Download presentation
Presentation is loading. Please wait.

1
Compartment Syndromes Evaluation & Management Abdulaziz Al-Ahaideb Feb 16/2000 Subspecialty Rounds

2
2 Compartment Syndromes Definition Types Pathophysiology Etiology Clinical evaluation Diagnosis Management Complications

3
3 Definition An elevation of the interstitial pressure in a closed osteofascial compartment that results in micrvascular compromise.If left untreated will cause tissue damage. Compartments with relatively noncompliant fascial or osseous structures most commonly are involved,especially the anterior compartment of the leg and the volar compartment of the forearm.

4
4 Types of compartment syndrome Compartment syndromes can be classified as : acute compartment syndrome (ACS) or chronic compartment syndrome (CCS) depending on the cause of increased intra- compartmental pressure and the duration of symptoms
 or chronic compartment syndrome (CCS) depending on the cause of increased intra- compartmental pressure and the duration of symptoms")
5
5 Sites of Acute Compartment Syndrome Acute compartment syndrome can develop anywhere a skeletal muscle is surrounded by a substantial fascia. ACS may occur in foot, leg, thigh, buttocks, lumbar paraspinous muscles, hand, forearm, arm and shoulder.

6
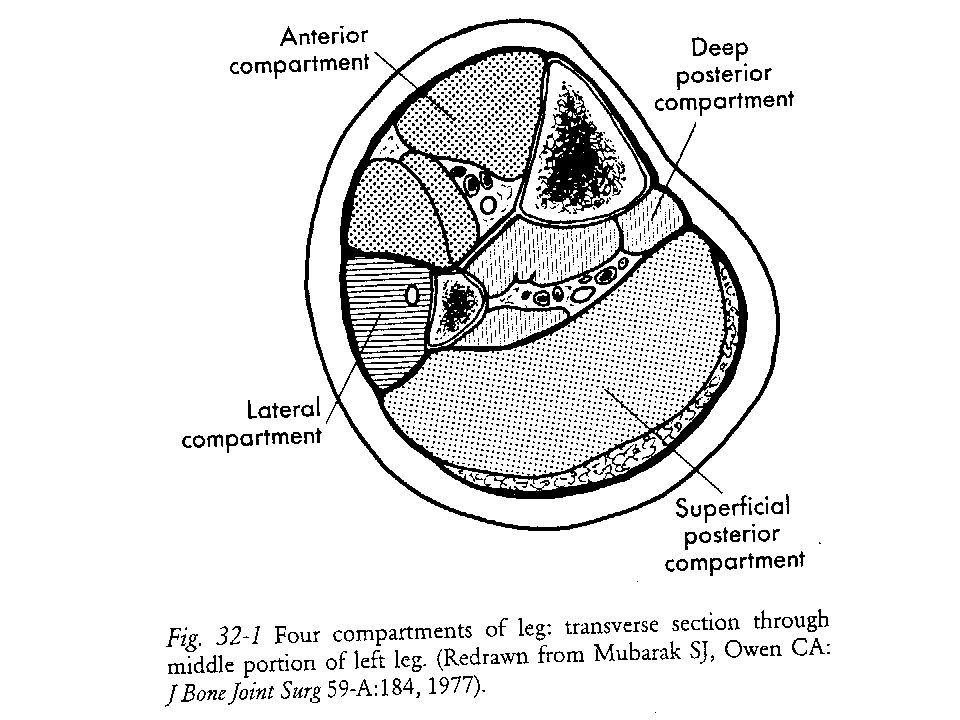
6 Compartments Foot 9 Leg 4 (anterior,lateral, sup & deep posterior ) Hand 4 Thigh 3 (anterior, posterior, medial ) Forearm 4 (sup &deep volar,dorsal, mobile wad of Henry)
 Hand 4 Thigh 3 (anterior, posterior, medial ) Forearm 4 (sup &deep volar,dorsal, mobile wad of Henry)")
7
7 Pathophysiology of ACS CS develops after prolonged elevated intra- compartmental pressure, which results from either externally applied or internally expanding pressure forces. Increased tissue pressure will decrease capillary blood flow leading to local tissue necrosis caused by O2 deprivation. Local blood flow (LBF) =Pa-Pv/R.
 =Pa-Pv/R..")
8
8 Pathophysiology of ACS The elevated intra-compartmental pressure increases the local venous pressure leading to narrowed arteriovenous perfusion gradient and compartment tamponade, resulting -if uncontrolled - in nerve injury and muscle ischemia

9
9 Etiology of ACS External Restriction of Compartment Size : casts, tight dressings, splints, lying on limb for long period, MAST, burn eschar, closure of fascial defect, lithotomy position, malfunctioning pneumatic boot

10
10 Etiology of ACS Internal Increase in Compartment Volume : factures (the most common ones are : In adults --- closed and open tibial shaft fx, distal radial fx In children --- radial head or neck fx, supracondylar fx, forearm fxs

11
11 Etiology of ACS Hemorrhage (e.g. due to vascular injury ) Coagulopathy (e.g. hemophilia, ASA overdose, thrombolytics, heparin infusion, sickle cell disease or trait ) Muscle edema (e.g. severe exercise, crush injury [trauma,alcohol,or drug- induced], trauma with or without fx )
 Muscle edema (e.g. severe exercise, crush injury [trauma,alcohol,or drug- induced], trauma with or without fx ).")
12
12 Etiology of ACS Surgically related (e.g. knee arthroscopy, tibial osteotomy without drainage, after epidural anesthesia ) Massive crystalloid infusion Ruptured Backer ’ s cyst Muscle hypertrophy ( androgens ) Rhabdomyolysis
 Massive crystalloid infusion Ruptured Backer ’ s cyst Muscle hypertrophy ( androgens ) Rhabdomyolysis.")
13
13 Etiology of ACS Intracompartmental fluid infusion (interosseosus infusion ) Capillary leak syndrome Intra-arterial injections of sclerosing agents Post – ischemic reperfusion
 Capillary leak syndrome Intra-arterial injections of sclerosing agents Post – ischemic reperfusion")
14
14 Clinical Evaluation of ACS History : Pain out of proportion to that expected with the injury Severe pain at rest Hyperesthesia or paresthesia Presence of a causing factor Mechanism of injury ( long bone fx, high- energy trauma, penetrating injuries, crush injury )
")
15
15 Clinical Evaluation of ACS Physical examination : Tightness of the involved compartment (tense) Pain with Passive stretching of those muscles passing through the compartment Hyperesthesia or paresthesia N.B. Paralysis, pallor or absent arterial pulse are late findings

16
16 Clinical Evaluation of ACS Follow-up exams are important to determine if any progression of symptoms exists If Pt complains of pain, determine if any neural compromise exists : sensory nerves begin to lose conductive ability, followed by motor nerves some nerves may reveal effects of increasing pressure others ( e.g. in the anterior compartment of the lower leg, the deep peroneal nerve quickly will be affected and sensation in the 1 st web space may be lost )
.")
17
17 Clinical Evaluation of ACS The diagnosis of ACS may be delayed in : patients with multiple injuries or altered consciousness and in children, in whom physical findings cannot be accurately documented and in patients with altered neurological function caused by vascular injuries,peripheral nerve injury,continuous epidural anesthesia or tourniquet palsy The 5Ps are present in an established ACS

18
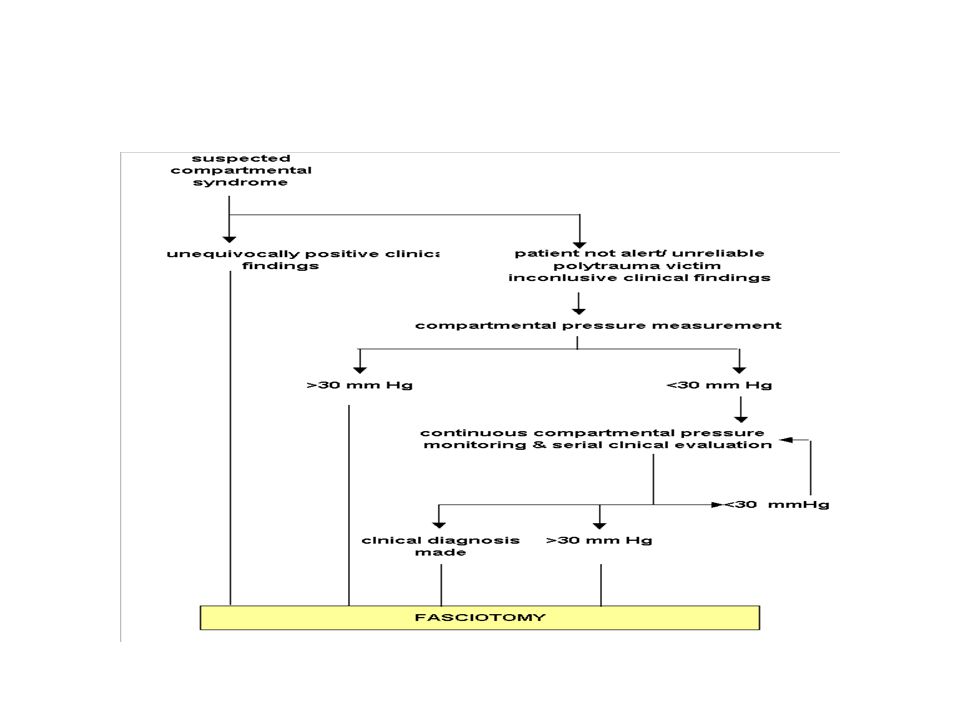
18 Clinical Evaluation of ACS High index of suspicion remains the cornerstone of diagnosing ACS If ACS is suspected and clinical examination is equivocal or inadequate, compartmental pressures should be measured Many surgeons use 30 mmHg (in normotensive pt) or when the ICP rises to a level 10 to 30 mmHg below the diastolic BP( in hypotensive pt) as the cutoff for performing fasciotomy (still an area of big controversy)
 or when the ICP rises to a level 10 to 30 mmHg below the diastolic BP( in hypotensive pt) as the cutoff for performing fasciotomy (still an area of big controversy)")
19
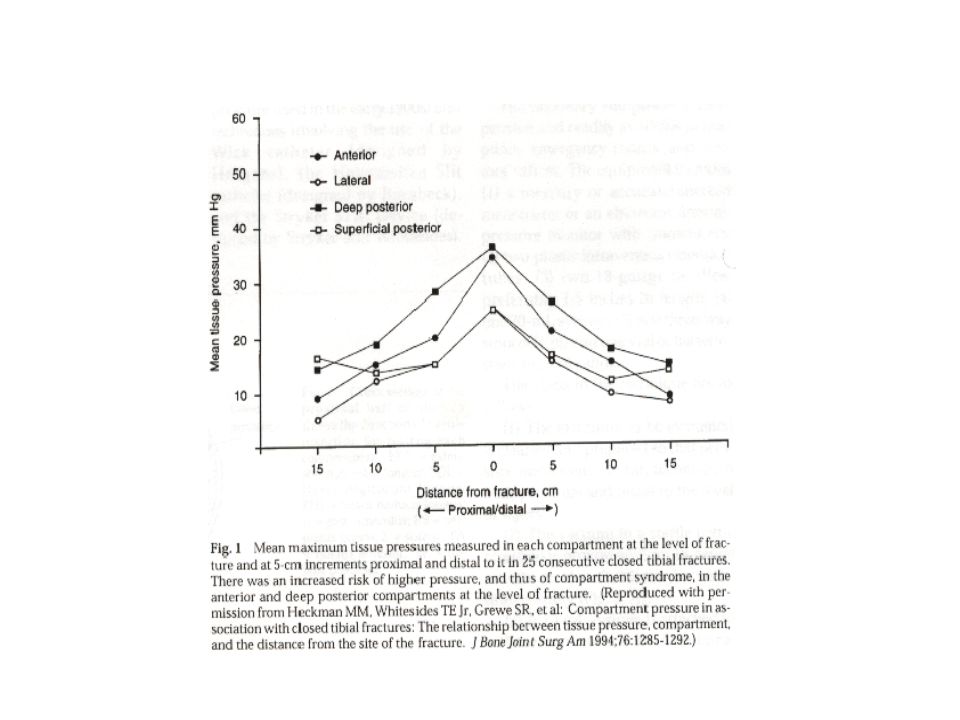
19 Clinical Evaluation of ACS The pressures in all compartments must be measured Compartment pressure measurement should be taken as close to the fracture site as possible since these measurements will give the highest readings. (see the diagram)
.")
21
21 DDx of ACS Cellulitis DVT Gas gangrene Necrotizing fasciitis Peripheral vascular injury Rhabdomyolysis

22
22 Management of ACS ICP can be measured using different devices : stryker hand-held slit catheter wick catheter fiberoptic transducer (Camino catheter) If the sophisticated methods are not available,,intravenous tubing, a three way stopcock, a syringe,a side-ported needle and a mercury manometer can be used
 If the sophisticated methods are not available,,intravenous tubing, a three way stopcock, a syringe,a side-ported needle and a mercury manometer can be used")
23
23 Management of ACS When an ACS is suspected,several procedures can be used to decrease the likelihood of development of a full-blown ACS these include : * Removal of the possible cause (release of tight dressings or circular constrictive bandages, splitting of casts, removal of MAST, cut the webril) * Correction of coagulopathy * Positioning of the limb at the level of the heart
 * Correction of coagulopathy * Positioning of the limb at the level of the heart")
24
24 Management of ACS * Cooling the limb * Treat systemic hypotension / shock * Hyperbaric oxygen ( still experimental ) * Use of mannitol (still experimental )
 * Use of mannitol (still experimental )")
25
25 Management of ACS If symptoms don ’ t resolve in 30 to 60 min after appropriate treatment,pressure measurement should be repeated,and,if equivocal, fasciotomy is indicated

27
27 Management of ACS The definitive treatment of acute compartment syndrome is FASCIOTOMY Procedure is done without a tourniquet,each potentially limiting envelope is opened over the entire length of the compartment, all muscle groups should be soft to palpation at the end of the procedure Muscle debridement should be kept to a minimum

28
28 Management of ACS After decompression, there is no immediate closure, skin is packed open with bulky dressing Care after decompression : sterile dressing (saline soaks ), splinting the limb in functional position Return to OR for 2 nd look in 2-5 days where any necrotic material is debrided. If no evidence of ms necrosis the skin is loosely closed. If closure is not accomplished,the debridement is repeated after another 72- h interval, after which skin closure or skin grafting can be performed

29
29 Management of ACS Skeletal fixation : external fixation, plates, IM nailing can all be applied at time of initial surgical decompression

30
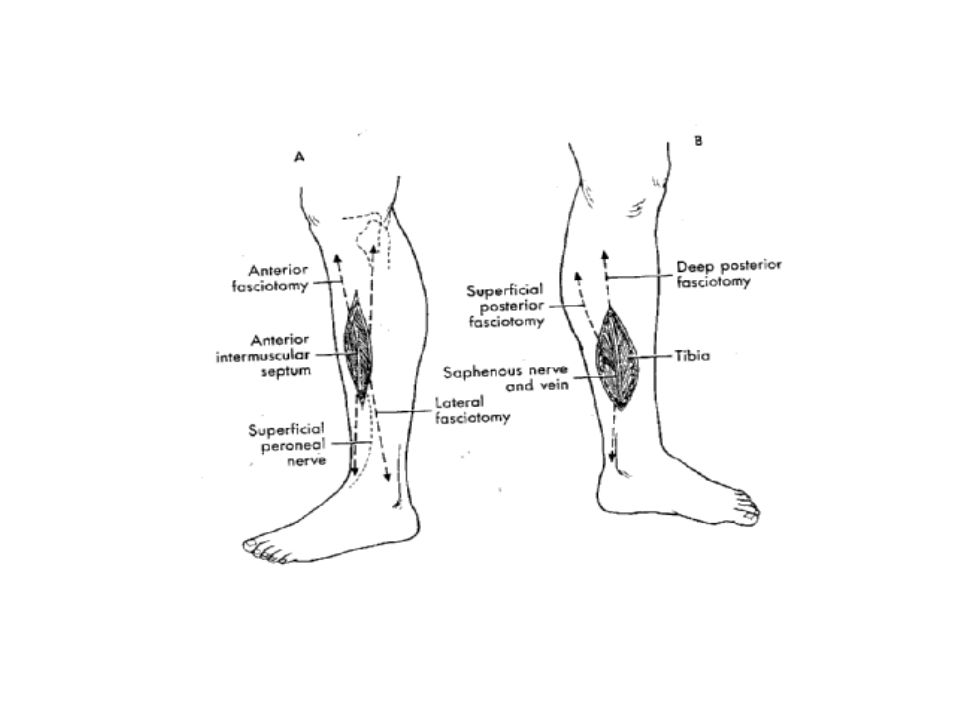
30 Management of ACS of the Leg Three approaches have been described for release of the compartments of the leg : Fibulectomy – a radical procedure and rarely if ever is indicated Single incision fasciotomy – may be useful if the soft tissue of the limb is not extensively distorted

31
31 Management of ACS of the leg Double – incision four compartment fasciotomy : is safer and more effective and generally should be used.

34
34 Prognosis Excellent to poor, depending on how quickly ACS is diagnosed and treated,, and whether or not complications develop

35
35 Complications of ACS Myonecrosis : happens after an ischemic insult of an 8 hours or more duration Rx fasciotomy + debridement of the muscles + neurolysis may lead to myoglobinuria and eventually renal failure. Diuresis ( by mannitol,diuretics or IV fluids ) should be prompted to increase the tubular flushing and eliminate the proteinaceous material
 should be prompted to increase the tubular flushing and eliminate the proteinaceous material.")
36
36 Complications of ACS Volkmann contracture : is the residual limb deformity that over wks to mos follows untreated ACS or ischemia from arterial injury. It may occur in the upper or lower extremities. Most commonly following humeral (supracondylar) or femoral shaft fxs. Pathogenesis : prolonged ischemia --------- myonecrosis ------ fibroblastic proliferation ------ contraction of the cicatrix ----myotendinous adhesion formation.
 or femoral shaft fxs. Pathogenesis : prolonged ischemia myonecrosis fibroblastic proliferation contraction of the cicatrix ----myotendinous adhesion formation..")
37
37 Complications of ACS Volkmann contracture : Rx ------ ** Non-surgical (physiotherapy & bracing of the involved joints) ** Surgical ( contracture release, nerve compression release, amputation or reconstruction with tissue transfers )
 ** Surgical ( contracture release, nerve compression release, amputation or reconstruction with tissue transfers )")
38
38 Complications of ACS Neurovascular injury Infection Amputation Rhabdomyolysis Myoglobinuric renal failure Death

39
39 Missed ACS The patient presents with various stages of muscle infarction. Difficulty occur when massive changes have become obvious. Fasciotomy will not help and make the situation worse because the muscles are necrotic and the risk of the infection is very high.

40
40 Prophylactic Fasciotomy Prophylactic fasciotomy of the forearm or leg should be performed if arterial ischemia has been present for >4 – 6 h Should be considered whenever an open tibia fx is debrided or a tibial osteotomy is performed

41
41 Chronic Compartment Syndrome Also known as exertional CS, recurrent CS and subacute CS Exercise – induced pain Occur mainly in the lower limb Typical patient is young (20-30s) athlete (long distance runner)or military recruits pushed past normal limits of functional tolerance
 athlete (long distance runner)or military recruits pushed past normal limits of functional tolerance")
42
42 Pathophysiology of CCS Not yet fully understood Probably occurs from increased muscle relaxation pressure during exercise, which causes decreased muscle blood flow, leading to ischemic pain and impaired muscle function

43
43 Physical Exam in CCS May reveal tenderness over the musculature involved in the compartment Bilateral involvement is common ( up to 82% ) Fascial hernias ( 39% in one of the studies )
 Fascial hernias ( 39% in one of the studies )")
44
44 Diagnosis of CCS Intracompartmental testing is the hallmark of diagnosis (as reported by Pedwotiz et al ) : 1) Pre-exercise resting pressure of 15 mm Hg or more. 2) Pressure of 30 mm Hg 1 minute after the exercise. 3) Pressure of 20 mm Hg or more 5 minutes after the exercise.
 Pressure of 30 mm Hg 1 minute after the exercise. 3) Pressure of 20 mm Hg or more 5 minutes after the exercise..")
45
45 DDx of CCS Periostitis Entrapment of the superficial peroneal nerve Tendinitis of the posterior tibial tendon Stress fracture of tibia Intermittent claudication

46
46 Work up of CCS Plain x-rays : will show 90% of stress fx Bone scan : diffuse uptake ……..periostitis localized uptake …… stress fx Tinel test : may be positive in superficial peroneal nerve entrapment NCS : could be helpful MRI : promising results reported

47
47 Treatment of CCS Non-operative : NSAIDs electrostimulation massage muscle relaxants ultrasound cessation or significant reduction of athletic activities

48
48 Treatment of CCS Operative treatment Single incision fasciotomy Double incision fasciotomy After surgery : Early ROM exercises are encouraged. WBAT on crutches is allowed on POD#1. Light jogging is allowed at 2-3 weeks if no swelling or tenderness

49
49 OITE A 30-year-old soccer player has pain and swelling 4 hours after being kicked in the anterior compartment of the leg. Which of the following physical findings best indicates increased compartment pressure ? 1- Anterior compartment tenderness 2- Pain with active ankle dorsiflexion 3- Pain with passive flexion of the toes 4- Pain with passive extension of the toes 5- Decreased sensation on the dorsum of the foot

50
50 OITE A 30-year-old man who sustained an isolated comminuted closed tibial shaft fracture after being struck by a car reports severe pain in his leg. Examination reveals the smell of alcohol on his breath. The patient has a 1 + pulse, but he will not cooperate with the neurologic examination. Management should include : 1- A long leg cast 2- An external fixator 3- An emergent angiogram 4- Measurement of compartment pressures 5- Administration of an analgesic and reexamination

51
Questions ??

Similar presentations



>")



 measure of P perfusion.>")











