Download presentation
Presentation is loading. Please wait.

1
Critical Care

2
A 56 year old wm, s/p AAA repair, in the ICU on the vent,with the following persistent hypotension despite fluids and pressors PCWP - 20 CVP15 hyponatremia hypoglycemia Dx and management?

3
Adrenal Insufficiency Random cortisol level of less than 20µg/dl is suggestive Cosyntropin test - 250 µg of cosyntropin Check cortisol level at 30 minutes Failure to increase greater than 9 µg is diagnostic Administer Dexamethasone - it does not affect cosyntropin test

4
Label the axis on the following graph Delivery dependent Delivery independent X Y

5
CaO2 = 1.34 x Hgb x SaO2 + ( 0.0032 x PaO2 ) DO2 = CaO2 x C.O VO2 = C(a-v)O2 x C.O
 DO2 = CaO2 x C.O VO2 = C(a-v)O2 x C.O")
6
Oxygen-hemoglobin disociation curve What is P50 ? Factors that shift curve to the right ?

7
Oxygen-hemoglobin disociation curve P50 P50 - the partial pressure of oxygen at which hemoglobin is 50% saturated with oxygen

8
AVP( ADH) is secreted in response to what?
 is secreted in response to what")
9
Increased serum osmolality and hypovolemia ADH increases water permeability and passive sodium transport to the distaltubule, allowing increased water reabsorption

10
Which of the following precludes a diagnosis of brain death? A. Uremia B. Hypothermia below 32.2 C C. Systemic blood pressure of 70/40 mmHg D. Hypercarbia with a PaCO 2 greater than 60mm Hg with no respiratory response Answer: A, B, C

11
Brain death Def – Irreversible cessation of all functions of the brain, including brain stem 1 st – Exclude reversible causes of coma, i.e. sedation, hypothermia, neuromuscular blockage, shock 2 nd – Clinically unresposive to pain, absent brainstem reflexes and positive apnea test Or flow study of blood to brain

12
A 45 year old female presents to the emergency room with nausea and vomiting and severe headache. She has been having these episodes frequently which last about an hour. A CT scan of the abd pelvis is obtained. You suspect it is a pheochromocytoma. What is your work up?

13
Stop any interfering medications Labetalol Tricyclic Antidepressant Levodopa or Methyldopa Benzodiazepines Labs: Best studies Plasma Free Metanephrines Test Sensitivity: 99% Test Specificity: 89% Urine Metanephrines (24 hour collections) Test Sensitivity: 76% Test Specificity: 94% Tests with lower efficacy (rarely used now) Urinary VMA Imprecise test Plasma Catecholamines (Norepinephrine, Epinephrine) Test Sensitivity: 85% Test Specificity: 80% Differential Diagnosis Primary Aldosteronism Carcinoid Malignant Hypertension Thyrotoxicosis Menopause Panic Disorder Medication withdrawal (e.g. Clonidine )
.")
14
Preoperative IV Fluids Alpha Blocker Phenoxybenzamine start - 20mg per day then increase by 10mg every 3 days until pt has postural hypotension Prazosin - 1mg QID BetaBlocker most pts do not need B-blocker reserved for tachyarrhytmias can exacerbate hypertensive crisis

15
You are about to do a laparoscopic cholecystectomy on a 25 year old female. The nurse anesthesist calls you into the room. She states that the patient has a temperature of 104.5 deg,HR of 132 and high ETCO2 This came on right after induction. What is your most likely diagnosis and management of this patient ?

16
↑ End tidal CO2 Tachycardia Fever 2°C per hour Cyanosis Mottling of skin Tachypnoea Arrhythmias Rigidity Sweating Hypercarbia Labile blood pressure Intense masseter spasm Ice packs Cooling blankets Fans Cold intravenous fluids Intragastric, intracystic cooling Peritoneal dialysis using cold diasylate Extracorporeal cooling if equipment is available Core temperature Arterial line and CVP line Urinary catheter ECG Pulse oximetry & capnography Blood gases Serum glucose Serum potassium Blood for CPK Urine for myoglobin Signs and Symptoms Active Cooling Monitoring Malignant Hyperthermia Terminate anaesthesia and surgery as soon as possible Hyperventilate with 100% oxygen Give Dantrolene Transfer to ICU as soon as possible

17
Malignant Hyperthermia DANTROLENE 2.5 mg/kg IV Repeat as required at 5.10 min intervals to a maximum cumulative dose of 10 mg/kg. Favorable response indicated by: (a) fall in heart rate (b) abolition of arrhythmia (c) decline in body temperature (d) reduced muscle tone ARRHYTHMIAS If these persist despite Dantrolene give: PROCAINAMIDE 1 mg/kg/ml IV Maximum dose: 15 mg/kg ACIDOSIS Correction with SODIUIM BICARBONATE 0.5 - 1.0 mmol/kg/dose IV Repeated as necessary HYPERKALAEMIA Control if necessary using glucose and INSULIN 0.1 units/kg in 2 ml/kg 50% dextrose IV URINE OUTPUT MANNITOL 0.5 - 1.0 g/kg (2.5 - 5ml/kg of 20% solution) and/or FUROSEMIDE 1 mg/kg IV to maintain urine output (> 1 ml/kg/hr)
 fall in heart rate (b) abolition of arrhythmia (c) decline in body temperature (d) reduced muscle tone ARRHYTHMIAS If these persist despite Dantrolene give: PROCAINAMIDE 1 mg/kg/ml IV Maximum dose: 15 mg/kg ACIDOSIS Correction with SODIUIM BICARBONATE mmol/kg/dose IV Repeated as necessary HYPERKALAEMIA Control if necessary using glucose and INSULIN 0.1 units/kg in 2 ml/kg 50% dextrose IV URINE OUTPUT MANNITOL g/kg ( ml/kg of 20% solution) and/or FUROSEMIDE 1 mg/kg IV to maintain urine output (> 1 ml/kg/hr).")
18
You are called to see a pt post-op in the ICU, this is the tracing on the monitor. Case 1. BP 70, HR160 Case 2.BP125/67, HR86

19
Atrial Fibrillation Irregular P waves > 300/min, irregular ventricular rhythm Associated Conditions: MI.HTN,hypoxia,Hyperthyroidism,electrolyte imbalance, pulmonary embolus If Unstable ( Case 1) Cardioversion – 200 – 360 J Initial Therapy Diltiazem 0.25mg/kg, then 10-15mg/hr Digoxin 0.5mg, then 0.25mg Q2hrs Esmolol, procainamide, amiodarone Subsequent therapy Procainamide, Digoxin, anticoagulation
 Cardioversion – 200 – 360 J Initial Therapy Diltiazem 0.25mg/kg, then 10-15mg/hr Digoxin 0.5mg, then 0.25mg Q2hrs Esmolol, procainamide, amiodarone Subsequent therapy Procainamide, Digoxin, anticoagulation")
20
A 45 year old male with gastric outlet obstruction, has had an NG tube in for six days. His avg daily out put is 1500cc per day. On the sixth day you realize that the intern has not been replacing the NG output. Inadequate or no replacement of nasogastric suctioning would result in what disturbance?

21
Hypokalemic,hypochloremic metabolic alkalosis PARADOXICAL ACIDURIA

22
1.Adequate volume status and hypotension refractory to inotropic agents 2.Distended neck veins, distant heart sounds, and hypotension 3.Hypotension, appropriate volume, atrial fibrillation with a HR of 40 4.Hypotension and low right and left atrial pressures 5.Adequate volume, no mechanical defects, hypotension A.Inotropic agents B.Cardiac pacing C.Fluid administration D.Pericardiocentesis E.Intraaortic balloon pump Match the treatment 1.E 2.D 3.B 4.C 5.A

23
TNICU – PTD #2, Ex-lap, GradeII liver injury & splenectomy. R2 called at 0100 to see pt. RN states abdomen is tight. How do you work this up?

24
Abdominal Compartment Syndrome s hould be suspected and sought for in any multiple trauma patient who has undergone a period of profound shock and aggressive ressuscitation.Clinically fall in urine output elevated central venous pressure. Increase peak airway pressure Decrease pulm compliance The diagnosis confirmed by measurement of intra-abdominal pressure.

25
Pt with long cardiac history, PAC placed pre-op for large ventral hernia repair. 1 st – CI 1.4 SVR 880 PWP 9 CVP 6 2 nd – CI 1.6 SVR 1000 PWP 15 CVP11 Vitals: BP 110/55, HR 128 Which Inotropic agent do you want to use and why?

26
Milrinone Dose:0.3 – 0.75ug/kg/min2.0 – 20ug/kg/min Mechanism:Phosphodiesterase inhibitorB1,2,α Cardiac contractility: Heart rate:No change Preload: SVR: Oxygen delivery: Dobutamine

27
55 year old on trauma service with severe watery, foul smelling diarrhea, WBC 40,000, 15 bands. Colonoscopy showed the following.

28
Pseudomembranous Colitis -Pseudomembranes compromised of fibrin, mucus and necrotic epithelial cells -Mostly in rectosigmoid -Accessible to sig-scope -C.diff toxinis agent responsible -found in 90 -100% of Pts with Pseudomembranous colitis -Mortality 20% - if untreated -Progression – perforation, toxic megacolon TREATMENT: Flagyl – 250mg PO/IV Q 6 hrs – 7 – 10days If unsuccessful Vancomycin – 125 mg Q6 hrs ( PO only )
")
29
A 17 year old male, multiple GSW, Blood loss ~ 2000cc, rapid respiration, weak pulse, confused, skin is cold and clammy and pale. What Class of hemorrhagic shock ?

30
Classes of Hemorrhage >35%4 25-35% 3 15-25% 2 <15%1 Resp. Volume Resp. Rate BP Pulse Pressure/ Strength Pulse Rate Vasocon- striction Blood Loss Stage Average Blood Volume = 5 L

31
65 year old male, restrained driver in MVC, Vitals :BP 90/40, HR 110

33
A B C D

35
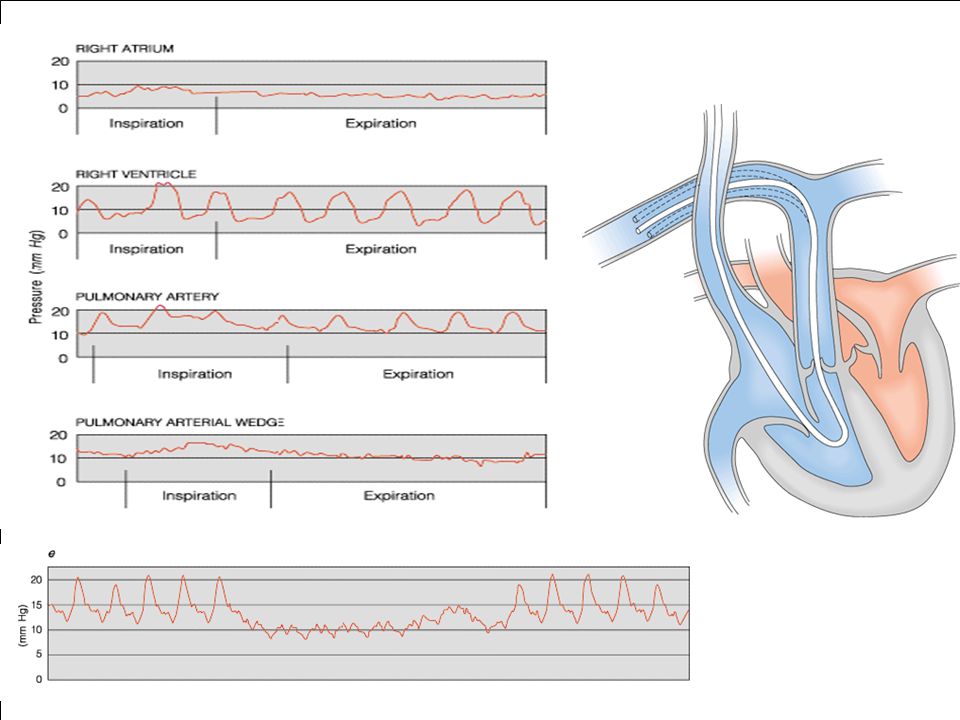
What is the significance of SvO2?

36
Causes for an increase in SvO2 decreased peripheral oxygen consumption increased peripheral shunting ( e.g sepsis. cyanide toxicity, hypothermia. increased peripheral shunting ( e.g sepsis. cyanide toxicity, hypothermia. An SvO2 of 75% is usually quoted as the normal value. A range of 63-77% is acceptable A range of 63-77% is acceptable under normal conditions, tissues extract 25% of the oxygen delivered ( the balloon at the end of the pulmonary artery catheter is inflated, the blood distal to the balloon stagnates, absorbs oxygen from the surrounding ventilated alveoli and becomes closer in saturation to arterial blood ) Mixed Venous Oxygen Saturation % - Condition 77% - Sepsis, shunting, hypothermia, cell poisoning, wedged catheter 66-77% - Normal range 60% - Cardiac decompensation 55% - Lactic acidosis 32% - Unconsciousness 20% - Permanent cell damage
 Mixed Venous Oxygen Saturation % - Condition 77% - Sepsis, shunting, hypothermia, cell poisoning, wedged catheter 66-77% - Normal range 60% - Cardiac decompensation 55% - Lactic acidosis 32% - Unconsciousness 20% - Permanent cell damage.")
37
Dietary protein – (UNN + 4gm) 6.25 What equation is this? What does the 6.25 and 4 stand for?
 6.25 What equation is this What does the 6.25 and 4 stand for")
38
1.Nitrogen balance 2.grams protein = 6.25(grams N) 1.4 = factor for skin and GI losses
 1.4 = factor for skin and GI losses")
39
Copius irrigation and immediate application of 2.5% calcium gluconate gel.

40
Hydrofluoric acid

Similar presentations
















 *Most Common Bases E.g bicarbonate (HCO3-) *Most.>")


