Download presentation
Presentation is loading. Please wait.

1
HEMOLYTIC ANEMIA HOSEA NJOKU 1405

2
CLASSIFICATION OF HEMOLYTIC ANEMIA
1. Intrinsic (intracorpuscular) abnormalities (A) HEREDITARY (i) Membrane abnormalities: Membrane skeleton: Spherocytosis, Elliptocytosis, Membrane lipids: Abetalipoproteinemia (ii) Enzyme deficiencies: Glycolytic enzymes: pyruvate kinase, hexokinase; Enzymes of HMP shunt: G-6PD (iii) Disorders of Hemoglobin: Deficient globin synthesis: Thalassemia syndromes; Structurally abnormal globin: Sickle cell anemia, unstable Hb (B) ACQUIRED Membrane defect: Paroxysmal Nocturnal Hemoglobinuria 2. Extrinsic (extracorpuscular) abnormalities (A) ANTIBODY MEDIATED: Isohemagglutinins: Transfusion reactions, Erythroblastosis fetalis; Autoantibodies: idiopathic drug- associated, SLE (B) MECHANICAL TRAUMA: Microangiopathic hemolytic anemias: TTP, DIC, Defective cardiac valves (C) INFECTIONS: Malaria
 abnormalities. (A) HEREDITARY. (i) Membrane abnormalities: Membrane skeleton: Spherocytosis, Elliptocytosis, Membrane lipids: Abetalipoproteinemia. (ii) Enzyme deficiencies: Glycolytic enzymes: pyruvate kinase, hexokinase; Enzymes of HMP shunt: G-6PD. (iii) Disorders of Hemoglobin: Deficient globin synthesis: Thalassemia syndromes; Structurally abnormal globin: Sickle cell anemia, unstable Hb. (B) ACQUIRED. Membrane defect: Paroxysmal Nocturnal Hemoglobinuria. 2. Extrinsic (extracorpuscular) abnormalities. (A) ANTIBODY MEDIATED: Isohemagglutinins: Transfusion reactions, Erythroblastosis fetalis; Autoantibodies: idiopathic drug- associated, SLE. (B) MECHANICAL TRAUMA: Microangiopathic hemolytic anemias: TTP, DIC, Defective cardiac valves. (C) INFECTIONS: Malaria.")
4
BASIC FEATURES Abnormal and accelerated destruction of red cells and, in some anemias, their precursors Increased breakdown of hemoglobin, which may result in: increased bilirubin level (mainly indirect-reacting) with jaundice increased fecal and urinary urobilinogen Hemoglobinemia, methemalbuminemia, hemoglobinuria and hemosiderinuria (where there is significant intravascular hemolysis). Bone marrow compensatory reaction: Erythroid hyperplasia with accelerated production of red cells, reflected by reticulocytosis, and slight macrocytosis in peripheral blood Expansion of bone marrow in infants and children with severe chronic hemolysis - changes in bone configuration visible on X-ray
 with jaundice. increased fecal and urinary urobilinogen. Hemoglobinemia, methemalbuminemia, hemoglobinuria and hemosiderinuria (where there is significant intravascular hemolysis). Bone marrow compensatory reaction: Erythroid hyperplasia with accelerated production of red cells, reflected by reticulocytosis, and slight macrocytosis in peripheral blood. Expansion of bone marrow in infants and children with severe chronic hemolysis - changes in bone configuration visible on X-ray.")
5
CLINICAL FEATURES OF HEMOLYTIC ANEMIA
PALLOR JAUNDICE SPLENOMEGALY

6
GLOBIN > Amino Acids
Heme > Iron and Protoporphyrin Protoporphyrin > Unconjugated bilirubin.

7
Extravascular Hemolysis
RBC is broken down by the Reticuloendothelial cell > Liver , Spleen, Kidney. CLINICAL FEATURES OF EH anemia with splenomegaly Jaundice with unconjugated bilirubin Marrow hyperplasia with corrected reticulocyte count of >3%

8
INTRAVASCULAR HEMOLYSIS
Rbc Broken Down In Blood Vessels Hemoglobin Released Hb Binds To Haptoglobin CLINICAL FEATURES Hemoglobinemia hemoglobinuria hemosiderinuria decreased haptoglobin level in blood.

9
LABORATORY FEATURES -Anemia -reticulocytosis -increased serum iron
-antiglobulin coombs test is positive.

10
-Anisopoikilocytosis, sperocytosis
BLOOD SMEAR -Anisopoikilocytosis, sperocytosis -erythroblasts -schistocytes BONE MARROW SMEAR -erythroid hyperplasia

11
PROGNOSIS The prognosis for patients with hemolytic anemia depends on the underlying cause. Overall, mortality rates are low in hemolytic anemias. However, the risk is greater in older patients and patients with cardiovascular impairment. Morbidity depends on the etiology of the hemolysis and the underlying disorder, such as sickle cell anemia or malaria.

12
Heriditary Spherocytosis
Life span of RBC ↓10 to 20 days (normal: 120 days) Mutations: mostly affect spectrin, ankyrin, band 3,or band 4.2
 Mutations: mostly affect spectrin, ankyrin, band 3,or band 4.2.")
13
HERIDITARY ELIPTOCYTOSIS
Mutation in spectrin/band 4.1 Intrinsic defect with extravascular hemolysis

14
G6PD DEFICIENCY GSH PRODUCTION is impaired- GSH is supposed to stop oxidants generated by phagocytes during an infection. This resuults in hemolysis. Could also be caused by Fava beans. Oxidative stress causes the Hb to form heinz bodies.

15
PYRUVATE KINASE DEFICIENCY

16
HEMOGLOBINOPATHIES SICKLE CELL ANEMIA
Mutation in β-globin gene creates sickle hemoglobin (HbS) by the substitution of valine for glutamic acid at the 6th amino acid residue of β-globin
 by the substitution of valine for glutamic acid at the 6th amino acid residue of β-globin.")
17
SIICKLE CELL ANEMIA… Severe hemolytic anemia - life span of RBC only 20 days Microvascular obstructions (Vaso-occlusive crises) ↑ transit time for red cells through the microvasculature (sluggish blood flow in spleen and bone marrow) 90% HbS, 8% HbF, 2% HbA2, (No HbA)
 90% HbS, 8% HbF, 2% HbA2, (No HbA)")
18
INCREASES RISKS FOR SICKLING
Hypoxemia Acidosis Dehydration DECREASES RISKS FOR SICKLING HbF

20
B- THALASSEMIA Mutations leading to aberrant RNA splicing most common
no mature mRNA, complete failure of β-globin production (β0) New splice junctions in abnormal positions normal & abnormal splicing, some normal β-globin mRNA (β+) In β-globin promoter ↓transcription, some normal β-globin is synthesized (β+) “Stop” codons - No synthesis of β-globin (β0) Leading to poorly hemoglobinized RBC
 New splice junctions in abnormal positions. normal & abnormal splicing, some normal β-globin mRNA (β+) In β-globin promoter. ↓transcription, some normal β-globin is synthesized (β+) Stop codons - No synthesis of β-globin (β0) Leading to poorly hemoglobinized RBC.")
23
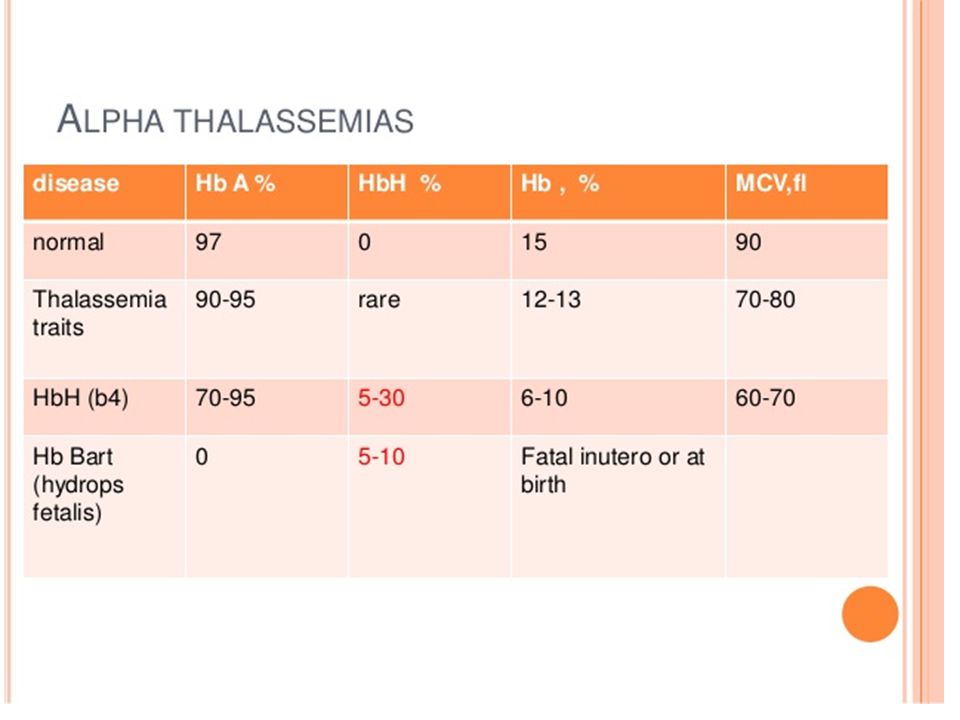
A-THALASSEMIA More common in South East Asians and Africans
Deletions involving one or more of the α-globin genes Severity of disease is proportional to missing α-globin genes

24
Paroxysmal Nocturnal Hemoglobinuria
Intrinsic defect with intravascular hemolysis In paroxysmal nocturnal hemoglobinuria, hemolysis is due to intravascular complement-mediated destruction of erythrocytes. > lack of CD55.

25
Immunohemolytic Anemias
WARM TYPE ANTIBODIES COLD TYPE ANTIBODIES

26
WARM TYPE ANTIBODIES CONFIRMATION- Direct coombs test.
Primary (idiopathic) Secondary: B cell neoplasms (e.g., chronic lymphocytic leukemia), Autoimmune disorders (e.g., systemic lupus erythematosus), Drugs(e.g., α-methyldopa, penicillin, quinidine) CONFIRMATION- Direct coombs test.
 Secondary: B cell neoplasms (e.g., chronic lymphocytic leukemia), Autoimmune disorders (e.g., systemic lupus erythematosus), Drugs(e.g., α-methyldopa, penicillin, quinidine) CONFIRMATION- Direct coombs test.")
27
COLD TYPE ANTIBODY. IgM against bodies own RBC
Infection- Mycoplasma Pneumonia, Infectious mononucleosis.

29
Hemolytic Disease of the Newborn
Maternal antibodies cross the placenta and react with fetal red cells causing hemolysis of fetal RBCs Rh Incompatibility: maternal allo-immunization to fetal red cell antigens (D antigen of Rh blood group) No problems during first pregnancy, but anti-Rh antibodies may cause problems in subsequent pregnancies
 No problems during first pregnancy, but anti-Rh antibodies may cause problems in subsequent pregnancies.")
30
INFECTION Malaria- intravascular hemolysis, severly called blackwater fever.

31
TREATMENT Definitive therapy depends on the cause:
Symptomatic treatment can be given by blood transfusion, if there is marked anemia. In severe immune-related hemolytic anemia, steroid therapy is sometimes necessary. Sometimes splenectomy can be helpful where extravascular hemolysis, or hereditary spherocytosis, is predominant (i.e., most of the red blood cells are being removed by the spleen

33
References Current Medical Diagnosis and Treatment 2009 By Stephen J. McPhee, Maxine A. Papadakis page 436

Similar presentations






. Senescent RBC is detected & cleared.>")
; FRCEdin; FRCSEdin>")
 Course code: MLHE-201 Supervisor: Prof. Dr Magda Sultan Date : 26/12/2013 Outcome : The student will know : -The types of.>")
 Hb is found in RBCs its main function is to transport O2 to tissues. Structure: 2 parts : heme + globin Globin: four globin chains (2 α.>")





 Course code: MLHE-201 Supervisor: Prof. Dr Magda Sultan Outcome : The student will know : -The types of hemolytic anemias.>")

 Hb is found in RBCs its main function is to transport O2 to tissues. Structure: 2 parts : heme + globin Globin: four chains. Heme: porphyrin.>")

 A. Hereditary 1. Membrane defect (spherocytosis, elliptocytosis)>")
