Download presentation
Presentation is loading. Please wait.

1
EUCAST European Committee on Antimicrobial Susceptibility Testing convened by European Society for Clinical Microbiology and Infectious Diseases (ESCMID) National European Breakpoint Committees and financed by ESCMID National Breakpoint Committees DG-SANCO of the European Union (3 year grant from May 2004)
 National European Breakpoint Committees and financed by ESCMID National Breakpoint Committees DG-SANCO of the European Union (3 year grant from May 2004)")
2
The objectives of EUCAST are to form in EUCAST, under the auspices of the European Society of Clinical Microbiology and Infectious Diseases", a professional network of (i) the national breakpoint committees and experts on antimicrobial susceptibility testing and (ii) industry involved in the production and marketing of antimicrobial agents or of in-vitro diagnostic medical devices used in antimicrobial susceptibility testing; to set common European breakpoints for surveillance of antimicrobial resistance; to identify national differences in clinical breakpoints and to harmonise breakpoints for existing and new antimicrobial drugs; to produce, disseminate and update a series of documents on the technology of in-vitro antimicrobial susceptibility testing, promoting standardisation of methods used in different parts of Europe and comparability of results obtained by different technologies; to encourage internal and external national and international quality assessment schemes; to collaborate with European and international groups concerned with antimicrobial susceptibility testing and/or the epidemiology of antimicrobial resistance; to advise European Community Institutions on the technology and interpretation of antimicrobial susceptibility testing; to work with groups outside Europe (eg NCCLS) to achieve international consensus on susceptibility testing; to devise and participate in educational and training programmes for antimicrobial susceptibility testing.
 the national breakpoint committees and experts on antimicrobial susceptibility testing and (ii) industry involved in the production and marketing of antimicrobial agents or of in-vitro diagnostic medical devices used in antimicrobial susceptibility testing; to set common European breakpoints for surveillance of antimicrobial resistance; to identify national differences in clinical breakpoints and to harmonise breakpoints for existing and new antimicrobial drugs; to produce, disseminate and update a series of documents on the technology of in-vitro antimicrobial susceptibility testing, promoting standardisation of methods used in different parts of Europe and comparability of results obtained by different technologies; to encourage internal and external national and international quality assessment schemes; to collaborate with European and international groups concerned with antimicrobial susceptibility testing and/or the epidemiology of antimicrobial resistance; to advise European Community Institutions on the technology and interpretation of antimicrobial susceptibility testing; to work with groups outside Europe (eg NCCLS) to achieve international consensus on susceptibility testing; to devise and participate in educational and training programmes for antimicrobial susceptibility testing.")
3
EUCAST EUCAST General Committee: - one representative, appointed by the appropriate medical associations, from each European country - one representative each from ISC and FESCI - Chairperson and Scientific secretary (appointed by ESCMID) - meets once a year at ECCMID - all Steering Committee proposals are referred to the General Committee for comments before decision EUCAST Steering Committee: - Chairperson and a Scientific Secretary (appointed by ESCMID) - one representative each from the European national breakpoint committees (presently 6) - two representatives from the EUCAST General Committee - Czech Republic and Greece 2002-2004 - Russia and Spain 2004 -2006 EUCAST industry email network - The network consists of all interested manufacturers of pharmaceuticals and susceptibility testing devices. All are invited to take an active part in EUCAST activities - Steering Committee proposals are referred to the industry network for comments before decision - relevant industry members can apply for inclusion on the email list by contacting the EUCAST secretariat

4
EUCAST General Committee 2004 Austria Prof Helmut Mittermayer Belgium Prof Jan Verhaegen Bosnia Dr Selma Uzunovic-Kamberovic Bulgaria Prof Krassimir Metodiev Croatia Dr Arjana Tambic-Andrasevic Czech Republic Dr Pavla Urbaskova Denmark Dr Niels Frimodt-Møller Estonia Dr Paul Naaber Finland Dr Antti Nissinen France Prof Claude-James Soussy Germany Prof Bernd Wiedemann Greece Prof Alkiviadis Vatopoulos Hungary Dr Éva Bán Iceland Dr Karl Gustaf Kristinsson Ireland Dr Martin Cormican Italy Prof Pietro Emanuele Varaldo Latvia Dr Arta Balode Lithuania Prof Arvydsa Ambrozaitis Netherlands Prof John Degener Norway Dr Martin Steinbakk Poland Prof Waleria Hryniewicz Portugal Prof Jose Melo Cristino Romania no official representative Russia Dr Olga Stetsiouk Serbia Dr Lazar Ranin Slovak Republic Prof. Milan Niks Slovenia Dr Jana Kolman Spain Dr Francisco Soriano Sweden Dr Barbro Olsson-Liljequist Switzerland Prof Jaques Bille Turkey Dr Deniz Gür UK Prof Alasdair MacGowan Yugoslavia no official representative ISC – Prof Paul Tulkens FESCI – Prof David Livermore Email network of industry with interest in antimicrobials Chairperson Gunnar Kahlmeter, Sweden Scientific Secretary Derek Brown, UK

5
EUCAST Steering Committee Membership Chairperson Gunnar Kahlmeter2002 - 05 Scientific Secretary Derek Brown 2002 - 05 BSAC (The UK) Alasdair MacGowan2002 - 05 CA-SFM (France) Fred Goldstein2002 - 05 CRG (The Netherlands) Johan W. Mouton2002 - 05 DIN (Germany) Arne Rodloff2002 - 05 NWGA (Norway) Martin Steinbakk2002 - 05 SRGA (Sweden) Anders Österlund 2002 - 05 General Committee rep Olga Stetsiouk (Russia)2004 - 06 General Committee rep Francisco Soriano (Spain) 2004 - 06
 Arne Rodloff NWGA (Norway) Martin Steinbakk SRGA (Sweden) Anders Österlund General Committee rep Olga Stetsiouk (Russia) General Committee rep Francisco Soriano (Spain)")
6
EUCAST Subcommittee on Antifungal Susceptibility Testing EUCAST Subcommittee on Antifungal Susceptibility Testing (EUCAST AFST) develop reference methods for antifungal susceptibility testing set breakpoints for antifungal drugs Financed through EUCAST EUCAST processes for breakpoint setting, decisions and consultation
 develop reference methods for antifungal susceptibility testing set breakpoints for antifungal drugs Financed through EUCAST EUCAST processes for breakpoint setting, decisions and consultation")
7
EUCAST publications 1.European Committee on Antimicrobial Susceptibility Testing. (2000). Terminology relating to methods for the determination of susceptibility of bacteria to antimicrobial agents. EUCAST Definitive Document E.Def 1.2. Clinical Microbiology and Infection 6, 503-8. 2.European Committee on Antimicrobial Susceptibility Testing. (2000). Determination of antimicrobial susceptibility test breakpoints. EUCAST Definitive Document E.Def 2.1. Clinical Microbiology and Infection 6, 570-2. 3.European Committee on Antimicrobial Susceptibility Testing. (2000). Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by agar dilution. EUCAST Definitive Document E.Def 3.1. Clinical Microbiology and Infection 6, 509-15. 4.European Committee on Antimicrobial Susceptibility Testing. (2001). Linezolid breakpoints. EUCAST Definitive Document E.Def 4.1. Clinical Microbiology and Infection 7, 283-4. 5.European Committee on Antimicrobial Susceptibility Testing. (2003). Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by broth microdilution. EUCAST Discussion Document E.Def 5.1. Clinical Microbiology and Infection 9 (issue 7 insert) 1-10. 6.Ridgway, G.L., Bébéar, C., Bébéar, C.M, et al. (2001). Antimicrobial susceptibility testing of intracellular and cell-associated pathogens. EUCAST Discussion Document E.Dis 6.1. Clinical Microbiology and Infection 7 (issue 12 insert),1-10. 7.Rodriguez-Tudela, J.L., Barchiesi, F., Bille, J. et al. (2003). Determination of minimum inhibitory concentrations by broth microdilution of fermentative yeasts. EUCAST Discussion Document E.Dis 7.1. Clinical Microbiology and Infection 9 (issue 8 insert), 1-8. 8.Drobniewski, F. (2002). Antimicrobial susceptibility testing of Mycobacterium tuberculosis. EUCAST Discussion Document E.Dis 8.1. Clinical Microbiology and Infection 8 (issue 10 insert),1-10. 9.Kahlmeter G, Brown DFJ, Goldstein FW et al. (2003) European harmonization of MIC breakpoints for antimicrobial susceptibility testing of bacteria. Journal of Antimicrobial Chemotherapy 52, 145-148. Discussion documents will be posted on the EUCAST website for comments and after a period of consultation they will be submitted for publication as Definitive Documents in CMI. Following publication they will also be available on the EUCAST website (www.eucast.org).www.eucast.org
. Terminology relating to methods for the determination of susceptibility of bacteria to antimicrobial agents. EUCAST Definitive Document E.Def 1.2. Clinical Microbiology and Infection 6, European Committee on Antimicrobial Susceptibility Testing. (2000). Determination of antimicrobial susceptibility test breakpoints. EUCAST Definitive Document E.Def 2.1. Clinical Microbiology and Infection 6, European Committee on Antimicrobial Susceptibility Testing. (2000). Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by agar dilution. EUCAST Definitive Document E.Def 3.1. Clinical Microbiology and Infection 6, European Committee on Antimicrobial Susceptibility Testing. (2001). Linezolid breakpoints. EUCAST Definitive Document E.Def 4.1. Clinical Microbiology and Infection 7, European Committee on Antimicrobial Susceptibility Testing. (2003). Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by broth microdilution. EUCAST Discussion Document E.Def 5.1. Clinical Microbiology and Infection 9 (issue 7 insert) Ridgway, G.L., Bébéar, C., Bébéar, C.M, et al. (2001). Antimicrobial susceptibility testing of intracellular and cell-associated pathogens. EUCAST Discussion Document E.Dis 6.1. Clinical Microbiology and Infection 7 (issue 12 insert), Rodriguez-Tudela, J.L., Barchiesi, F., Bille, J. et al. (2003). Determination of minimum inhibitory concentrations by broth microdilution of fermentative yeasts. EUCAST Discussion Document E.Dis 7.1. Clinical Microbiology and Infection 9 (issue 8 insert), Drobniewski, F. (2002). Antimicrobial susceptibility testing of Mycobacterium tuberculosis. EUCAST Discussion Document E.Dis 8.1. Clinical Microbiology and Infection 8 (issue 10 insert), Kahlmeter G, Brown DFJ, Goldstein FW et al. (2003) European harmonization of MIC breakpoints for antimicrobial susceptibility testing of bacteria. Journal of Antimicrobial Chemotherapy 52, Discussion documents will be posted on the EUCAST website for comments and after a period of consultation they will be submitted for publication as Definitive Documents in CMI. Following publication they will also be available on the EUCAST website (")
8
EUCAST websites are found at www.eucast.org The EUCAST websites are accessed via www.eucast.org This is a section of the official ESCMID website giving details of all EUCAST activities including - constitution - organisation - committee member lists - meetings - EUCAST documents - clinical MIC breakpoint tables - MIC distributions for wild type bacteria and fungi - epidemiological MIC cut-off values

9
www.eucast.org This is the first screen of the EUCAST general website found at www.eucast.org. www.eucast.org

10
This is the first screen of the EUCAST program for the display of wild type MIC distributions in microorganisms. Choose to display in English, French or German. The link to the programme is found on www.eucast.org

11
Specify the drug or the bug (never both) - after a few seconds a table of MIC-distributions is shown. Click on any species in the left hand column to display the data as a bar chart, with EUCAST epidemiological cut-off values and harmonised European clinical breakpoints.

12
EUCAST wild type MIC distributions and epidemiological cut-off values – the concept JAC 2003; 52: 145-148 EUCAST developed the concept of antimicrobial wild type MIC distributions and epidemiological cut-off values (JAC 52:145-148, 2003). Software was created to receive and display large volumes of MIC data for bacteria and fungi over the Internet. It is freely available at http://www.eucast.org. Distributions are displayed in an aggregated format. Tables and graphs show the part of the MIC distribution which, when EUCAST defines the ”epdemiological cut-off value”, is defined as the ”wild type distribution”. The epidemiological cut-off value separating microorganisms without (wild type) and with acquired or mutational resistance (non-wild type) and clinical breakpoints are, if defined, shown on the bottom line of the graph. The epidemiological cut-off value (left hand lower corner) is shown as WT≤ X mg/L. The clinical breakpoints (right hand lower corner) are shown as S≤ Y mg/L and R> Z mg/L.
 and with acquired or mutational resistance (non-wild type) and clinical breakpoints are, if defined, shown on the bottom line of the graph. The epidemiological cut-off value (left hand lower corner) is shown as WT≤ X mg/L. The clinical breakpoints (right hand lower corner) are shown as S≤ Y mg/L and R> Z mg/L..")
13
The wild type MIC distributions provide 1.reference material for committees involved in decisions on clinical breakpoints 2.reference material for epidemiological cut-off values for antimicrobial resistance surveillance 3.reference MIC ranges of wild type organisms for a wide spectrum of species and antimicrobials 4.an international reference for calibration of antimicrobial susceptibility testing methods Use of EUCAST wild type MIC distributions

14
EUCAST wild type MIC distributions and epidemiological cut-off values – methods and data Origin of MIC data Each distribution is comprised of aggregated MIC data including individual MIC distributions from - publications in international journals - breakpoint committees - antimicrobial surveillance systems such as EARSS, SENTRY, the Alexander Project - pharmaceutical companies and susceptibility testing device manufacturers. Thus, unless otherwise specifically stated, distributions include results obtained with different methods. These methods do not give exactly the same results but the results rarely vary by more than one doubling dilution step. In this way the aggregated EUCAST MIC distributions contain the random variation between different investigators and the systematic variation seen between different methods. Origin of the organisms included in the MIC distributions The data are from tests on bacteria and fungi collected from man and animals, of any geographic origin and over a wide timeframe. MIC methods represented Species-specific distributions of MIC values collected from all over the world are included in the database. The distributions shown represent full range MIC values determined with methods described by EUCAST, BSAC (UK), CA-SFM (France), CRG (The Netherlands), DIN (Germany), NCCLS (USA), NWGA (Norway), and SRGA (Sweden) or methods calibrated to these methods (eg. commercial methods which give full range MIC values).
, CA-SFM (France), CRG (The Netherlands), DIN (Germany), NCCLS (USA), NWGA (Norway), and SRGA (Sweden) or methods calibrated to these methods (eg. commercial methods which give full range MIC values)..")
15
S. pneumoniae and ciprofloxacin MIC distributions This slide shows a section of the data set for S.pneumoniae and ciprofloxacin. Each MIC distribution is from a different investigator, surveillance program, breakpoint committee or pharmaceutical company. The median of the uni- or of the forst part of the multi- modal distribution has been marked in blue.

16
EUCAST wild type MIC distributions – templates for calibration of MIC determinations Laboratories which cannot fit their own MIC data to the the EUCAST reference distribution should look into the following possibilities: The method used for MIC determination in the local set of data is not adequately calibrated, The species identification is incomplete, There are too few determinations to allow identification of the part of the distribution that constitutes the wild type microorganisms. This usually corresponds to the four lowest dilution steps. Exclusion of data All submitted full-range MIC distributions have been accepted. There has been no systematic exclusion of data from one contributor or from one method. The contributions are screened by the EUCAST Steering Committee and less than 10% have been excluded from the aggregated distributions. However, all data are held in the database and are accessible to the Steering Committee. The most common reason for exclusion has been that the data were not full-range MICs so that a significant proportion of MICs were outside the tested range.

17
EUCAST wild type MIC distributions – why are only the MICs of wild type microorganisms displayed? The distributions consist of MIC-values determined over 30 years or more. While the wild type distribution does not change there may be major differences in resistance over time and between sources. Resistance frequencies obtained through the aggregated MIC distributions would not be representative of current antimicrobial resistance frequencies and would be both confusing and misleading. Thus once the epidemiological cut-off value has been determined by the EUCAST Steering Committee it blocks display of the non- wild type microorganisms (red bars, upper figure) and shows only the part representing the wild type (lower fig).
 and shows only the part representing the wild type (lower fig)..")
18
EUCAST wild type MIC distributions - what does ”Data not released for public use” in pull-down lists imply When selecting antimicrobials in the pull-down list, many agents are followed by the text "data not released for public use". This implies that data for the drug in question are present (fig) but are incomplete and require more data contributions. As EUCAST decisions on epidemiological cut-off values and clinical breakpoints are made for each group of agents, the tables and graphs are released for general use.
 but are incomplete and require more data contributions. As EUCAST decisions on epidemiological cut-off values and clinical breakpoints are made for each group of agents, the tables and graphs are released for general use..")
19
Everyone is invited to contribute data All who have full-range MIC data for bacteria or fungi are invited to contribute data as long as MICs are determined with an accepted standardised method, which should be named. Once entered on the database the data will not be identifiable as separate distributions but will help build the aggregate reference distributions. The biologically resistant (non-wild type) part of the distribution will be seen only by the EUCAST Steering Committee. Submitting data to the EUCAST database does not interfere with publication of data. Where can I get more information? Contact EUCAST – email addresses and information can be obtained through the EUCAST website at http://www.eucast.org EUCAST wild type MIC distributions – how to contribute data
 part of the distribution will be seen only by the EUCAST Steering Committee. Submitting data to the EUCAST database does not interfere with publication of data. Where can I get more information. Contact EUCAST – addresses and information can be obtained through the EUCAST website at EUCAST wild type MIC distributions – how to contribute data.")
20
Graph shown in the EUCAST program for display of MIC distributions of wild type bacteria. V alues >1% show on graph!

21
(1) To define epidemiological cut-off values
 To define epidemiological cut-off values")
22
(2) As a template for calibration of methodology (accuracy and imprecision). ”We have defined the result of antimicrobial susceptibility testing!”

23
(3) Reference MIC database for breakpoint setting - to avoid clinical breakpoints that divide wild type bacteria
 Reference MIC database for breakpoint setting - to avoid clinical breakpoints that divide wild type bacteria")
24
(4) As MIC reference database
 As MIC reference database")
25
1 Examples from the EUCAST wild type MIC distribution program.

26
EUCAST definitions of clinical breakpoints Clinically Susceptible (S) a microorganism is defined as susceptible by a level of antimicrobial activity associated with a high likelihood of therapeutic success a microorganism is categorized as susceptible (S) by applying the appropriate breakpoint in a defined phenotypic test system Clinically Intermediate (I) a microorganism is defined as intermediate by a level of antimicrobial activity associated with indeterminate therapeutic effect a microorganism is categorized as intermediate (I) by applying the appropriate breakpoints in a defined phenotypic test system Clinically Resistant (R) a microorganism is defined as resistant by a level of antimicrobial activity associated with a high likelihood of therapeutic failure. a microorganism is categorized as resistant (R) by applying the appropriate breakpoint in a defined phenotypic test system Clinical breakpoints may be altered with legitimate changes in circumstances Clinical breakpoints are presented as S x, y mg/L EUCAST has re-defined susceptible, intermediate and resistant and defined the terms wild type and non- wild type microorganism. The national breakpoint committees have also agreed on a common format for susceptible (S≤) and resistant (R>).
 by applying the appropriate breakpoint in a defined phenotypic test system Clinical breakpoints may be altered with legitimate changes in circumstances Clinical breakpoints are presented as S x, y mg/L EUCAST has re-defined susceptible, intermediate and resistant and defined the terms wild type and non- wild type microorganism. The national breakpoint committees have also agreed on a common format for susceptible (S≤) and resistant (R>)..")
27
EUCAST definitions of epidemiological cut off values Wild type (WT) a microorganism is defined as wild type (WT) for a species by the absence of acquired and mutational resistance mechanisms to the drug in question. a microorganism is categorized as wild type (WT) for a species by applying the appropriate cut-off value in a defined phenotypic test system. wild type microorganisms may or may not respond clinically to antimicrobial treatment. Microbiological resistance - non-wild type (NWT) a microorganism is defined as non-wild type (NWT) for a species by the presence of an acquired or mutational resistance mechanism to the drug in question. a microorganism is categorized as non-wild type (NWT) for a species by applying the appropriate cut-off value in a defined phenotypic test system. non-wild type microorganisms may or may not respond clinically to antimicrobial treatment. Epidemiological cut-off values will not be altered by changing circumstances. The wild type is presented as WT z mg/L
 for a species by applying the appropriate cut-off value in a defined phenotypic test system. wild type microorganisms may or may not respond clinically to antimicrobial treatment. Microbiological resistance - non-wild type (NWT) a microorganism is defined as non-wild type (NWT) for a species by the presence of an acquired or mutational resistance mechanism to the drug in question. a microorganism is categorized as non-wild type (NWT) for a species by applying the appropriate cut-off value in a defined phenotypic test system. non-wild type microorganisms may or may not respond clinically to antimicrobial treatment. Epidemiological cut-off values will not be altered by changing circumstances. The wild type is presented as WT z mg/L.")
28
EUCAST procedure for setting breakpoints The next 9 slides describe the EUCAST procedure for harmonising European breakpoints.

29
1. Data on dosing, formulations, clinical indications and target organisms are reviewed and differences which might influence breakpoints are highlighted Dosage BSAC UK CA-SFM France CRG Netherlands DIN Germany NWGA Norway SRGA Sweden Most common dose 500 x 2 oral 400 x 2 iv 500 x 2 oral 200 x 2 iv 250 x 2 oral 200 x iv 500 x 2 oral 200 x 2 iv 200-400 x 2 oral 400 x 2 iv 500 x 2 oral 400 x 2 iv Maximum dose schedule 750 x 2 oral 400 x 3 iv 750 x 2 oral 400 x 3 iv 750 x 2 oral 400 x 3 iv 750 x 2 oral 400 x 2 iv data pending 750 x 2 oral 400 x 3 iv Available formulationsoral, iv Clinical data There is clinical evidence for ciprofloxacin to indicate a poor response in systemic infections caused by Salmonellae with low-level fluoroquinolone resistance (MIC>0.064 mg/L) EUCAST has suggested that the epidemiological cut off value (S 0.064 mg/L) be used in Salmonellae systemic infections. These strains are best found using a nalidixic acid 30 µg screen disc in routine susceptibility testing. There is agreement in EUCAST that ciprofloxacin activity against Enterococci and Streptococci, including S.pneumoniae, is insufficient to categorize wild type bacteria “susceptible”. National breakpoint committees
 EUCAST has suggested that the epidemiological cut off value (S mg/L) be used in Salmonellae systemic infections. These strains are best found using a nalidixic acid 30 µg screen disc in routine susceptibility testing. There is agreement in EUCAST that ciprofloxacin activity against Enterococci and Streptococci, including S.pneumoniae, is insufficient to categorize wild type bacteria susceptible . National breakpoint committees.")
30
2. Multiple MIC-distributions are collected, the wild type MIC distribution is defined and tentative epidemiological cut-off values determined (WT < X mg/L) Epidemiological cut off: WT<2.0
 Epidemiological cut off: WT<2.0.")
31
3. Existing national clinical breakpoints are compared Breakpoints prior to harmonisation (mg/L) S BSACCA-SFMCRGDINNWGASRGANCCLS General breakpointsND1/2 0.125/21/2 Species related breakpointsnot yetno Enterobacteriaceae1/10.12/20.12/11/2 Pseudomonas spp.1/4ND1/11/2 Acinetobacter spp.1/11/2 Staphylococci1/10.12/20.06/21/2 Streptococci1/1excluded0.12/2 excl S. pneumoniae2/2 (I)*excluded0.12/2 (I)* excl Enterococciexcluded 0.12/2 1/2 Haemophilus/Moraxella spp.1/10.12/0.50.12/0.251/- Corynebacteriaexcl N. Meningitidis1/10.06/0.120.03/0.25 N. Gonorrhoeae0.06/-0.06/10.06/0.120.06/0.250.06/0.5 P. MultocidaND 0.12/0.25 AnaerobesexcludedNDexcluded Campylobacter spp.1/1 Helicobacter pylori2/2no Ciprofloxacin was used in this example:
 S BSACCA-SFMCRGDINNWGASRGANCCLS General breakpointsND1/ /21/2 Species related breakpointsnot yetno Enterobacteriaceae1/10.12/20.12/11/2 Pseudomonas spp.1/4ND1/11/2 Acinetobacter spp.1/11/2 Staphylococci1/10.12/20.06/21/2 Streptococci1/1excluded0.12/2 excl S. pneumoniae2/2 (I)*excluded0.12/2 (I)* excl Enterococciexcluded 0.12/2 1/2 Haemophilus/Moraxella spp.1/10.12/ /0.251/- Corynebacteriaexcl N. Meningitidis1/10.06/ /0.25 N. Gonorrhoeae0.06/-0.06/10.06/ / /0.5 P. MultocidaND 0.12/0.25 AnaerobesexcludedNDexcluded Campylobacter spp.1/1 Helicobacter pylori2/2no Ciprofloxacin was used in this example:.")
32
4. Using available PK/PD data, Monte Carlo simulations are performed and a tentative breakpoint calculated ”Minimum requirement for S-category” is that the high MIC value of the wild type MIC-distribution is consistent with the MIC derived from the PK/PD index needed for optimal efficacy based on free drug”. Johan – can you suggest one or two illustrations?

33
5. Clinical data relating outcome to MIC-values and resistance mechanisms are assessed in relation to the tentative breakpoint

34
6. Tentative breakpoints are checked against target species wild type MIC distributions to avoid splitting the wild type Epidemiological cut off: WT<2.0 <2 mg/L To permit reproducible susceptibility testing, splitting of the wild type must be avoided … thus break-points of 0.25, 0.5, 1.0 and 2.0 mg/L were not acceptable. Since S≤4 mg/L was considered too high it was decided to set the break- point at S≤0.125 mg/L, rendering wild type S.pneumoniae intermediately susceptible to ciprofloxacin.

35
8. Re-appraisal of tentative breakpoints following comments 7. Consultation process on tentative breakpoints - national committees - EUCAST general committee - pharmaceutical industry, AST device manufacturers - others via EUCAST website 9. Further consultation if required

36
Summary of EUCAST procedure for setting clinical breakpoints 1.Data on dosing, formulations, clinical indications and target organisms are reviewed and differences which might influence breakpoints are highlighted. 2.Multiple MIC-distributions are collected, the wild type MIC distribution is defined and tentative epidemiological cut-off values determined (WT < X mg/L). 3.Existing national clinical breakpoints are compared. 4.Using available PK/PD data, Monte Carlo simulations are performed and a tentative breakpoint calculated. ”Minimum requirement for S-category” is that the high MIC value of the wild type MIC-distribution is consistent with the MIC derived from the PK/PD index needed for optimal efficacy based on free drug”. 5.Clinical data relating outcome to MIC-values and resistance mechanisms are assessed in relation to the tentative breakpoint. 6.Tentative breakpoints are checked against target species wild type MIC distributions to avoid splitting the wild type. 7.Consultation process (national committees, EUCAST general committee and pharmaceutical industry and AST device manufacturers). 8.EUCAST clinical breakpoint tables are published on the internet (www.eucast.org) with links to tables and graphs of wild type distributions of MIC values.www.eucast.org
. 3.Existing national clinical breakpoints are compared. 4.Using available PK/PD data, Monte Carlo simulations are performed and a tentative breakpoint calculated. Minimum requirement for S-category is that the high MIC value of the wild type MIC-distribution is consistent with the MIC derived from the PK/PD index needed for optimal efficacy based on free drug . 5.Clinical data relating outcome to MIC-values and resistance mechanisms are assessed in relation to the tentative breakpoint. 6.Tentative breakpoints are checked against target species wild type MIC distributions to avoid splitting the wild type. 7.Consultation process (national committees, EUCAST general committee and pharmaceutical industry and AST device manufacturers). 8.EUCAST clinical breakpoint tables are published on the internet ( with links to tables and graphs of wild type distributions of MIC values.")
37
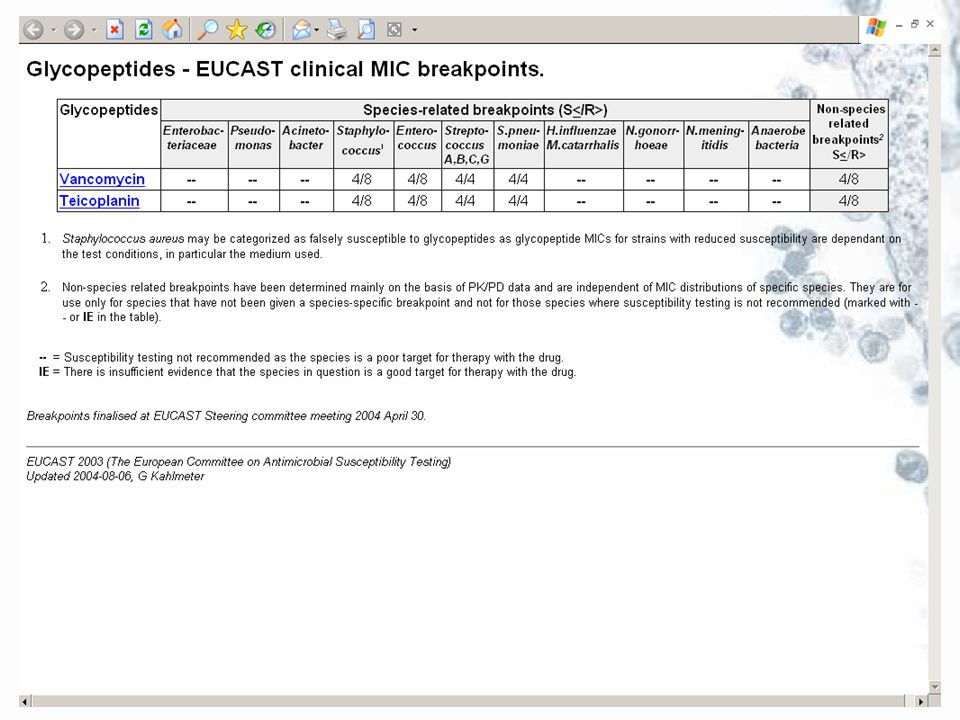
EUCAST breakpoint tables at www.eucast.org

41
How to implement EUCAST breakpoints The national breakpoint committees have committed themselves to implementing EUCAST breakpoints – which means that anyone using the national European systems will gradually adhere to the EUCAST breakpoint system Breakpoints as presented in EUCAST tables can be directly applied to MIC distributions (local and national surveillance, EARSS, etc) Systems for automated susceptibility testing can be set up with EUCAST MIC breakpoints.
 Systems for automated susceptibility testing can be set up with EUCAST MIC breakpoints.")
Similar presentations




 Antimicrobial susceptibility testing in Europe - the role of national breakpoint committees and EUCAST Gunnar.>")

 breakpoints – the impact on the BSAC recommendations Alasdair MacGowan Southmead Hospital BRISTOL.>")














