS TO INSULIN THERAPY Cardiovascular Risk Mortality After MI Reduced by Insulin Therapy in the DIGAMI Study Patients at high risk of cardiovascular disease are often thought to be inappropriate candidates for treatment with insulin because of the belief that hypoglycemia, hyperinsulinemia, or other metabolic effects of insulin might provoke or worsen the outcome of major cardiovascular events. This figure shows data from the Diabetes Mellitus Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) trial. This Swedish trial studied the short-term and long-term effects of intensive insulin treatment of patients with diabetes who were enrolled in the trial at the time of a myocardial infarction. The subjects were immediately randomized to continued management according to the judgment of their physicians, or to intravenous infusion of insulin and glucose for 48 hours followed by a four-injection regimen subsequently for as long as 5 years. Other aspects of management of the infarction included treatment with b-blockers, angiotensin-converting enzyme inhibitors, fibrinolytic agents, and aspirin in high proportions of both groups. The rationale underlying the study was the old observation that, in animal experiments and studies of small numbers of humans, infarct size and outcome are improved by insulin- glucose infusion, in part because of suppression of otherwise elevated free fatty acid levels in plasma. The figure shows the cumulative total mortality rates in the whole population of 620 subjects randomized to the two treatments, as well as the rates for a predefined subgroup of subjects who were judged likely to survive the initial hospitalization and were not previously using insulin. The whole population showed an 11% actual and a 28% relative risk reduction with intensive insulin treatment after 5 years, and the subgroup showed a 15% actual and a 51% relative risk reduction. Most of the benefit was apparent in the first month of treatment and presumably was partly due to immediate intravenous infusion of insulin; however, the survival curves tended to separate further over time, suggesting an ongoing benefit from intensive treatment. This study suggests that insulin is an entirely appropriate treatment for patients with type 2 diabetes and high cardiovascular risk, especially at the time of myocardial infarction. Malmberg K, Rydén L, Hamsten A, Herlitz J, Waldenström, Wedel H, and the DIGAMI study group. Effects of insulin treatment on cause-specific one-year mortality and morbidity in diabetic patients with acute myocardial infarction. Eur Heart J. 1996;17: ; Nattrass M. Managing diabetes after myocardial infarction: time for a more aggressive approach. BMJ. 1997;314:1497; Malmberg K, and the DIGAMI study group. Prospective randomised study of intensive insulin treatment on long term survival after acute myocardial infarction in patients with diabetes mellitus. BMJ. 1997;314: .2 .2 .1 .1 1 2 3 4 5 1 2 3 4 5 Years of Follow-up Years of Follow-up Malmberg, et al. BMJ. 1997;314: 6-11
 (N = 272) Risk reduction (28%) Risk reduction (51%) .5. P = P = Slide BARRIERS TO INSULIN THERAPY. Cardiovascular Risk. Mortality After MI Reduced by Insulin Therapy in the DIGAMI Study. Patients at high risk of cardiovascular disease are often thought to be inappropriate candidates for treatment with insulin because of the belief that hypoglycemia, hyperinsulinemia, or other metabolic effects of insulin might provoke or worsen the outcome of major cardiovascular events. This figure shows data from the Diabetes Mellitus Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) trial. This Swedish trial studied the short-term and long-term effects of intensive insulin treatment of patients with diabetes who were enrolled in the trial at the time of a myocardial infarction. The subjects were immediately randomized to continued management according to the judgment of their physicians, or to intravenous infusion of insulin and glucose for 48 hours followed by a four-injection regimen subsequently for as long as 5 years. Other aspects of management of the infarction included treatment with b-blockers, angiotensin-converting enzyme inhibitors, fibrinolytic agents, and aspirin in high proportions of both groups. The rationale underlying the study was the old observation that, in animal experiments and studies of small numbers of humans, infarct size and outcome are improved by insulin- glucose infusion, in part because of suppression of otherwise elevated free fatty acid levels in plasma. The figure shows the cumulative total mortality rates in the whole population of 620 subjects randomized to the two treatments, as well as the rates for a predefined subgroup of subjects who were judged likely to survive the initial hospitalization and were not previously using insulin. The whole population showed an 11% actual and a 28% relative risk reduction with intensive insulin treatment after 5 years, and the subgroup showed a 15% actual and a 51% relative risk reduction. Most of the benefit was apparent in the first month of treatment and presumably was partly due to immediate intravenous infusion of insulin; however, the survival curves tended to separate further over time, suggesting an ongoing benefit from intensive treatment. This study suggests that insulin is an entirely appropriate treatment for patients with type 2 diabetes and high cardiovascular risk, especially at the time of myocardial infarction. Malmberg K, Rydén L, Hamsten A, Herlitz J, Waldenström, Wedel H, and the DIGAMI study group. Effects of insulin treatment on cause-specific one-year mortality and morbidity in diabetic patients with acute myocardial infarction. Eur Heart J. 1996;17: ; Nattrass M. Managing diabetes after myocardial infarction: time for a more aggressive approach. BMJ. 1997;314:1497; Malmberg K, and the DIGAMI study group. Prospective randomised study of intensive insulin treatment on long term survival after acute myocardial infarction in patients with diabetes mellitus. BMJ. 1997;314: Years of Follow-up. Years of Follow-up. Malmberg, et al. BMJ. 1997;314:")
12
Reassurance About Common Concerns
Insulin Therapy in Type 2 DM Improves Insulin Sensitivity by Reducing Glucotoxicity Reduces Cardiovascular Risk Causes Modest Weight Gain Rarely Causes Severe Hypoglycemia Patients fears and concerns can be addressed by education Slide 6-15 BARRIERS TO INSULIN THERAPY Reassurance About Common Concerns The preceding slides have presented findings that offer reassurance about the risk-benefit ratio of using insulin for type 2 diabetes. Slide 9 shows that intensive treatment with insulin actually improves the insulin sensitivity of peripheral tissues, at least in the short term, by reducing the glucotoxic effects of hyperglycemia. Slide 10 shows that insulin treatment improves triglyceride levels, fosters a trend toward better HDL levels, and has no effect on LDL levels or blood pressure. Slide 11 shows an impressively reduced mortality with immediate and sustained intensive insulin treatment following myocardial infarction, suggesting that in this setting the benefits outweigh any theoretical cardiovascular hazards. Slide 12 shows the weight gain found in the UKPDS with various treatments, confirming that insulin causes the most weight gain but also that the mean gain is relatively modest, about 10 lb during 10 years for both less obese and more obese patients. Slide 13 shows that concurrent use of metformin markedly reduces weight gain when insulin treatment is started or intensified. Slide 14 shows more data from the UKPDS confirming that both mild and severe hypoglycemia are more common with insulin treatment than with other treatments, but that the rate of severe hypoglycemia is quite low. Buse JB. Overview of current therapeutic options in type 2 diabetes. Diabetes Care ;22(suppl 3):C65-C70; Berger M, Jorgens V, Mühlhauser I. Rationale for the use of insulin therapy alone as the pharmacological treatment of type 2 diabetes. Diabetes Care. 1999;22(suppl 3):C71-C75; UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352: 6-15
:C65-C70; Berger M, Jorgens V, Mühlhauser I. Rationale for the use of insulin therapy alone as the pharmacological treatment of type 2 diabetes. Diabetes Care. 1999;22(suppl 3):C71-C75; UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:")
13
Current Concepts in Insulin Therapy

19
Comparison of Human Insulins and Analogues
Insulin Onset of Duration of Preparations Action Peak Action Lispro/Aspart 5-15 minutes 1-2 hours 3-5 hours Human Regular minutes 2-4 hours 4-8 hours Human NPH/Lente 1-4 hours 4-12 hours hours Human Ultralente 6-8 hours Unpredictable hours Glargine 2-3 hours Flat ~24 hours Slide 6-22 INSULIN TACTICS Comparison of Human Insulins and Analogues Insulin has been used therapeutically for more than 70 years. In general, human insulin, synthesized by genetically altered microorganisms, has a more rapid onset of action and a shorter duration of action than previous preparations derived from animal pancreas. Regular human insulin has an onset of action ranging from about 30 to 60 minutes with peak concentrations achieved at between 2 and 4 hours. The “intermediate-acting” insulins, NPH and lente, have gradual onset and peak effects usually between 4 and 8 hours, and a total duration of 10 to 20 hours. Human ultralente insulin is somewhat longer-acting, but still usually falls short of a 24-hour effect. Short- acting insulin analogues (lispro and aspart) have very desirable action profiles at mealtimes because they have an onset of action ranging from 5 to 15 minutes; the peak of action occurs 1 hour after injection, and the insulin effect practically vanishes 4 hours after administration. Insulin glargine is a long- acting analogue insulin that has essentially no peak. Glargine is absorbed within 1 to 2 hours and has a plasma concentration about 50% lower than that observed with NPH, but twice the duration of action. Bolli GB, Di Marchi RD, Park GD, Pramming S, Koivisto VA. Insulin analogues and their potential in the management of diabetes mellitus. Diabetologia. 1999;42: ; Kelley DB, ed. Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: American Diabetes Association; 1998:56-72; Edelman SV, Henry RR. Insulin therapy for normalizing glycosylated hemoglobin in type II diabetes: applications, benefits, and risks. Diabetes Reviews. 1995;3: ; Skyler JS. Insulin therapy in type 2 diabetes mellitus. In: DeFronzo RA, ed. Current Therapy of Diabetes Mellitus. St Louis, Mo: Mosby-Year Book Inc; 1998: ; Riddle MC. Evening insulin strategy. Diabetes Care. 1990;13: The time course of action of any insulin may vary in different individuals, or at different times in the same individual. Because of this variation, time periods indicated here should be considered general guidelines only. 6-22
 have very desirable action profiles at mealtimes because they have an onset of action ranging from 5 to 15 minutes; the peak of action occurs 1 hour after injection, and the insulin effect practically vanishes 4 hours after administration. Insulin glargine is a long- acting analogue insulin that has essentially no peak. Glargine is absorbed within 1 to 2 hours and has a plasma concentration about 50% lower than that observed with NPH, but twice the duration of action. Bolli GB, Di Marchi RD, Park GD, Pramming S, Koivisto VA. Insulin analogues and their potential in the management of diabetes mellitus. Diabetologia. 1999;42: ; Kelley DB, ed. Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: American Diabetes Association; 1998:56-72; Edelman SV, Henry RR. Insulin therapy for normalizing glycosylated hemoglobin in type II diabetes: applications, benefits, and risks. Diabetes Reviews. 1995;3: ; Skyler JS. Insulin therapy in type 2 diabetes mellitus. In: DeFronzo RA, ed. Current Therapy of Diabetes Mellitus. St Louis, Mo: Mosby-Year Book Inc; 1998: ; Riddle MC. Evening insulin strategy. Diabetes Care. 1990;13: The time course of action of any insulin may vary in different individuals, or at different times in the same individual. Because of this variation, time periods indicated here should be considered general guidelines only")
20
Twice-daily Split-mixed Regimens
Regular NPH Insulin Effect Slide 6-23 INSULIN TACTICS Twice-daily Split-mixed Regimens Twice-daily mixtures of NPH and regular insulins have been widely used for type 2 diabetes for many years. In some cases, premixed 70/30 insulin is used for this purpose. Patient profiles of insulin levels resulting from this method, as shown in this figure, do not come close to matching the normal endogenous secretory pattern, shown in the shaded background. Patients with type 1 diabetes using this “split- mixed” regimen rarely achieve reasonably good glycemic control by present standards, since they lack endogenous insulin to supplement the partially adequate profile of injected insulin. Type 2 diabetes patients who have substantial endogenous insulin may fare much better with this regimen, but may experience late morning or nocturnal hypoglycemia because of excessive levels of insulin at these times. Berger M, Jorgens V, Mühlhauser I. Rationale for the use of insulin therapy alone as the pharmacological treatment of type 2 diabetes. Diabetes Care. 1999;22(suppl 3):C71-C75; Edelman SV, Henry RR. Insulin therapy for normalizing glycosylated hemoglobin in type II diabetes: applications, benefits, and risks. Diabetes Reviews ;3: B L S HS B 6-23
:C71-C75; Edelman SV, Henry RR. Insulin therapy for normalizing glycosylated hemoglobin in type II diabetes: applications, benefits, and risks. Diabetes Reviews. 1995;3: B. L. S. HS. B")
21
Multiple Daily Injections (MDI) NPH + Regular
NPH at AM and HS + Regular AC NPH at HS + Regular AC Regular Regular NPH NPH Insulin Effect Insulin Effect Slide 6-24 INSULIN TACTICS Multiple Daily Injections (MDI) NPH + Regular Another strategy, shown in this slide, consists of two injections of NPH (or lente) insulin daily plus two or three injections of regular insulin with meals. The second injection of NPH is given at bedtime, to confer less risk of nocturnal hypoglycemia while providing enough insulin to control overnight fasting glucose levels. This is often called a multiple daily injection (MDI) regimen. It is widely used for type 1 diabetes patients but is also appropriate for type 2 diabetes patients whose endogenous levels are declining. The match of insulin levels to endogenous needs is better with this approach than with twice-daily NPH and regular, but still not very good. B L S HS B B L S HS B 6-24
 NPH + Regular. Another strategy, shown in this slide, consists of two injections of NPH (or lente) insulin daily plus two or three injections of regular insulin with meals. The second injection of NPH is given at bedtime, to confer less risk of nocturnal hypoglycemia while providing enough insulin to control overnight fasting glucose levels. This is often called a multiple daily injection (MDI) regimen. It is widely used for type 1 diabetes patients but is also appropriate for type 2 diabetes patients whose endogenous levels are declining. The match of insulin levels to endogenous needs is better with this approach than with twice-daily NPH and regular, but still not very good. B. L. S. HS. B. B. L. S. HS. B")
22
Multiple Daily Injections (MDI) Ultralente + Regular
Insulin Effect Slide 6-25 INSULIN TACTICS Multiple Daily Injections (MDI) Ultralente + Regular This slide shows another version of an MDI regimen, with ultralente given once daily (usually at bedtime or suppertime) or sometimes twice daily, together with three mealtime injections of regular insulin. Its results are generally similar to those of MDI using NPH and regular. B L S HS B 6-25
 Ultralente + Regular. This slide shows another version of an MDI regimen, with ultralente given once daily (usually at bedtime or suppertime) or sometimes twice daily, together with three mealtime injections of regular insulin. Its results are generally similar to those of MDI using NPH and regular. B. L. S. HS. B")
23
Limitations of Human Regular Insulin
Slow onset of action Requires inconvenient administration: 20 to 40 minutes prior to meal Risk of hypoglycemia if meal is further delayed Mismatch with postprandial hyperglycemic peak Long duration of activity Up to 12 hours’ duration Increased at higher dosages Potential for late postprandial hypoglycemia Slide 6-26 INSULIN TACTICS Limitations of Human Regular Insulin The preceding slides illustrate some of the limitations of human regular insulin. If it is given immediately prior to a meal, its onset of action is too slow to match the normal insulin peak and the blood glucose response to the meal is much greater than in a person without diabetes. To improve the relationship between the profile of action of regular insulin and the needs accompanying the meal, patients are routinely advised to administer their injection 20 to 40 minutes prior to the meal. This is inconvenient, is infrequently achieved, and poses the risk of premeal hypoglycemia if the meal is inadvertently delayed. Furthermore, the duration of action of regular insulin is much longer than the normal insulin peak following meals, typically at least 6 hours and up to 12 hours when large doses are injected. This persistence of high insulin levels leads to risk of hypoglycemia, which is often countered by between-meal snacks that foster weight gain in type 2 diabetes patients. 6-26

24
Basal and Bolus Insulins
Slide 6-16 Mimicking Nature The Basal/Bolus Insulin Concept This approach to insulin therapy combines basal insulin to meet the insulin requirement to suppress hepatic glucose production between meals with bolus insulin (prandial or mealtime) and to meet the insulin requirement to maintain normal glucose levels after eating. The next several slides will illuminate this concept. 6-16
 and to meet the insulin requirement to maintain normal glucose levels after eating. The next several slides will illuminate this concept")
25
The Basal/Bolus Insulin Concept
Basal Insulin Suppresses glucose production between meals and overnight Nearly constant levels 50% of daily needs Bolus Insulin (Mealtime or Prandial) Limits hyperglycemia after meals Immediate rise and sharp peak at 1 hour 10% to 20% of total daily insulin requirement at each meal Slide 6-20 MIMICKING NATURE WITH INSULIN THERAPY The Basal/Bolus Insulin Concept Insulin is capable of restoring glycemia to nearly normal in most patients with type 2 diabetes. The basal/bolus insulin concept attempts to mimic, with insulin therapy, the patterns that normally control glucose in persons without diabetes. Basal insulin suppresses glucose production so that the levels remain nearly constant between meals and overnight. Basal insulin meets about half of the patient’s daily need for insulin and may be sufficient when considerable endogenous insulin remains. Bolus insulin (10% to 20% of the total daily insulin requirement given at each meal) limits hyperglycemia after meals. This tends to smooth the peaks of glucose that occur in response to these meals. Frequent glucose monitoring aids in determining the candidates for basal or mealtime regimens. Ideally, each component of insulin replacement therapy should come from a different type of insulin with a specific profile to fit the patient’s needs. Practical methods to accomplish this basal/bolus strategy will be illustrated later in this module. Edelman SV, Henry RR. Insulin therapy for normalizing glycosylated hemoglobin in type II diabetes: applications, benefits, and risks. Diabetes Reviews. 1995;3: ; Kelley DB, ed. Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: American Diabetes Association; 1998:56-72. Ideally, for insulin replacement therapy, each component should come from a different insulin with a specific profile 6-20
 Limits hyperglycemia after meals. Immediate rise and sharp peak at 1 hour. 10% to 20% of total daily insulin requirement at each meal. Slide MIMICKING NATURE WITH INSULIN THERAPY. The Basal/Bolus Insulin Concept. Insulin is capable of restoring glycemia to nearly normal in most patients with type 2 diabetes. The basal/bolus insulin concept attempts to mimic, with insulin therapy, the patterns that normally control glucose in persons without diabetes. Basal insulin suppresses glucose production so that the levels remain nearly constant between meals and overnight. Basal insulin meets about half of the patient’s daily need for insulin and may be sufficient when considerable endogenous insulin remains. Bolus insulin (10% to 20% of the total daily insulin requirement given at each meal) limits hyperglycemia after meals. This tends to smooth the peaks of glucose that occur in response to these meals. Frequent glucose monitoring aids in determining the candidates for basal or mealtime regimens. Ideally, each component of insulin replacement therapy should come from a different type of insulin with a specific profile to fit the patient’s needs. Practical methods to accomplish this basal/bolus strategy will be illustrated later in this module. Edelman SV, Henry RR. Insulin therapy for normalizing glycosylated hemoglobin in type II diabetes: applications, benefits, and risks. Diabetes Reviews. 1995;3: ; Kelley DB, ed. Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: American Diabetes Association; 1998: Ideally, for insulin replacement therapy, each component should come from a different insulin with a specific profile")
26
Insulin and Glucose Patterns: Normal and Type 2 Diabetes
400 120 100 300 80 mg/dL 200 U/mL 60 40 100 Slide 6-17 MIMICKING NATURE WITH INSULIN THERAPY Insulin and Glucose Patterns Normal and Type 2 Diabetes This figure compares the normal 24-hour profiles of glucose and insulin concentrations in plasma with those typical of type 2 diabetes. Polonsky et al studied 16 patients with untreated type 2 diabetes and 14 matched controls. Plasma glucose levels were considerably higher in the diabetic patients both under fasting conditions and in response to meals, as expected. The main abnormality was a prominent increase of fasting and 24-hour mean glucose levels. The rise of glucose after meals was proportionately less abnormal than the fasting elevations. The basal and 24-hour mean levels of insulin and C-peptide, however, did not differ greatly from those in the control group. Still, compared to normal subjects, diabetic patients did show significantly lower incremental responses of insulin secretion to meals, and the increases of insulin secretion after meals were more sluggish. These patterns suggest that, in type 2 diabetes, much higher fasting glucose is required to stimulate the b-cells to secrete enough insulin to suppress overnight glucose production by the liver and kidney. The authors of this paper studied other aspects of insulin secretion in these patients and found several kinds of abnormalities. Polonsky KS, Bruce D, Given MD, et al. Abnormal patterns of insulin secretion in non- insulin-dependent diabetes mellitus. N Engl J Med. 1988;318: 20 0600 1000 1400 1800 2200 0200 0600 0600 1000 1400 1800 2200 0200 0600 B L S B L S Time of Day Time of Day Polonsky, et al. N Engl J Med. 1988;318: 6-17

27
Rapid-acting Analogues: Clinical Features
Insulin profile more closely mimics normal physiology Convenient administration immediately prior to meals Faster onset of action Limit postprandial hyperglycemic peaks Shorter duration of activity Reduced late postprandial hypoglycemia But more frequent late postprandial hyperglycemia Need for basal insulin replacement revealed Slide 6-27 INSULIN TACTICS Short-acting Analogues: Lispro and Aspart Clinical Features Two quick-acting insulin analogues, insulin lispro and insulin aspart, have absorption profiles that more closely match normal mealtime patterns. Small alterations in their molecular structure relative to human insulin reduce their tendency to aggregate into pairs (dimers) or groups of six (hexamers) molecules, thus speeding their absorption after subcutaneous injection. Because of this property, they can be given immediately before meals. This timing is much more convenient for patients than waiting 20 to 40 minutes after the injections to begin eating. Their quick onset of action matches normal mealtime peaks of plasma insulin better than does human regular insulin. Clinical studies have shown that these properties lead to less prominent peaks of glucose after meals and less late postprandial hypoglycemia. However, rapid waning of the effects of mealtime lispro and aspart leads to greater dependency on adequate basal insulin levels between meals and overnight. 6-27
 or groups of six (hexamers) molecules, thus speeding their absorption after subcutaneous injection. Because of this property, they can be given immediately before meals. This timing is much more convenient for patients than waiting 20 to 40 minutes after the injections to begin eating. Their quick onset of action matches normal mealtime peaks of plasma insulin better than does human regular insulin. Clinical studies have shown that these properties lead to less prominent peaks of glucose after meals and less late postprandial hypoglycemia. However, rapid waning of the effects of mealtime lispro and aspart leads to greater dependency on adequate basal insulin levels between meals and overnight")
28
Rapid-acting Insulin Analogues: Lispro and Aspart
400 500 Aspart Lispro 450 350 400 300 350 250 300 200 250 Plasma Insulin (pmol/L) Regular Plasma Insulin (pmol/L) 200 150 Human 150 100 Regular 100 Human 50 Slide 6-28 INSULIN TACTICS Short-acting Insulin Analogues: Lispro and Aspart Plasma Insulin Profiles This figure shows two separate experiments displaying the plasma insulin profiles after injection of insulin lispro and insulin aspart in comparison to that of human regular insulin. The experiment with lispro, shown on the left, included 10 patients with type 1 diabetes, and the experiment with aspart shows findings from 18 healthy subjects. Both of these analogues have very rapid onset of action, which allows them to be taken immediately before meals. Both reach a peak about 1 hour after injection, with a decline in baseline levels in 4 hours, closely matching normal insulin patterns. The delayed and extended profile of human regular insulin is seen in both studies, with significant elevations above baseline persisting well beyond 4 hours after injection. Heinemann L, Heise T, Wahl LC, et al. Prandial glycaemia after a carbohydrate-rich meal in type I diabetic patients: using the rapid acting insulin analogue [Lys(B28), Pro (B29)] human insulin. Diabet Med. 1996;13: ; Mudaliar SR, Strange P, Lindberg FA, et al. Insulin aspart (B28 asp-insulin): a fast-acting analog of human insulin. Diabetes Care ;22: 50 30 60 90 120 150 180 210 240 50 100 150 200 250 300 Time (min) Time (min) Meal SC injection Meal SC injection Heinemann, et al. Diabet Med. 1996;13: ; Mudaliar, et al. Diabetes Care. 1999;22: 6-28
 Regular. Plasma Insulin (pmol/L) Human Regular Human. 50. Slide INSULIN TACTICS. Short-acting Insulin Analogues: Lispro and Aspart. Plasma Insulin Profiles. This figure shows two separate experiments displaying the plasma insulin profiles after injection of insulin lispro and insulin aspart in comparison to that of human regular insulin. The experiment with lispro, shown on the left, included 10 patients with type 1 diabetes, and the experiment with aspart shows findings from 18 healthy subjects. Both of these analogues have very rapid onset of action, which allows them to be taken immediately before meals. Both reach a peak about 1 hour after injection, with a decline in baseline levels in 4 hours, closely matching normal insulin patterns. The delayed and extended profile of human regular insulin is seen in both studies, with significant elevations above baseline persisting well beyond 4 hours after injection. Heinemann L, Heise T, Wahl LC, et al. Prandial glycaemia after a carbohydrate-rich meal in type I diabetic patients: using the rapid acting insulin analogue [Lys(B28), Pro (B29)] human insulin. Diabet Med. 1996;13: ; Mudaliar SR, Strange P, Lindberg FA, et al. Insulin aspart (B28 asp-insulin): a fast-acting analog of human insulin. Diabetes Care. 1999;22: Time (min) Time (min) Meal. SC injection. Meal. SC injection. Heinemann, et al. Diabet Med. 1996;13: ; Mudaliar, et al. Diabetes Care. 1999;22:")
30
Multiple Daily Injections (MDI) NPH + Mealtime Lispro
NPH at AM and HS + Lispro AC NPH at HS + Lispro AC Insulin Effect B S L HS Lispro NPH Slide 6-29 INSULIN TACTICS Multiple Daily Injections (MDI) NPH + Mealtime Lispro This schematic slide shows the profiles resulting from two kinds of multiple-injection regimens in which insulin lispro is substituted for human regular insulin. The peaks of lispro more closely match the normal profile, but the 4-hour duration of lispro leaves lunch and late evening poorly covered by insulin with the two-mealtime-injection regimen on the left. With NPH at bedtime and lispro with meals, as shown on the right, clear gaps of coverage of basal requirements are evident as well. 6-29
 NPH + Mealtime Lispro. This schematic slide shows the profiles resulting from two kinds of multiple-injection regimens in which insulin lispro is substituted for human regular insulin. The peaks of lispro more closely match the normal profile, but the 4-hour duration of lispro leaves lunch and late evening poorly covered by insulin with the two-mealtime-injection regimen on the left. With NPH at bedtime and lispro with meals, as shown on the right, clear gaps of coverage of basal requirements are evident as well")
31
Limitations of Human NPH, Lente, and Ultralente
Do not mimic basal insulin profile Variable absorption Pronounced peaks Less than 24-hour duration of action Cause unpredictable hypoglycemia Major factor limiting insulin adjustments More weight gain Slide 6-30 THE ROLE OF INSULIN IN TYPE 2 DIABETES Limitations of Human NPH, Lente, and Ultralente Clinical use of insulin lispro, a better mealtime insulin than human regular, has directed attention to the properties of extended-release human insulins that have been used to provide basal insulin replacement. Human NPH, lente, and ultralente insulin all have mean durations of action of less than 24 hours, precluding them from providing adequate basal insulin replacement for many patients. All three, but especially NPH and lente, have pronounced peaks of action. Ultralente is thought to have substantial day-to-day variation of action. These limitations cause variations of glucose levels and unpredictable hypoglycemia, which are the leading factors limiting glycemic control at the present time. Recurrent hypoglycemia with insulin therapy of type 2 diabetes may be one factor in weight gain. 6-30

32
The Quest for Basal Insulin Replacement
Mealtime Lispro + NPH and NPH at HS Lispro NPH Insulin Effect Slide 6-31 INSULIN TACTICS Multiple Daily Injections (MDI) The Quest for Basal Insulin Replacement An experimental intensive insulin regimen tested by Italian researchers in patients with type 1 diabetes illustrates the lack of adequate long- acting insulin preparations to provide a reliable and consistent basal insulin. The quest for basal insulin replacement has prompted the use of multiple daily injections of mealtime insulin lispro + NPH and NPH at bedtime. The combination of four doses of NPH with higher proportions of lispro provides a constant basal insulin, with the desired insulin peak effects after mealtimes, as well as maintenance of better glycemic control during the night and between meals. Bolli GB, Di Marchi RD, Park GD, Pramming S, Koivisto VA. Insulin analogues and their potential in the management of diabetes mellitus. Diabetologia. 1999;42: B L S HS B Bolli, et al. Diabetologia. 1999; 42: 6-31
 The Quest for Basal Insulin Replacement. An experimental intensive insulin regimen tested by Italian researchers in patients with type 1 diabetes illustrates the lack of adequate long- acting insulin preparations to provide a reliable and consistent basal insulin. The quest for basal insulin replacement has prompted the use of multiple daily injections of mealtime insulin lispro + NPH and NPH at bedtime. The combination of four doses of NPH with higher proportions of lispro provides a constant basal insulin, with the desired insulin peak effects after mealtimes, as well as maintenance of better glycemic control during the night and between meals. Bolli GB, Di Marchi RD, Park GD, Pramming S, Koivisto VA. Insulin analogues and their potential in the management of diabetes mellitus. Diabetologia. 1999;42: B. L. S. HS. B. Bolli, et al. Diabetologia. 1999; 42:")
33
The Ideal Basal Insulin . . .
Mimics normal pancreatic basal insulin secretion Long-lasting effect around 24 hours Smooth, peakless profile Reproducible and predictable effects Reduced risk of nocturnal hypoglycemia Once-daily administration for convenience Slide 6-32 INSULIN TACTICS The Ideal Basal Insulin… A growing need exists for an insulin preparation that can provide a basal insulin profile. The lack of reproducibility in glucose-lowering effects of previously available preparations, including NPH insulin and ultralente, continues to be a major limitation for most insulin regimens. The ideal basal insulin replacement would mimic normal pancreatic basal insulin secretion, provide 24-hour effects, sustain a smooth, peakless insulin profile, and employ a regimen that has reproducible, predictable effects once steady state is achieved. Ideal basal insulin would reduce the risk of nocturnal hypoglycemia with the convenience of once-daily administration. 6-32

34
Profiles of Various Basal Insulins
Glargine NPH Ultralente CSII n = 20 T1DM Mean ± SEM SC insulin 4.0 3.0 2.0 1.0 24 20 16 12 8 4 Time (h) mg/kg/min mol/kg/min The goal of diabetes treatment is maintenance of long-term near-normoglycemia to prevent the onset and/or progression of long-term complications. Different insulins have different mechanisms of action, with differing abilities to meet this treatment goal. Glargine is a peakless insulin with a long duration of action (nearly 24 hours). Because of these features, it is associated with less nocturnal hypoglycemia and lower postprandial glucose levels. Glargine also has a lower intersubject variability than NPH and ultralente, and it closely mimics continuous subcutaneous insulin infusion (CSII), the gold standard of basal insulin replacement. Lepore M, Pampanelli S, Fanelli C, et al. Pharmacokinetics and pharmacodynamics of subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente human insulin and continuous subcutaneous infusion of insulin lispro. Diabetes. 2000;49: SC=subcutaneous; CSII=continuous subcutaneous insulin infusion Lepore M et al. Diabetes. 2000;49:
 mg/kg/min. mol/kg/min. The goal of diabetes treatment is maintenance of long-term near-normoglycemia to prevent the onset and/or progression of long-term complications. Different insulins have different mechanisms of action, with differing abilities to meet this treatment goal. Glargine is a peakless insulin with a long duration of action (nearly 24 hours). Because of these features, it is associated with less nocturnal hypoglycemia and lower postprandial glucose levels. Glargine also has a lower intersubject variability than NPH and ultralente, and it closely mimics continuous subcutaneous insulin infusion (CSII), the gold standard of basal insulin replacement. Lepore M, Pampanelli S, Fanelli C, et al. Pharmacokinetics and pharmacodynamics of subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente human insulin and continuous subcutaneous infusion of insulin lispro. Diabetes. 2000;49: SC=subcutaneous; CSII=continuous subcutaneous insulin infusion. Lepore M et al. Diabetes. 2000;49:")
35
Long-Acting Insulins: Ultralente and Glargine
Injected once or twice daily Onset within 6–8 hours Peak effect within 10–20 hours Glargine 24-hour, long-acting recombinant human insulin analogue has no peak Cannot be diluted or mixed with other insulins or solutions Administered once daily In combination therapy, glargine given at bedtime; rapid- or short-acting given during the day Review slide and include comments based on experience.

36
Glucose Utilization Rate
Glargine vs NPH Insulin in Type 1 Diabetes Action Profiles by Glucose Clamp 6 5 4 NPH Glucose Utilization Rate (mg/kg/h) 3 2 Glargine Slide 6-34 INSULIN TACTICS Glargine vs NPH Insulin in Type 1 Diabetes Action Profiles by Glucose Clamp Lepore et al conducted pharmacokinetic studies of insulin glargine in 20 type 1 diabetes patients. Patients were studied in a two-way crossover clamp design after subcutaneous injection. Onset of action was more delayed with insulin glargine (median 1.1 vs 0.7 hours, respectively) and more prolonged (median 22.8 vs 13.8 hours, respectively) compared with NPH. Glucose utilization rates shown on this slide indicate that insulin glargine has a peakless, long-acting profile that closely mimics that of nondiabetic subjects. Lepore M, Kurzhals R, Pampanelli S, Fanelli CG, Bolli GB. Pharmacokinetics and dynamics of s.c. injection of the long-acting insulin glargine (HOE1) in T1DM. Diabetes. 1999;48 (suppl 1):A97. 1 10 20 30 Time (h) After SC Injection End of observation period Lepore, et al. Diabetes. 1999;48(suppl 1):A97. 6-34
 Glargine. Slide INSULIN TACTICS. Glargine vs NPH Insulin in Type 1 Diabetes. Action Profiles by Glucose Clamp. Lepore et al conducted pharmacokinetic studies of insulin glargine in 20 type 1 diabetes patients. Patients were studied in a two-way crossover clamp design after subcutaneous injection. Onset of action was more delayed with insulin glargine (median 1.1 vs 0.7 hours, respectively) and more prolonged (median 22.8 vs 13.8 hours, respectively) compared with NPH. Glucose utilization rates shown on this slide indicate that insulin glargine has a peakless, long-acting profile that closely mimics that of nondiabetic subjects. Lepore M, Kurzhals R, Pampanelli S, Fanelli CG, Bolli GB. Pharmacokinetics and dynamics of s.c. injection of the long-acting insulin glargine (HOE1) in T1DM. Diabetes. 1999;48 (suppl 1):A Time (h) After SC Injection. End of observation period. Lepore, et al. Diabetes. 1999;48(suppl 1):A")
37
Bedtime Glargine vs NPH, With Mealtime Regular
4 48 NPH Glargine 3 ** 36 2 Patients (%) 24 1 Baseline Baseline 12 8.5 1 8.8 1 11.1 4 10.6 4 1 * * Slide 6-51 INSULIN TACTICS Advancing With Multiple Daily Injections Bedtime Glargine vs NPH, With Mealtime Regular A multicenter, randomized, parallel group study was conducted to compare insulin glargine with NPH in patients with type 2 diabetes who were previously treated with insulin-only therapy. The 518 patients were randomized to receive insulin glargine once daily at bedtime or NPH once daily at bedtime or twice daily in the morning and at bedtime based on the patient’s prestudy insulin regimen. In addition, the patients were allowed to use preprandial regular insulin as part of their daily regimen. At baseline, the mean HbA1c was 8.5% and mean FPG was 11.1 mmol/L (196 mg/dL). Similar reductions were observed in HbA1c (–0.41% in the insulin glargine group compared with –0.59% in the NPH group). Compared with baselines, patients receiving insulin glargine achieved a significant reduction in FPG of 1.72 mmol/L (–31 mg/dL) and the NPH groups achieved a reduction of 1.17 mmol/L (–21 mg/dL). Of note, the risk of nocturnal hypoglycemia was reduced by 25% in the patients receiving insulin glargine (31.3% vs 40.2%; P < .02). Rosenstock J, Schwartz S, Clark C, Edwards M, Donley D. Efficacy and safety of HOE 901 (insulin glargine) in subjects with type 2 DM: a 28-week randomized, NPH insulin- controlled trial. Diabetes. 1999;48(suppl 1):A100. * 2 * HbA1c FPG Nocturnal (%) (mmol/L) Hypoglycemia *P < .01 (change from baseline to endpoint within each group) **P < .02 (compared to NPH) Rosenstock, et al. Diabetes. 1999;48(suppl 1):A100. 6-51
 Baseline. Baseline 1. * * Slide INSULIN TACTICS. Advancing With Multiple Daily Injections. Bedtime Glargine vs NPH, With Mealtime Regular. A multicenter, randomized, parallel group study was conducted to compare insulin glargine with NPH in patients with type 2 diabetes who were previously treated with insulin-only therapy. The 518 patients were randomized to receive insulin glargine once daily at bedtime or NPH once daily at bedtime or twice daily in the morning and at bedtime based on the patient’s prestudy insulin regimen. In addition, the patients were allowed to use preprandial regular insulin as part of their daily regimen. At baseline, the mean HbA1c was 8.5% and mean FPG was 11.1 mmol/L (196 mg/dL). Similar reductions were observed in HbA1c (–0.41% in the insulin glargine group compared with –0.59% in the NPH group). Compared with baselines, patients receiving insulin glargine achieved a significant reduction in FPG of 1.72 mmol/L (–31 mg/dL) and the NPH groups achieved a reduction of 1.17 mmol/L (–21 mg/dL). Of note, the risk of nocturnal hypoglycemia was reduced by 25% in the patients receiving insulin glargine (31.3% vs 40.2%; P < .02). Rosenstock J, Schwartz S, Clark C, Edwards M, Donley D. Efficacy and safety of HOE 901 (insulin glargine) in subjects with type 2 DM: a 28-week randomized, NPH insulin- controlled trial. Diabetes. 1999;48(suppl 1):A100. * 2. * HbA1c. FPG. Nocturnal. (%) (mmol/L) Hypoglycemia. *P < .01 (change from baseline to endpoint within each group) **P < .02 (compared to NPH) Rosenstock, et al. Diabetes. 1999;48(suppl 1):A")
38
Bedtime Glargine vs NPH, With Mealtime Regular
4 48 NPH Glargine 3 36 ** 2 24 Weight (kg) Patients (%) 1 12 Slide 6-52 INSULIN TACTICS Advancing With Multiple Daily Injections Bedtime Glargine vs NPH, With Mealtime Regular Rosenstock et al examined the effects of advancing multiple daily insulin injection regimens to include bedtime insulin glargine. In this study of patients, significant reductions in HbA1c in the insulin glargine patients were associated with less weight gain compared with those receiving NPH. At 28 weeks, patients in the insulin glargine group had gained 0.41 kg (0.9 lb) compared with 1.4 kg (3.1 lb) in the patients receiving NPH. Presumably, this effect (ie, less weight gain in the insulin glargine group) is a clinical reflection of less frequent episodes of hypoglycemia and decreased supplemental caloric intake in patients receiving bedtime insulin glargine. In general, very few patients experienced severe hypoglycemia and the insulin glargine patients experienced a 25% reduction in the frequency of episodes of nocturnal hypoglycemia compared with those receiving NPH. Rosenstock J, Schwartz S, Clark C, Edwards M, Donley D. Efficacy and safety of HOE 901 (insulin glargine) in subjects with type 2 DM: a 28-week randomized, NPH insulin- controlled trial. Diabetes. 1999;48(suppl 1):A100. * Weight Gain Nocturnal Hypoglycemia *P < **P < .02 (compared to NPH) Rosenstock, et al. Diabetes. 1999;48(suppl 1):A100. 6-52
 Patients (%) Slide INSULIN TACTICS. Advancing With Multiple Daily Injections. Bedtime Glargine vs NPH, With Mealtime Regular. Rosenstock et al examined the effects of advancing multiple daily insulin injection regimens to include bedtime insulin glargine. In this study of 518 patients, significant reductions in HbA1c in the insulin glargine patients were associated with less weight gain compared with those receiving NPH. At 28 weeks, patients in the insulin glargine group had gained 0.41 kg (0.9 lb) compared with 1.4 kg (3.1 lb) in the patients receiving NPH. Presumably, this effect (ie, less weight gain in the insulin glargine group) is a clinical reflection of less frequent episodes of hypoglycemia and decreased supplemental caloric intake in patients receiving bedtime insulin glargine. In general, very few patients experienced severe hypoglycemia and the insulin glargine patients experienced a 25% reduction in the frequency of episodes of nocturnal hypoglycemia compared with those receiving NPH. Rosenstock J, Schwartz S, Clark C, Edwards M, Donley D. Efficacy and safety of HOE 901 (insulin glargine) in subjects with type 2 DM: a 28-week randomized, NPH insulin- controlled trial. Diabetes. 1999;48(suppl 1):A100. * Weight Gain. Nocturnal. Hypoglycemia. *P < **P < .02 (compared to NPH) Rosenstock, et al. Diabetes. 1999;48(suppl 1):A")
39
Insulin Glargine Summary of Completed Trials
Glucose-insulin clamp studies of Glargine vs NPH Smooth, continuous release from injection site Longer duration of action with effect for about 24 hours Peakless profile Equivalent absorption rates at various injection sites Clinical efficacy equivalent to NPH, with significantly less nocturnal hypoglycemia Slide 6-35 INSULIN TACTICS Insulin Glargine Summary of Completed Trials Glucose-insulin clamp studies have compared the actions of insulin glargine with those of NPH. In general, these trials have found that insulin glargine provides a smooth, continuous release of insulin from the injection site. With an essentially flat profile, compared with other insulins, insulin glargine has a longer duration of action, providing constant levels for about 24 hours. Studies have demonstrated no variation in absorption rates at various injection sites (arm, leg, abdomen). Finally, the duration of action of insulin glargine allows for once-daily dosing. Improvements in glycemic control indicate that insulin glargine is clinically equivalent to NPH, with significantly fewer incidents of nocturnal hypoglycemia. 6-35
. Finally, the duration of action of insulin glargine allows for once-daily dosing. Improvements in glycemic control indicate that insulin glargine is clinically equivalent to NPH, with significantly fewer incidents of nocturnal hypoglycemia")
40
Type 1 diabetics should be on a basal / bolus insulin regimen
All Type 1 diabetics should be on a basal / bolus insulin regimen to control glucose while minimizing hypoglycemia Slide 6-19 MIMICKING NATURE WITH INSULIN THERAPY Over time, most patients will need both basal and mealtime insulin to control glucose Since both fasting and postprandial glucose levels are abnormal in type 2 diabetes and the underlying insulin deficiency typically progresses, most patients will need both basal insulin and mealtime insulin if excellent glucose control is to be maintained. The goal of intensive insulin therapy is to delay the onset of microvascular complications and retard their progression once they occur. 6-19

41
most type 2 diabetics will also need both basal and mealtime insulin
However over time, most type 2 diabetics will also need both basal and mealtime insulin to control glucose Slide 6-19 MIMICKING NATURE WITH INSULIN THERAPY Over time, most patients will need both basal and mealtime insulin to control glucose Since both fasting and postprandial glucose levels are abnormal in type 2 diabetes and the underlying insulin deficiency typically progresses, most patients will need both basal insulin and mealtime insulin if excellent glucose control is to be maintained. The goal of intensive insulin therapy is to delay the onset of microvascular complications and retard their progression once they occur. 6-19

42
Beginning Insulin Therapy
Slide 6-36 Overcoming Complexity by Starting With Basal Insulin One way to overcome the complexity of multiple daily insulin injection regimens is to start with basal insulin in patients with type 2 diabetes who are no longer responding adequately to oral agents. 6-36

43
When Oral Medications Are Not Enough
Watch for the following signs Increasing BG levels Elevated A1C Unexplained weight loss Traces of ketonuria Poor energy level Sleep disturbances Polydipsia Next steps Make a decision to start insulin Offer patient encouragement, not blame An A1C level of 7% or higher is a signal to reappraise a patient’s treatment plan. For a patient on combination oral therapy, the primary care physician must consider the initiation of insulin. Remind the patient of disease progression…

44
Natural History of Type 2 Diabetes
Severity of Glucose Intolerance NGT IGT Frank Diabetes Insulin Secretion Risk of Macrovascular Complications Insulin Resistance Worsens with Time Postprandial Glucose Fasting Blood Glucose Explain each component (line) as it is animated. Type 2 diabetes begins with insulin resistance (impaired glucose tolerance), which is linked to macrovascular disease. Beta cell function accelerates to compensate, however, it eventually begins to deteriorate, resulting in insulin deficiency and elevated glucose. In response to deteriorating beta cell function and subsequent loss of first-phase insulin response, postprandial glucose increases, which is associated with the initiation of macrovascular complications. While fasting glucose levels remain normal during the initial stages of this cycle. They eventually rise, initiating the development of microvascular complications. Main Message(s) While physicians often look at fasting glucose as an indication of control, we can see that the postprandial glucose is the initial driver of hyperglycemia and microvascular complications. Because beta cell deterioration is progressive and persistent, all patients who live long enough will eventually need insulin therapy. With the increasing prevalence of type 2 diabetes among younger adults, we will see many patients living with diabetes for many years. Normal Blood Glucose Risk of Microvascular Complications Years to Decades Typical Diagnosis of Diabetes
 as it is animated. Type 2 diabetes begins with insulin resistance (impaired glucose tolerance), which is linked to macrovascular disease. Beta cell function accelerates to compensate, however, it eventually begins to deteriorate, resulting in insulin deficiency and elevated glucose. In response to deteriorating beta cell function and subsequent loss of first-phase insulin response, postprandial glucose increases, which is associated with the initiation of macrovascular complications. While fasting glucose levels remain normal during the initial stages of this cycle. They eventually rise, initiating the development of microvascular complications. Main Message(s) While physicians often look at fasting glucose as an indication of control, we can see that the postprandial glucose is the initial driver of hyperglycemia and microvascular complications. Because beta cell deterioration is progressive and persistent, all patients who live long enough will eventually need insulin therapy. With the increasing prevalence of type 2 diabetes among younger adults, we will see many patients living with diabetes for many years. Normal Blood Glucose. Risk of Microvascular Complications. Years to Decades. Typical Diagnosis of Diabetes.")
45
Initiating Insulin Therapy in Type 2 Diabetes
Let blood glucose levels guide choice of insulins Select type(s) of insulin and timing of injection(s) based on pattern of patient’s sugar (fasting, lunch, dinner, bedtime) Choose from currently available insulin preparations Rapid-acting (mealtime): lispro, aspart Short-acting (mealtime): regular insulin Intermediate-acting (background): NPH, lente Long-acting (background): ultralente, glargine Insulin mixtures Provide long-acting or intermediate-acting as basal and rapid-acting as bolus Titrate every week As described, patients often proceed from taking a single oral medication to taking 2 or more oral agents or a combination of oral medication with insulin. Commonly, insulin is initiated in a schedule with intermediate- or long-acting insulin at bedtime to control fasting glucose levels and oral medications to control daytime glucose levels. Goal: to approximate endogenous insulin secretion…
 of insulin and timing of injection(s) based on pattern of patient’s sugar (fasting, lunch, dinner, bedtime) Choose from currently available insulin preparations. Rapid-acting (mealtime): lispro, aspart. Short-acting (mealtime): regular insulin. Intermediate-acting (background): NPH, lente. Long-acting (background): ultralente, glargine. Insulin mixtures. Provide long-acting or intermediate-acting as basal. and rapid-acting as bolus. Titrate every week. As described, patients often proceed from taking a single oral medication to taking 2 or more oral agents or a combination of oral medication with insulin. Commonly, insulin is initiated in a schedule with intermediate- or long-acting insulin at bedtime to control fasting glucose levels and oral medications to control daytime glucose levels. Goal: to approximate endogenous insulin secretion…")
46
Starting With Basal Insulin: Advantages
1 injection with no mixing Slow, safe, and simple titration Low dosage Limited weight gain Effective improvement in glycemic control Slide 6-37 INSULIN TACTICS Starting With Basal Insulin Advantages Patients who no longer respond adequately to oral agents will benefit from combination therapy that consists of maintaining the use of oral antidiabetic agents together with insulin therapy. The advantages of adding basal insulin to prior treatment with oral agents include the following: (1) only one insulin injection may be required each day, with no need for mixing different types of insulin; (2) the use of insulin pens can enhance patient acceptance of the treatment; (3) titration can be accomplished in a slow, safe, simple fashion; and (4) eventually combination therapy requires a lower total dose of insulin. The result is effective improvement in glycemic control while causing only limited weight gain. 6-37
 only one insulin injection may be required each day, with no need for mixing different types of insulin; (2) the use of insulin pens can enhance patient acceptance of the treatment; (3) titration can be accomplished in a slow, safe, simple fashion; and (4) eventually combination therapy requires a lower total dose of insulin. The result is effective improvement in glycemic control while causing only limited weight gain")
47
Glargine at HS + Oral Agents or Mealtime Lispro
TZD lispro Metformin Glargine Glargine Insulin Effect Insulin Effect Slide 6-56 INSULIN TACTICS: THE FUTURE Glargine at HS + Oral Agents or Inhaled Insulin Based on the advances in insulin therapy, it may be proposed that future regimens for type 2 diabetes patients might include the use of an injectable long-acting basal insulin analogue in combination with oral agents or with inhaled human insulin. The addition of basal insulin glargine to a combination of oral agents can improve glycemic control, reducing glucotoxicity, which may in turn restore endogenous insulin response to sulfonylurea and potentiate the effect of insulin sensitizers. Alternatively, the long-acting insulin glargine can provide a basal insulin profile to be associated in the future with prandial inhaled insulin, which mimics normal insulin effects in response to meals. B L S HS B B L S HS B 6-56

48
Starting with Basal Insulin
Continue oral agent(s) at same dosage (eventually stop secretegogue) Add single, evening insulin dose (around 10 U) Glargine (bedtime or anytime?) NPH (bedtime) 70/30 (evening meal) or 75/25 Adjust dose by fasting BG Increase insulin dose weekly as needed Increase 4 U if FBG >140 mg/dL Increase 2 U if FBG = 120 to 140 mg/dL Treat to target (usually <120 mg/dL) Slide 6-59 PRACTICAL GUIDELINES Starting Basal Insulin The most critical approach to the management of type 2 diabetes patients with persistent hyperglycemia despite combination oral therapy is to use a simple, straightforward strategy that will facilitate initiation of insulin therapy. The increasing use of insulin pens will certainly simplify the administration of insulin, and its use can be demonstrated to patients in “real time” during their visit to the physician’s office. It is very important that patients continue the oral agents at the same dosage and eventually reduce this dose when appropriate. Conservatively, a single insulin dose of around 10 U of NPH given at bedtime or 70/30 insulin given at the evening meal is a standard initial approach to treatment. Basal insulin glargine has the potential to facilitate and extend the use of this insulin strategy because of its long duration of action, peakless flat profile, more predictable response, and reduced risk of hypoglycemia. Insulin glargine is given once daily at bedtime, but based on its insulin kinetics, it could theoretically be given at any time. The insulin dose should be adjusted according to the fasting SMBG level. The insulin dose can be increased on a weekly basis as needed. It should be increased by 4 U if the fasting blood glucose (FBG) is greater than 140 mg/dL, and by 2 U if the FBG is 120 to 140 mg/dL. The treat- to-target level is usually an FBG < 120 mg/dL. 6-59
 at same dosage (eventually stop secretegogue) Add single, evening insulin dose (around 10 U) Glargine (bedtime or anytime ) NPH (bedtime) 70/30 (evening meal) or 75/25. Adjust dose by fasting BG. Increase insulin dose weekly as needed. Increase 4 U if FBG >140 mg/dL. Increase 2 U if FBG = 120 to 140 mg/dL. Treat to target (usually <120 mg/dL) Slide PRACTICAL GUIDELINES. Starting Basal Insulin. The most critical approach to the management of type 2 diabetes patients with persistent hyperglycemia despite combination oral therapy is to use a simple, straightforward strategy that will facilitate initiation of insulin therapy. The increasing use of insulin pens will certainly simplify the administration of insulin, and its use can be demonstrated to patients in real time during their visit to the physician’s office. It is very important that patients continue the oral agents at the same dosage and eventually reduce this dose when appropriate. Conservatively, a single insulin dose of around 10 U of NPH given at bedtime or 70/30 insulin given at the evening meal is a standard initial approach to treatment. Basal insulin glargine has the potential to facilitate and extend the use of this insulin strategy because of its long duration of action, peakless flat profile, more predictable response, and reduced risk of hypoglycemia. Insulin glargine is given once daily at bedtime, but based on its insulin kinetics, it could theoretically be given at any time. The insulin dose should be adjusted according to the fasting SMBG level. The insulin dose can be increased on a weekly basis as needed. It should be increased by 4 U if the fasting blood glucose (FBG) is greater than 140 mg/dL, and by 2 U if the FBG is 120 to 140 mg/dL. The treat- to-target level is usually an FBG < 120 mg/dL")
49
Advancing Bolus/ Adding Bolus Insulin
Indicated when FBG acceptable but HbA1c not at goal and/or Postprandial BG not at goal (<140mg/dl) Insulin options To Glargine, add mealtime Regular or Lispro To bedtime NPH, add morning NPH and mealtime Regular or Lispro To suppertime 70/30 or 75/25, add morning 70/30 or 75/25 Oral agent considerations Usually stop secretagogue (it is redundant to be on insulin and secretagogue) Continue metformin and TZD for additional glycemic and other benefits Slide 6-60 PRACTICAL GUIDELINES Advancing Basal/Bolus Insulin Clinical judgment should prevail when determining whether an advance to a basal/bolus insulin regimen is indicated, especially when the fasting blood glucose is acceptable, but this should be considered when the HbA1c is >7% or >7.5% suggesting postprandial hyperglycemia, and/or the SMBG before dinner is >180 mg/dL. There are three main insulin options. The first option is to add morning NPH and mealtime regular or lispro to the initial regimen of bedtime NPH insulin. The second option is to add morning 70/30 to suppertime 70/30 insulin. The third option is to add mealtime regular or lispro to bedtime insulin glargine. In terms of options for the oral agent, the sulfonylurea may be stopped, but some patients may develop wide fluctuations in blood glucose levels that require resumption of the sulfonylurea. For some patients, metformin can be continued to provide weight control, or glitazone can be continued to achieve glycemic stability. 6-60
 Insulin options. To Glargine, add mealtime Regular or Lispro. To bedtime NPH, add morning NPH and mealtime Regular or Lispro. To suppertime 70/30 or 75/25, add morning 70/30 or 75/25. Oral agent considerations. Usually stop secretagogue (it is redundant to be on insulin and secretagogue) Continue metformin and TZD for additional glycemic and other benefits. Slide PRACTICAL GUIDELINES. Advancing Basal/Bolus Insulin. Clinical judgment should prevail when determining whether an advance to a basal/bolus insulin regimen is indicated, especially when the fasting blood glucose is acceptable, but this should be considered when the HbA1c is >7% or >7.5% suggesting postprandial hyperglycemia, and/or the SMBG before dinner is >180 mg/dL. There are three main insulin options. The first option is to add morning NPH and mealtime regular or lispro to the initial regimen of bedtime NPH insulin. The second option is to add morning 70/30 to suppertime 70/30 insulin. The third option is to add mealtime regular or lispro to bedtime insulin glargine. In terms of options for the oral agent, the sulfonylurea may be stopped, but some patients may develop wide fluctuations in blood glucose levels that require resumption of the sulfonylurea. For some patients, metformin can be continued to provide weight control, or glitazone can be continued to achieve glycemic stability")
50
Changing from Other regimens to Basal/Bolus Insulin
Total Daily Dose (~70-75% of prior insulin regimen TDD) ~50% Basal* ~50% Bolus* Usually divided into 3 premeal doses *Range: 40 to 60%
 ~50% Basal* ~50% Bolus* Usually divided into 3 premeal doses. *Range: 40 to 60%")
51
An Example: Mr. M: 58 yo with history type 2 diabetes for 8 years
In addition to oral meds, he is on 70/30 insulin: 30 u AM and 15 u PM Current Total Daily Dose = 45 u of 70/30 However, he has been having difficulty with wide glycemic excursions After discussing his options in detail, he is willing to begin basal/bolus regimen: New TDD= 45 u x .75 = = 34 u Basal = 17 u Lantus at bedtime Bolus = 17 u total / 3 = 5.6 u = 5 u Humalog with meals

52
Another method Same patient: Mr. M on 70/30 insulin: 30 u AM and 15 u PM Current Total Daily Dose = 45 u of 70/30 Instead, some clinicians prefer to instead calculate the new basal/bolus doses independently of each other Current Basal= 0.70 x 45 u TDD = 31.5 u N Current Bolus= 0.30 x 45 u TDD = 13.5 u R Then, use 70 to 75% of prior NPH, but divide prior short acting into 3 premeal doses New Basal= 0.75 x 31.5 u N = 24 u Lantus New Bolus= 13.5 u R / 3 = 4.5 u (round up or down) premeal Humalog
 premeal Humalog.")
53
Remember: every patient is an individual!
So which method is best? This is where the “Art of Medicine” comes in: If patient has been having difficulty with hypoglycemia, then start any new insulin regimen with conservative doses If patient, on the other hand, has been having hyperglycemia, then one can be more aggressive Remember: every patient is an individual!

54
Fine Tuning of Bolus Doses

55
Bolus Dose Insulin Premeal boluses:
Taken before meals Covers mealtime carbohydrate intake Prevents postprandial hyperglycemia Correction or supplementation boluses: Used to Correct and treat hyperglycemia May be given alone between meals for hyperglycemia May be given to supplement already scheduled insulin to cover premeal hyperglycemia

56
Calculation of Premeal Bolus Doses
Methods Estimate patient’s individual insulin-to carb ratio Formula: 500 Rule Weight based Method Only use patient’s pre-pump insulin: CHO ratio IF HAS BEEN SUCCESSFUL!! * Bode et al: Diabetes Care 1994: 19:

57
Determination of Insulin to Carb Ratio: Method 1
EXAMPLE: Estimate 1 unit of insulin: 15 gm carb Note: 1 unit: 15 gm is often a “safe” starting point for most patients . . .

58
Determination of Insulin to Carb Ratio: Method 2
Use the 500 Rule: Divide 500 by TDD= 1 unit insulin to ___ gm CHO as bolus EXAMPLE: 500 ÷ 34 u= 15 Bolus ratio is 1 u insulin : 15 gm CHO

59
Determination of Insulin to Carb Ratio: Method 3
Weight (lb) Insulin u: CHO gm * 1: 16 1: 15 1: 14 1: 13 1: 12 1: 11 1: 10 1: 9 200+ 1: 8 Weight Based Method *Walsh, Pumping Insulin, 2nd ed.
 Insulin u: CHO gm * : : : : : : : : : 8. Weight Based Method. *Walsh, Pumping Insulin, 2nd ed.")
60
Premeal Insulin and Carb Counting

61
Macronutrient Conversion to Blood Glucose
CHO is converted most rapidly –fiber takes longer Protein takes up to 6-8 hours, fat takes 12 hours or longer, but can cause delays in CHO absorption

62
Carbohydrate Counting
Benefits Allows for variation in appetite and preferences Increases variety of food choices Can be used to match insulin bolus doses to food intake

63
Carb Counting and Insulin Bolusing
Insulin-to-Carb Ratio EXAMPLE: 1 unit insulin: 15 grams CHO Sample Meal 1 c. orange juice g 2 slices toast g ½ c. oatmeal g 1 soft-cooked egg 1 tsp margarine Coffee & 1 T cream _____________________ Total CHO: g Insulin bolus: units Sample Meal 2 slices wheat bread g 2 oz. turkey breast Lettuce leaf, tomato slice 1 tsp mayonnaise ring pretzels g 2 small choc cookies g Diet soda, 16 oz__________ Total CHO: g Insulin bolus: units 1 unit insulin to every 15 gm CHO is a good starting amount. Patients need individualization: may require 1:10, 1:20, etc. Once the basal rates are set, can work on the bolus ratio!

64
Fine Tuning: Meal Bolus Doses
Adjust bolus based on post-meal BGs Carbohydrate counting or pre-determined meal portion Individualize insulin to carbohydrate dose or insulin to premeal dose

65
Correction Boluses for Hyperglycemia

66
Correction Bolus Insulin
To be taken to correct for hyperglycemia Based on insulin sensitivity factor Goal is for correction bolus to lower blood glucose to within 30 to 50 mg/dl of target value

67
Insulin Sensitivity Factor
Use to high blood glucose 1 unit of insulin will blood glucose by: mg/dl Regular: Rule Humalog: Rule 1500 or 1800 divided by TDD= amount of blood glucose lowered by 1 unit insulin

68
Insulin Sensitivity Factor
EXAMPLE TDD is 34 units 1500 Rule: ÷ 34 = 44 1 unit of Regular bg 44 mg/dl 1800 Rule: ÷ 34 = 53 1 unit of Humalog bg 53 mg/dl

69
Combining Correction and Premeal Boluses
If a patient’s insulin to carb ratio is 1:15gm and the insulin correction factor is 1: 50 mg/dl and their premeal BG goal is < 110 mg/dl….. What dose of Humalog would you give premeal if their actual premeal BG = 210 mg/dl and they are about to eat a turkey sandwich (30 gms carbs)? 210 mg/dl –110 mg/dl = 100/50 = 2 u for correction 30 gms carbs/15 = 2 u for mealtime carb coverage Premeal total insulin bolus dose = 4 u
 210 mg/dl –110 mg/dl = 100/50 = 2 u for correction. 30 gms carbs/15 = 2 u for mealtime carb coverage. Premeal total insulin bolus dose = 4 u.")
70
A Quick Word on using Sliding Scale Insulin….
Don’t!

71
Instead of Sliding Scale....
Think Supplementation or Correction Scale… Basal insulin is necessary even in the fasting state Sliding scales do not provide physiologic insulin needs Sliding scales often result in “chasing” of blood sugars There can be wide glycemic excursions Remember: Just because a diabetic’s FBG is <150 does not mean that they need no insulin!

73
The Solution: In acutely ill hospitalized diabetics: use continuous IV insulin If one must use an insulin scale in an outpatient or stable inpatient setting: Insulin scale should only supplement a routine scheduled regimen of basal and premeal insulin May use to correct for hyperglycemia between scheduled doses of insulin It should NEVER be ordered such that the scale is the only source of insulin for the patient

74
The Future of Insulin Therapy Slide 6-53 Future Insulin Therapy
The future looks bright for new insulin strategies using improved insulin preparations. Good examples are the fast-acting insulin analogues and the new long-acting insulin analogue that was developed through recombinant DNA technology, which may provide more physiologic basal-insulin supplementation. In addition, the possibility of using new routes of administration, such as inhaled insulin, is an exciting approach that is currently undergoing extensive clinical research. 6-53

75
The Future of Insulin Inhaled Insulin: Exubra, others
Oral / Buccal Insulin: Oralin New basal insulin: Insulin Detemir New Rapid Acting Insulin Analogue Other: Closed Loop Systems (Artificial pancreas) Slide 6-54 Insulin Tactics: The Future This slide shows some of the treatment approaches involving combination therapy with new insulin preparations that may prove viable in the future. They include the use of combination oral agents + basal insulin glargine, combination oral agents + bolus inhaled insulin, and basal insulin glargine + bolus inhaled insulin. The combination oral agents may consist of a sulfonylurea plus an insulin sensitizer, such as a glitazone or metformin, which also helps control weight gain. Basal insulin glargine has the advantage of providing prolonged action that may last up to 24 hours, with the relatively constant supply of basal insulin resulting from the continuous release of insulin from the injection site. Compared to injections, bolus inhaled insulin may provide mealtime insulin in a less invasive route of administration, which most patients would probably prefer. 6-54
 Slide Insulin Tactics: The Future. This slide shows some of the treatment approaches involving combination therapy with new insulin preparations that may prove viable in the future. They include the use of combination oral agents + basal insulin glargine, combination oral agents + bolus inhaled insulin, and basal insulin glargine + bolus inhaled insulin. The combination oral agents may consist of a sulfonylurea plus an insulin sensitizer, such as a glitazone or metformin, which also helps control weight gain. Basal insulin glargine has the advantage of providing prolonged action that may last up to 24 hours, with the relatively constant supply of basal insulin resulting from the continuous release of insulin from the injection site. Compared to injections, bolus inhaled insulin may provide mealtime insulin in a less invasive route of administration, which most patients would probably prefer")
78
Oral Agents + Mealtime Inhaled Insulin: Effect on HbA1c
Oral Agents Alone Inhaled Insulin 10 9 2.3% 8 * HbA1c (%) 7 Slide 6-55 INSULIN TACTICS: THE FUTURE Oral Agents + Mealtime Inhaled Insulin Effect on HbA1c The concept of inhaled insulin has been explored for those patients with type 2 diabetes who resist initiating insulin therapy because it requires injections. As a response to this resistance, a dry powder aerosol delivery system of human insulin has been developed. Weiss et al examined the ability of mealtime inhaled insulin to improve glycemic control in 69 subjects. Patients were randomized to a 3-month treatment period of either continued oral agents alone (sulfonylurea and/or metformin) or in combination with 1 or 2 puffs of inhaled insulin before meals. The inhaled insulin doses were titrated based on glucose testing 4 times daily. Patients continuing on oral agents alone showed little change in HbA1c at 12 weeks (–0.13%), while those receiving the inhaled insulin in addition to the oral agents exhibited a marked improvement in HbA1c (–2.28%). Weiss SR, Berger S, Cheng S, Kourides I, Landschulz W, Gelfand RA, for the Phase II Inhaled Insulin Study Group. Diabetes. 1999;48(suppl 1):A12. 6 5 Baseline Follow-up Baseline Follow-up (0) (12) (0) (12) Weeks *P < .001 Weiss, et al. Diabetes. 1999;48(suppl 1):A12. 6-55
 7. Slide INSULIN TACTICS: THE FUTURE. Oral Agents + Mealtime Inhaled Insulin. Effect on HbA1c. The concept of inhaled insulin has been explored for those patients with type 2 diabetes who resist initiating insulin therapy because it requires injections. As a response to this resistance, a dry powder aerosol delivery system of human insulin has been developed. Weiss et al examined the ability of mealtime inhaled insulin to improve glycemic control in 69 subjects. Patients were randomized to a 3-month treatment period of either continued oral agents alone (sulfonylurea and/or metformin) or in combination with 1 or 2 puffs of inhaled insulin before meals. The inhaled insulin doses were titrated based on glucose testing 4 times daily. Patients continuing on oral agents alone showed little change in HbA1c at 12 weeks (–0.13%), while those receiving the inhaled insulin in addition to the oral agents exhibited a marked improvement in HbA1c (–2.28%). Weiss SR, Berger S, Cheng S, Kourides I, Landschulz W, Gelfand RA, for the Phase II Inhaled Insulin Study Group. Diabetes. 1999;48(suppl 1):A Baseline. Follow-up. Baseline. Follow-up. (0) (12) (0) (12) Weeks. *P < Weiss, et al. Diabetes. 1999;48(suppl 1):A")
79
Summary: Insulin Therapy
Replaces complete lack of insulin in type 1 diabetes Supplements progressive deficiency in type 2 diabetes Basal insulin added to oral agents can be used to start Full replacement requires basal-bolus regimen Hypoglycemia and weight gain are main medical risks New insulin analogues and injection devices facilitate use

Similar presentations
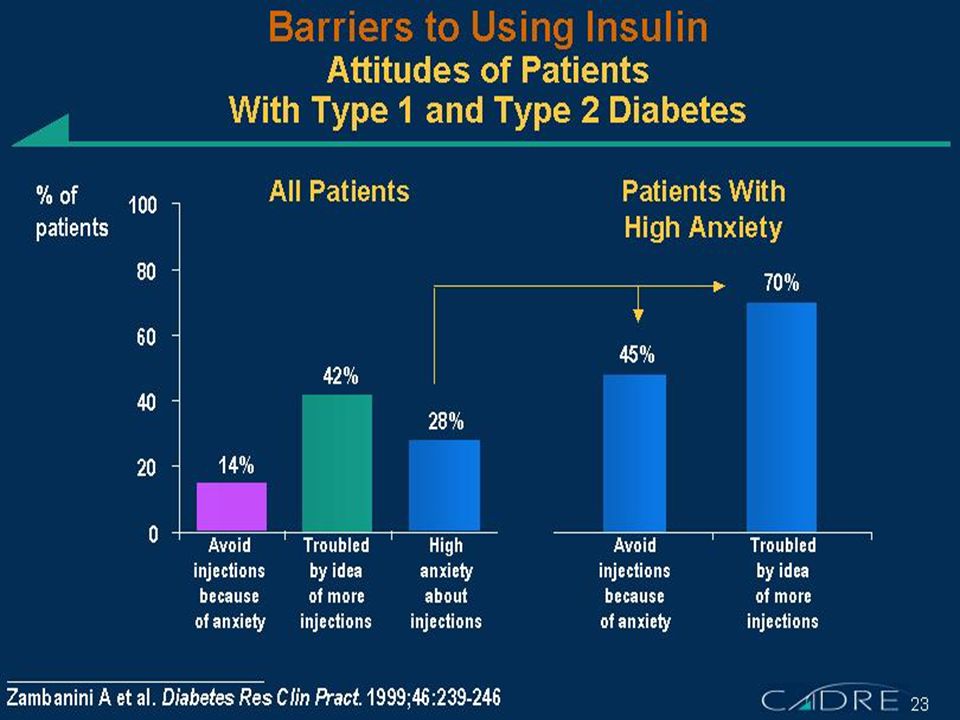

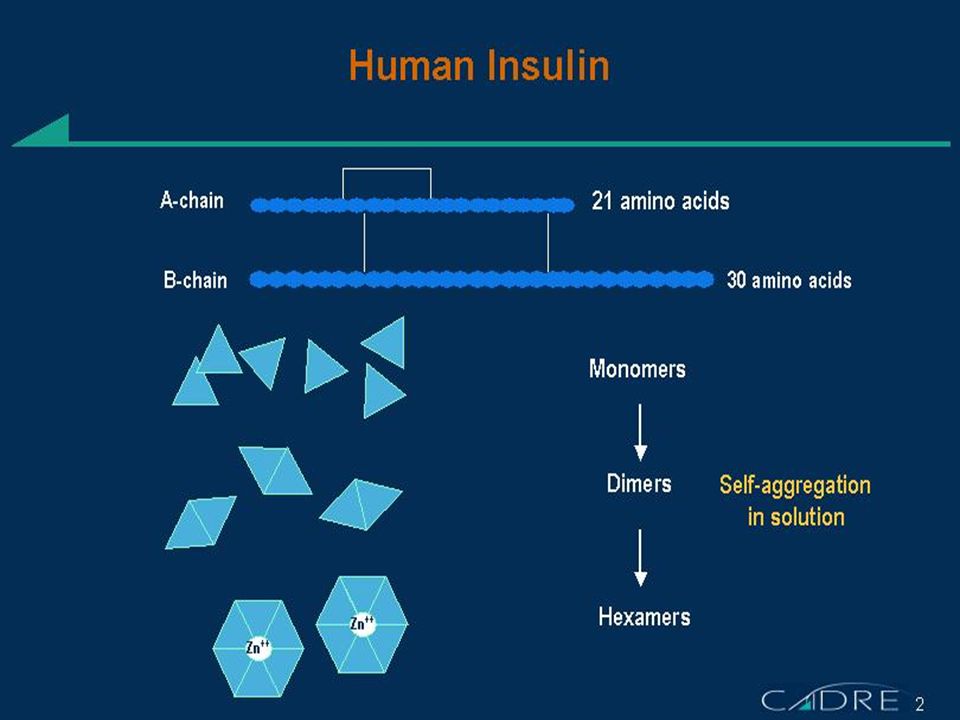
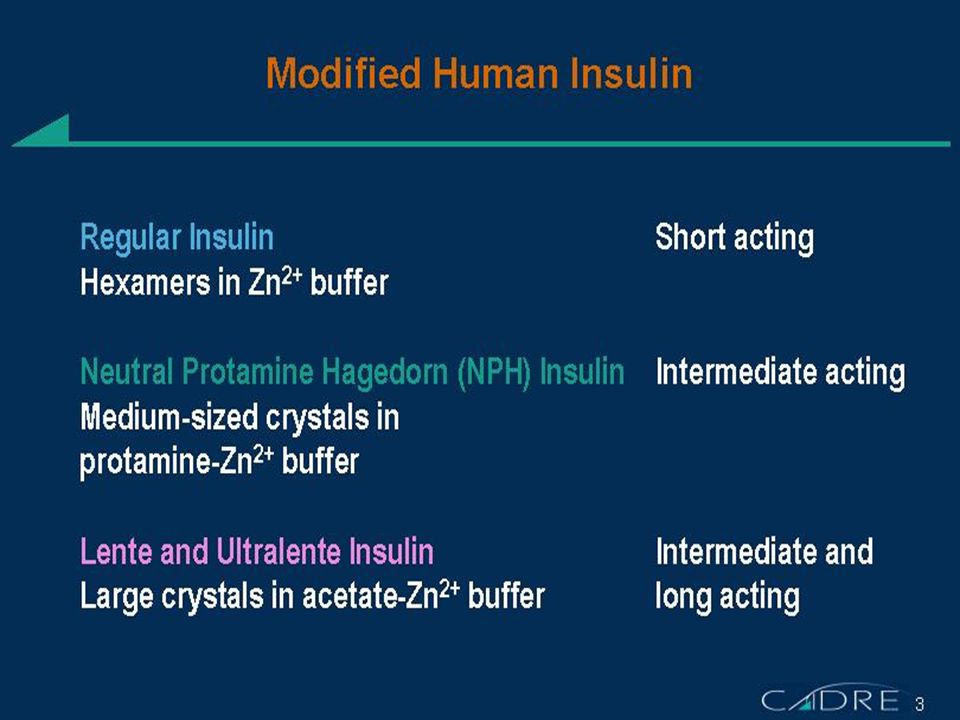
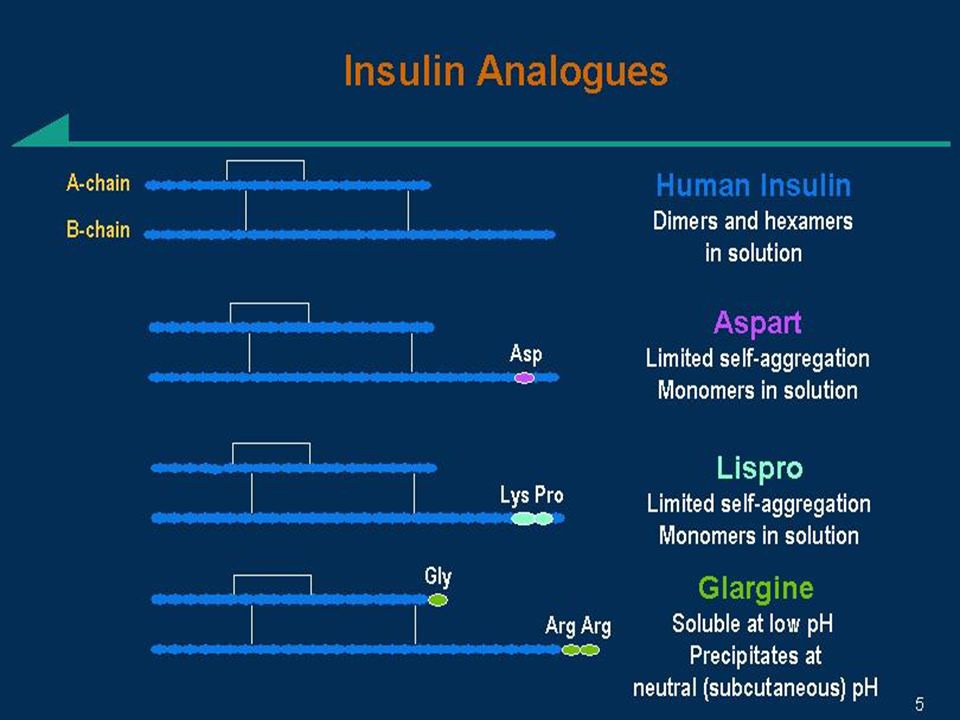
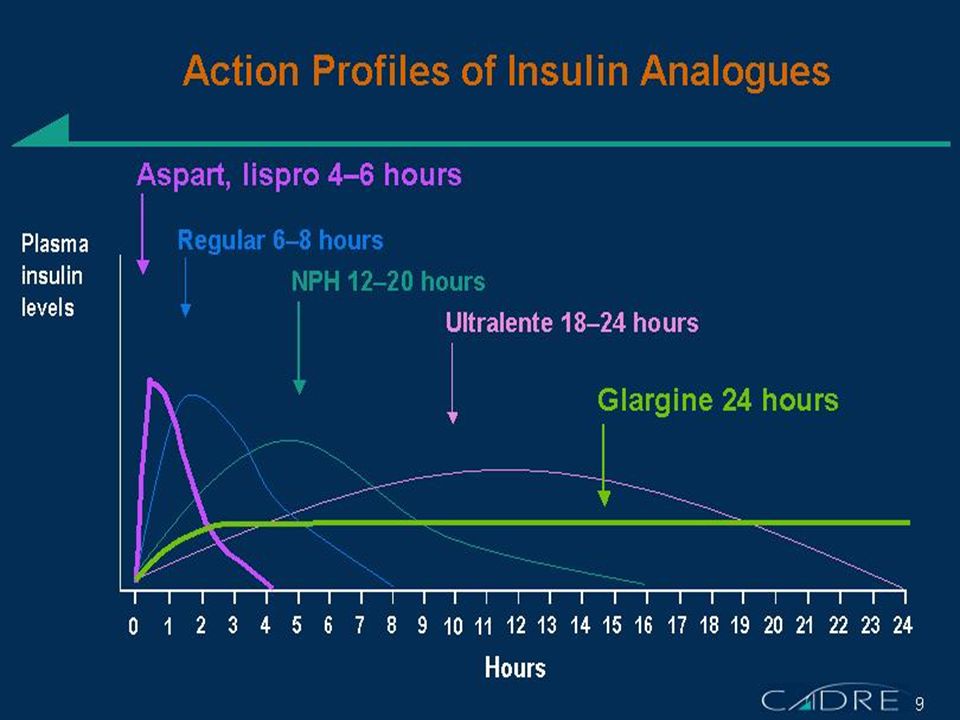
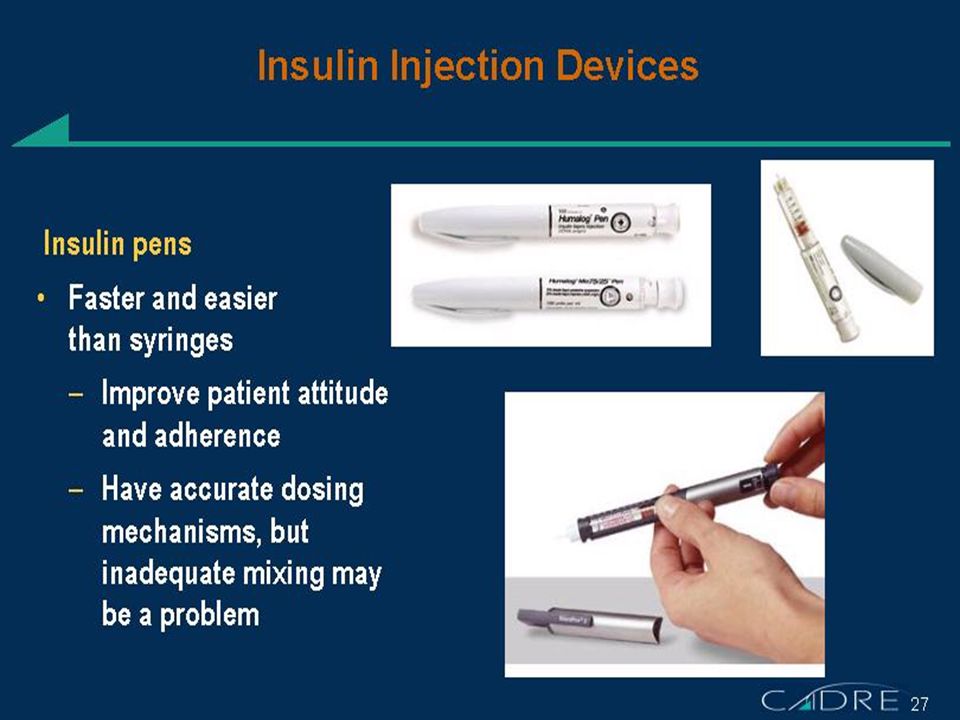
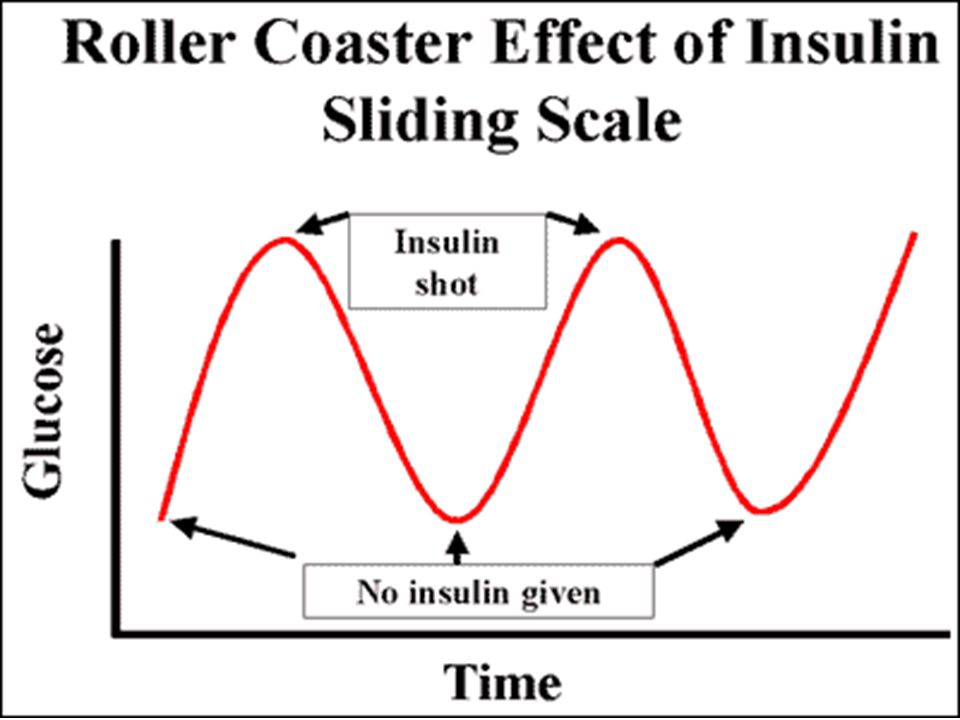
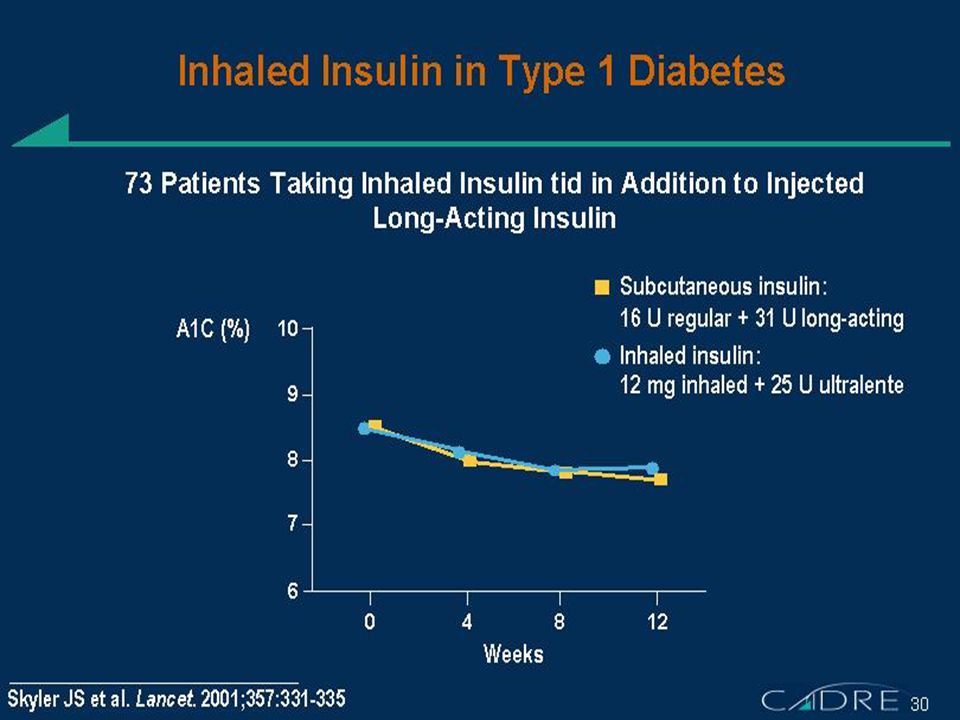






. Who needs screening for DM? Age >45 Obese – BMI >25 1 st degree relative with DM Racial groups: –African American –Hispanic American.>")



. 2 Insulin Learning outcomes >Understand the difference between insulin therapy in type 1 diabetes as compared to.>")









>")