Download presentation
Presentation is loading. Please wait.

1
WOUND HEALING Dr. Nahel Sorour Prof. of ENT Ain-Shams University

2
Epidermis Dermis Consists of 5 layers Outer st. sq epith.
Varies in thickness. No blood vessels or nerves endings Repair occurs via the basal germinal cell layer. Dermis Contains: bl. Vessels – sensory nerve endings – hair follicles - sweat & sebaceous glands and ducts – Arrectores pilorum. Bleeds when cut. Contains collagen bundles give tensile strength and elastic recoil. Contains gel matrix.

3
The Wound Definition Interruption of continuity of tissue resulting from a certain injury especially external physical trauma

4
Causes of tissue loss and destruction
Traumatic: accidental surgical Physical, chemical, microbial inflammation sever necrosis. Ischemia infarction. Body reaction: hypersensitivity to F.B.

5
Types of traumatic wounds
ACCORDING TO SKIN LOSS Closed wound: skin surface intact Without loss of skin Abrasions: partial division of superficial layer Contusion: Diffuse extravasation of blood and exudate ecchymotic. Hematoma: Localized collection in fascial planes – ve signs of inflammation. Opened wound: skin surface interrupted or loss of skin. Incised Stab and punctured wound Lacerated Crushed and gun shots.

7
According to contamination
Clean Contaminated According to the age of the wound Early (within 6 hours). Late ( 6-24h). delayed (after 24 h).
. Late ( 6-24h). delayed (after 24 h).")
8
WOUND HEALING Natural spontaneous response for restoration of tissue continuity after injury Healing is the interaction of a complex cascade of cellular events that generates Reconstitution and Resurfacing, Restoration of the tensile strength of injured skin. Sometimes, tissue has been disrupted so severely that it cannot heal naturally.

9
Phases of wound healing:
Inflammation (biochemical activation) overlapping [II] Proliferation (granulation& cellular activation) [III] Remodeling (maturation &differentiation of scare tissue)
 overlapping. [II] Proliferation. (granulation& cellular activation) [III] Remodeling. (maturation &differentiation of. scare tissue)")
10
Summary Inflammatory phase: Proliferative phase
A clot forms stop bleeding Vasodilatation of WBCs cells of inflammation defending and debridment of injured tissue. Proliferative phase Epithelization, Fibroplasia (fibroblasts and collagen), and Angiogenesis occur during the; additionally, Granulation tissue forms and The wound begins to contract. Remodeling (maturation) phase Collagen forms tight cross-links to other collagen and with protein molecules, Increasing the tensile strength of the scar.
, and. Angiogenesis occur during the; additionally, Granulation tissue forms and. The wound begins to contract. Remodeling (maturation) phase. Collagen forms tight cross-links to other collagen and with protein molecules, Increasing the tensile strength of the scar.")
11
[I] Inflammation (Biochemical -cellular activation) Period: 1-4 days
Aim: translation of mechanical injury into biochemical signals. This starts by: Changes the charge on the surface of collagen molecule. Platelets aggregation and extravasated plasma contact with the extravascular tissue proteins leads to activation of Hageman's factors (factor XII) and platelets.
![[I] Inflammation (Biochemical -cellular activation) Period: 1-4 days](http://slideplayer.com/slide/4413603/14/images/11/%5BI%5D+Inflammation+%28Biochemical+-cellular+activation%29+Period%3A+1-4+days.jpg "Aim: translation of mechanical injury into biochemical signals. This starts by: Changes the charge on the surface of collagen molecule. Platelets aggregation and extravasated plasma contact with the extravascular tissue proteins leads to activation of Hageman s factors (factor XII) and platelets.")
12
1ry vascular reaction: Activation of clotting factors cascade. Platelet aggregation Clot formation (The scab) which temporarily closes the wound consists mainly of fibrin mesh trapped other blood cells hemostasis. Temporary constricting of small blood vessels (few minutes) temporary blanching.
 which temporarily closes the wound consists mainly of fibrin mesh trapped other blood cells hemostasis. Temporary constricting of small blood vessels (few minutes) temporary blanching.")
13
Platelets: accumulate release alpha granules containing:
Activation of complement system chemotaxis degranulation of mast cells and cytolysis. Platelets: accumulate release alpha granules containing: vasoactive agents chemotactic factors growth factors. Alpha granules (growth factors) initiator proliferative phase by activating the local mesenchymal and epidermal cells.
 initiator proliferative phase by activating the local mesenchymal and epidermal cells.")
14
Types of growth factors
Mitogenic chemoattraction fibroblasts. PDGF Platelets derived growth factor chemoattraction Capillary endothelial cells. PDAF Platelets derived angiogenesis factor migration mitosis of epidermal cells epithelization PDEGF Platelets derived epidermal growth factor Chemoattraction for monocytes inhibit endothelial cell mitosis stimulate collagen synthesis by fibroblasts. TGF-B Transforming growth factor beta chemoattractant for neutrophil PF-4 Platelets factor 4

15
(signs of inflammation)
Vasodilatation (more persistent) Increase capillary engorgement ,Increase the capillary permeability, and blood flow under effect of histamine and bradykinin, serotonin, prostaglandins from platelets and mast cells flow of the necessary inflammatory cells and factors that fight infection and deriding the wound. This period is the event responsible for the erythema, edema, and heat observed after tissue injury Alterations in pH (secondary to tissue and bacterial degradation), The increase fluid tension in the area swelling press of the nerve endings, and tissue hypoxemia at the injury site contribute to the sensation of wound pain
 Increase capillary engorgement ,Increase the capillary permeability, and blood flow under effect of histamine and bradykinin, serotonin, prostaglandins from platelets and mast cells flow of the necessary inflammatory cells and factors that fight infection and deriding the wound. This period is the event responsible for the erythema, edema, and heat observed after tissue injury. Alterations in pH (secondary to tissue and bacterial degradation), The increase fluid tension in the area swelling press of the nerve endings, and tissue hypoxemia at the injury site contribute to the sensation of wound pain.")
16
Defending [migration of inflammatory cells & Chemoattraction to WBCs]
: PNL & Lymphocytes invade the wound and fibrin network within 3 hours defending and lysis with their lysosomes. release inflammatory mediators and bactericidal oxygen-free radicals. Lymphocytes also play a role in cellular immunity and antibody production. O2 is essential for the optimistic results of this defending process.
![Defending [migration of inflammatory cells & Chemoattraction to WBCs]](http://slideplayer.com/slide/4413603/14/images/16/Defending+%5Bmigration+of+inflammatory+cells+%26+Chemoattraction+to+WBCs%5D.jpg ": PNL & Lymphocytes invade the wound and fibrin network within 3 hours defending and lysis with their lysosomes. release inflammatory mediators and bactericidal oxygen-free radicals. Lymphocytes also play a role in cellular immunity and antibody production. O2 is essential for the optimistic results of this defending process.")
17
DEBRIDMENT Macrophages are essential for wound healing.
Macrophages (monocytes) enter the wound from the 2nd after wounding and present until the reparative process is complete. Along time macrophages continue phagocytose & cleaning the wound site of bacteria, debris, F.B and necrotic matter. producing the activation growth and chemotactic factors similar to those of platelets (complete the function of platelets)…...
 enter the wound from the 2nd after wounding and present until the reparative process is complete. Along time macrophages continue. phagocytose & cleaning the wound site of bacteria, debris, F.B and necrotic matter. producing the activation growth and chemotactic factors similar to those of platelets (complete the function of platelets)…...")
18
[II] Proliferation (granulation & cellular activation) starts after 3-5 days takes 5-20 days
INCLUDES: Granulation tissue formation Epithelization Contraction
![[II] Proliferation (granulation & cellular activation) starts after 3-5 days takes 5-20 days](http://slideplayer.com/slide/4413603/14/images/18/%5BII%5D+Proliferation+%28granulation+%26+cellular+activation%29+starts+after+3-5+days+takes+5-20+days.jpg "INCLUDES: Granulation tissue formation. Epithelization. Contraction.")
19
granulation tissue Granulation tissue formation occurs 3-5 days following injury Includes: Inflammatory cells, Fibroblasts and collagen, ground substance and Vascular and lymphatic proliferation

20
fibroblast The fibroblast is a critical component of granulation tissue. Fibroplasia begins from surrounding mesenchymal cells 3-5 days after injury and may last as long as 14 days. Fibroblasts migrate and proliferate in response to platelets growth factors. Fibroblasts are responsible for the production of collagen, elastin, ground substance

21
collagen synthesis the collagen fibers which is essential for:
bridging the wound gap supporting the growing vessels and wound strength. Fibroblasts Collagen III held together by weak electrostatic forces and is soluble in weak salt solution. It is laid down irregularly and haphazardly then polymerization occurs by cross linked to the collagen molecules Thick strong less soluble collagen [I] become more regular and perpendicular on the plane of wound. The process of collagen synthesis : Starts on the 3rd day The peak reaches by the 5-7 days It may extend to 6 m to 1 year.

22
This active metabolic process depends mainly on:
Vitamins: B, ascorbic acid O2 amino acids Elements: zinc, iron, copper Collagen formation decreased by: decrease of vit C. steroids (high dose). Protein starvation.
. Protein starvation.")
23
Angiogenesis (Vascular and lymphatic proliferation):
Ground substance Produced by fibroblasts (water – electrolytes – mucopolysaccharides (proteoglycans) – fibronectins – glycoproteins). Angiogenesis (Vascular and lymphatic proliferation): The macrophage growth factors stimulates angiogenesis New capillaries bud from endothelial cells in capillary near the wound edges appear proliferation a new network of capillaries is formed inside the granulation tissues red granulations.
 – fibronectins – glycoproteins). Angiogenesis (Vascular and lymphatic proliferation): The macrophage growth factors stimulates angiogenesis. New capillaries bud from endothelial cells in capillary near the wound edges appear proliferation a new network of capillaries is formed inside the granulation tissues red granulations.")
24
Stats within hours by mitosis of the basal cell layer.
Epithelization Stats within hours by mitosis of the basal cell layer. The epidermal cells advanced from the edges and creep across the wound surface in a favorable plane dissecting the wound between the living and dead tissue. Migration stops when it meets the opposite advanced epithelium. The new epithelium is thin non-pigmented. Incisional wounds are epithelized within hours after injury (distance of less than 1 mm). This epithelial layer provides a seal between the underlying wound and the environment.
. This epithelial layer provides a seal between the underlying wound and the environment.")
25
In open wounds: if the wound is moist well oxygenated with viable moist surface and epithelization rapid (few days) and cell migrate over the surface of the wound. However, The process is more slower if the wound dry. The cells burring under the eschar and slowly separating the mobile from the immobile tissue. This explain why the epithelial is more rapid in intact blister than after the blister has been debride and the base of the blister allowed to dry.

26
In sutured wounds: epithelium may invade the lining of the suture tracks. It usually degenerate with early removal of sutures. However, prolonged sutures ugly punctuate scars. This may be avoided by adhesions taps better cosmoses.

27
Wound contraction fibroblasts in the peripheral granulations maturation myofibroblasts centripetal movement of wound edges contraction decrease wound size facilitates closure of a defect. Lag period 2-3 days (with collagen synthesis) with Maximum rapid contraction 3-14 days (The maximal rate of contraction is 0.75 mm/d) It specially occurs at the back of the neck, trunk and face where the skin is loose Contraction must be distinguished from contracture. Contraction is decreased by : x-ray steroids grafting with dermis Burns If prevented slow healing – large fibrous tissue - ugly scar cicatrisation & complications.
 with Maximum rapid contraction 3-14 days (The maximal rate of contraction is 0.75 mm/d) It specially occurs at the back of the neck, trunk and face where the skin is loose. Contraction must be distinguished from contracture. Contraction is decreased by : x-ray. steroids. grafting with dermis. Burns. If prevented. slow healing – large fibrous tissue - ugly scar. cicatrisation & complications.")
28
Devascularization Collagen remodeling Cicatrisation
[III] Phase of remodeling (maturation &differentiation of scare tissue) It occurs after 20 days and continue for many months and years or indefinitely. Devascularization Collagen remodeling Cicatrisation
 It occurs after 20 days and continue for many months and years or indefinitely. Devascularization. Collagen remodeling. Cicatrisation.")
29
Devascularization: The granulation tissue is gradually replaced by a scare tissue which is relatively acellular and avascular tissue. pale scare tissue. The extracellular tissue change its contents. Water is resorbed from the scar.

30
Collagen remodeling Collagen remodeling during the maturation phase depends on continued collagen synthesis in the presence of collagen destruction under effect of collagenase. The ratio of the collagen type [I] increase. New collagen is formed in more orderly fashion along the lines of tension in the scare. Facilitating collagen fibers cross-linking and ultimately decreasing scar thickness and increasing wound bursting strength.

31
Finally 4-12 w a pale red thick strong scare tend to contract is formed. Excessive contracture of the scare tissue cicatrisation. [contracture] a pathologic process of excessive fibrosis that limits motion of the underlying tissues and is typically caused by the application of excessive stress to the wound. 12-40 w soft white scare tend to relax. Hyalinization, calcification and even ossification may sometimes occur.

32
Complications of wound healing
Bleeding - shock - anemia. Injury of Imp. structures. Infection: Dehiscence (bursting wound). Implantation or epidermoid cyst Keloid formation Pigmentation tattooing Painful scare local or reformed neuroma. Cicatrization : burns deformity stricture and stenosis in tubes. Neoplasia: sq cell ca. on scare tissue. F.b. retained Maggots.
. Implantation or epidermoid cyst. Keloid formation. Pigmentation tattooing. Painful scare local or reformed neuroma. Cicatrization : burns deformity stricture and stenosis in tubes. Neoplasia: sq cell ca. on scare tissue. F.b. retained. Maggots.")
33
Tensile strength: The work done (force) in breaking a wound per unit area. The bursting strength of a wound is the force required to break a wound regardless of its dimension. Peak tensile strength of a wound occurs approximately 60 days after injury. A healed wound only reaches approximately 80% of the tensile strength of unwounded skin

34
the increase of cross linkage between the fibers increase its quality which is reflected in continuing increase in tensile strength. Factors affecting tensile strength: Factors affecting collagen synthesis specially vit C decrease. Direction of the w Parallel to the lines of Langer faster the healing and increase the tensile strength In the direction of the pull of the underlying muscle line of creases line scare least visible. no diff detectable between the wound that are taped and those that are sutured .

35
Dehiscence (bursting wound).
PF: Infection. Weak scare due to continuous strain (coughing vomiting) or stretch Decrease the bursting strength. Rapid absorbed catgut. Poor surgical technique. General conditions poor wound healing Decrease nutrition (Proteins) and vitamins (vit c)
 or stretch Decrease the bursting strength. Rapid absorbed catgut. Poor surgical technique. General conditions poor wound healing. Decrease nutrition (Proteins) and vitamins (vit c)")
36
Keloid formation & hypertrophic scars
Unknown etiology P.F. Repeated trauma Irritation of FB, hair, keratin TB patients - burns Age: In young, thin skin 1st year of life. And very old Sex: females Race: black Common Site: Neck over the sternum. Wounds that cross skin tension lines or wounds that are located on the ear lobes or presternal and deltoid areas.

37
Difference: Keloid grow beyond the wound borders
It does not tend to resolve spontaneously. Hypertrophic scars stay within the limit of the original wound and do tend to regress spontaneously. It can form as late as a year after injury whereas Hypertrophic scars are generally seen soon after tissue injury, if the active scare continue more than 6 month it is considered true keloid which may extend up to 5-10 years.

38
Histologically: Keloid also contain a greater amount of type III collagen than a mature scar, which suggests a failure in scar maturation. The collagen is loose disorganized wavy pattern of irregularly shaped fibers with a lower content of collagen cross-links compared to normal skin. keloid and hypertrophic scars have rich blood supply, high mesenchymal density, and a thick epidermal layer.

39
TTT: The recurrence rate of these abnormal scars is high.
Conservative management includes: Intralesional injection of triamcinolone. pressure, Laser, and radiotherapy. Excision & grafting :only if no response to conservative management.

40
Maggots

41
Factors affecting repair
General Local Age Smoking. Nutritional status Fluids electrolyte imbalance Drugs: Anticoagulants Cytotoxic drugs Hormones Temperature Chronic diseases : Anemia Uremia Jaundice Diabetes Intraoperative surgical factors O2 tension Inadequate bl. supply Wound tension Infection Extent of tissue loss, sloughs & F.B Age of wound Multiple dressing & Movement Drying Irradiation & Ultraviolet

42
Intraoperative surgical factors
Length & Direction The best cosmetic results may be achieved when incisions are made parallel to the direction of the tissue fibers. Tissue handling, Hemostasis, Maintaining moisture Materials of closure.

43
DISSECTION TECHNIQUE a clean regular incision should be made through the skin with one stroke of evenly applied pressure on the scalpel. Sharp dissection. Preserve the integrity of the underlying important structures

44
TISSUE HANDLING Minimize tissue trauma Handle all tissues very gently
Retractors should avoid excessive pressure, since tension can cause serious complications: impaired blood and lymph flow microbial colonization.

45
HEMOSTASIS Achieving complete hemostasis before wound closure to avoid postoperative hematomas & seromas Prevent the direct apposition of tissue. Ideal medium for serious infection. When clamping or ligating avoid excessive tissue damage. Mass ligation that involves large areas of tissue may produce necrosis.

46
MAINTAINING MOISTURE IN TISSUES
Periodically irrigate the wound with warm saline solution. or cover exposed surfaces with saline-moistened sponges to prevent tissues from drying out.

47
CHOICE OF CLOSURE MATERIALS
Cellular response to closure materials Closing tension Postoperative distraction forces Immobilization Elimination of dead space in the wound

48
REMOVAL OF NECROTIC TISSUE & FB
Presence of sloughs & F.B. : decrease the O2 tension high risk of bacterial infection Adequate debridement of all devitalized tissue and removal of inflicted foreign materials are essential to healing

49
O2 tension and blood supply
affect the rate of healing. It is essential for phagocytosis and collagen synthesis. Decrease O2 tension increase anaerobic infection. Blood supply: Face - other areas are slow. Ischemia due to pressure Venous engorgement Chronic inflammation with endarteritis obliterans, old age - atherosclerosis, inadequate hemostasis, Diabetes, Tension & edema x-ray irradiation. Hyperbaric O2

50
Infection Delayed healing or stop it G+ve staphylococci most common.
Infection compete with fibroblasts on nutrients & O2 decrease collagen Also collagenase enzyme activity destruction of collagen. Increase necrotic tissue (sloughs). Inflamed unhealthy granulation. Healing by 2ry intension. Increase fibrous tissue with Ugly scare. G+ve staphylococci most common. G-ve E-coli – klebsiella – Proteous – pseudomonas Anaerobic infection (Tetanus - gas gangrene) in crushed, damaged, ischemic lethal effect by endogenous and exogenous toxins.. Decrease O2 tension increase anaerobic infection.
. Inflamed unhealthy granulation. Healing by 2ry intension. Increase fibrous tissue with Ugly scare. G+ve staphylococci most common. G-ve E-coli – klebsiella – Proteous – pseudomonas. Anaerobic infection (Tetanus - gas gangrene) in crushed, damaged, ischemic lethal effect by endogenous and exogenous toxins.. Decrease O2 tension increase anaerobic infection.")
51
Infection increased by:
Prevent infection by Bad General conditions diabetes Steroids Bad surgical handling of tissue. Open drainage Prolonged sutures Prosthesis, FB, crushed wounds and sloughs. Bad hygiene & sterlization Carriers in staff or pt. Control General conditions Avoid steroids Good surgical handling Antibiotics prophylaxis Preoperative sterilization.

52
General Factors Age: Nutrition:
Fetal wound healing Wounds occurring in fetuses of early gestational age can heal without any scar formation. young old as the atherosclerosis and protein turn over slow healing. Nutrition: Proteins. Vitamins: Vit c: essential for collagen synthesis > decrease collagen and ground substances. Vit A: for epithelization. Vit B affecting collagen type III – antibody production Vit K formation of clotting factors. Minerals: Zinc: zinc sulphate Ca, cu. manganese.

53
Variants of wound healing
1ry intention 2ry intension 3ry intension

54
HEALING BY PRIMARY INTENTION
It occurs in Coapted or sutured clean wound No tissue loss No infection good blood supply Inflammatory (preparative), Proliferative, Remodeling End result: Rapid healing and epithelization with Less granulations, Less fibrosis and minimal better cosmetic scare. It is the best type of healing.
, Proliferative, Remodeling. End result: Rapid healing and epithelization with Less granulations, Less fibrosis and minimal better cosmetic scare. It is the best type of healing.")
55
HEALING BY SECONDARY INTENTION
caused by infection, excessive trauma, tissue loss, or imprecise approximation of tissue. Examples: Leg ulcer Pressure sore Infected wounds

56
The healing starts from the base upward as well from the margins.
The phases of healing are exaggerated and prolonged Granulation tissue may require treatment if it protrudes above the surface of the wound, preventing epithelialization. Contains myofibroblasts contraction. epidermis then thickened, no appendages or rete ridges, less adherent. More collagen tissue give scare with more scare tissue.

57
This occurs in complete thick skin loss.
However in partial thickness skin loss (Thiersch graft) there are rapid cover with epithelium from the edges and the remnants of the hair follicles. The granulations are minimal between the islands of the growing epithelium.
 there are rapid cover with epithelium from the edges and the remnants of the hair follicles. The granulations are minimal between the islands of the growing epithelium.")
58
Tertiary intention It occurs in when wound is re-sutured after braking down, controlling of infection, and surgical debridement We opposing two opposite granulating surfaces together aiming for decrease the fibrosis – scare tissue and promoting healing However, Resulting in deeper ugly scare

59
Examination of the wound
History: Examine General conditions: Local: Type of wound: Structures of the wound Surface – edges – infection- Discharge- hematoma – edema – fb. Examine deep structures: muscles, tendons, nerves and major Bl v LN examination. Test movement and sensations, exam. for fractures. Investigations: X-ray in two plains to exclude fb. Swab: culture in dirty wounds. General blood investigations

60
Structure of the wound Necrotic eschar: dry hard black dead tissue needs depriment. Sloughs: yellow, sticky tissue undergoing autolysis or grey dead CT. Granulation tissue: wound looks red, velvety and moist. there may be also evidence of yellow fibrinous membrane which should not be confused with infection.

61
Buds of epithelization: pink appearance of new skin cover extending from the margins with perhaps some islands of new epithelium contained in the main area of the wound bed depending on the depth of the wound.

62
Infection: signs of infection:

64
Exudate: indicate presence amount and ch. ch. E. g
Exudate: indicate presence amount and ch.ch. E.g. color, small and consistency. Odor: indicate the presence of odor e.g. sweet, bitter, putrid. Pain: analysis of pain Wound margin: indicate if the surrounding skin is macerated or dry. Describe epithelization around wound edges. Any undermining.

65
Care of the wound: Local General:
Antishock measurement Antitetanic serum Antigasgangren Antibiotics.: systemic - local Medical control of general factors affecting healing: Adequate proteins: kg/wt Adequate calories: male: 2500 Kcals female: 1900Kcals Vit C: mg/day VitA: micrograms. Zinc: millimols Local Assessment Surgical management Control infection wound dressing. Adjuvant therapy.

66
Surgical management Traditional cornerstones concepts of wound management Cleaning and irrigation with saline Sterilization, dirty wound: cleaned with antiseptics solution cetavlon. Debridement. dead tissue and foreign bodies must be removed. Devitalized skin should be excised. Damaged ms should be excised until ms bleeds and contract when cut. Management of the wound fluid: prevent tension and if needed extended the wound in longitudinal direction. Deep fascia must be freely excised in presence of tension or hematoma beneath. Sustained an optimum temperature for healing. Tissue is better to be held in apposition

67
The Exudate The exudate of chronic wounds has been found to inhibit wound healing. Removing or controlling exudate can lead to improved wound healing by: Compression Negative pressure devices and vacuum-assisted devices. Drains are important in preventing exudate from accumulating in wound site. A fine balance should be maintained between excessive exudate and drying of the wound.

68
METHODS OF CLOSURE OF WOUND
until the the wound can withstand stress without mechanical support. Types Sutures: 1ry delayed 1ry 2ry. Clips Staples Tapes [skin closure strips] Topical Adhesive materials and Tissue glues Tissue grafts Flaps Skin closure is better accomplished by microporous tape. It lowering infection and achieve great strength with less dehiscence.

69
Polyglycolin and polygalactin:
Wires: most inert maintain its tensile strength for long time. Painful difficult to tie. Plastic sutures: Inert Tie is usually loose and become untied spontaneously. Silk: Animal proteins inert absorbable over long period of time. loose its tensile strength & Unsuitable for suturing prosthesis . its irregularity and multifiber constituent occasionally haven bacteria form small abscess. Catgut: now it is manufactured from bovine collagen which cause less inflammatory reaction. And more constant in their absorption. Polyglycolin and polygalactin: it is hydrolyzed by extracellular enzymes. It lose 1/2 its strength by 21/2 weeks

70
Applications [1] Closed wounds
Contusions: skin sterilization. pressure bandages Hematoma: Small pressure. Large aspiration under sterile techniques. Organized collection incise and evacuate then compression. Infected drain.
![Applications [1] Closed wounds](http://slideplayer.com/slide/4413603/14/images/70/Applications+%5B1%5D+Closed+wounds.jpg "Contusions: skin sterilization. pressure bandages. Hematoma: Small pressure. Large aspiration under sterile techniques. Organized collection incise and evacuate then compression. Infected drain.")
71
[2] Open wounds Early Clean: incised (6h) clean – close
lacerated (6h) excision – clean – close wit 1ry suture including the underlying muscles. If there is skin loss Skin graft or skin flaps. Taped wounds are protected from infection than sutured wounds. Suture wound can be infected from outside media particularly within the first 3-4 days. Therefore, wound is better to be protected with dressing for at least 4 days with repeated cleaning and change of dressing.
![[2] Open wounds Early Clean: incised (6h) clean – close](http://slideplayer.com/slide/4413603/14/images/71/%5B2%5D+Open+wounds+Early+Clean%3A+incised+%286h%29+%EF%83%A0+clean+%E2%80%93+close.jpg "lacerated (6h) excision – clean – close wit 1ry suture including the underlying muscles. If there is skin loss Skin graft or skin flaps. Taped wounds are protected from infection than sutured wounds. Suture wound can be infected from outside media particularly within the first 3-4 days. Therefore, wound is better to be protected with dressing for at least 4 days with repeated cleaning and change of dressing.")
72
Potentially contaminated wounds Late (6-24h) [ DELAYED PRIMARY CLOSURE]
potentially infected traumatic wounds with extensive tissue loss and a high risk of infection. The surgeon usually treats these injuries by Debridement. leaves the wound open, Dressing changed twice a day. within 3-5 days If infection is controlled with the appearance of red granulation tissue Wound approximation using delayed 1ry suturing. It may be previously placed but untied, adhesive or strips, staples. If infection occurs, the wound is allowed to heal by secondary intention.
![Potentially contaminated wounds Late (6-24h) [ DELAYED PRIMARY CLOSURE]](http://slideplayer.com/slide/4413603/14/images/72/Potentially+contaminated+wounds+Late+%286-24h%29+%5B+DELAYED+PRIMARY+CLOSURE%5D.jpg "potentially infected traumatic wounds with extensive tissue loss and a high risk of infection. The surgeon usually treats these injuries by. Debridement. leaves the wound open, Dressing changed twice a day. within 3-5 days If infection is controlled with the appearance of red granulation tissue Wound approximation using delayed 1ry suturing. It may be previously placed but untied, adhesive or strips, staples. If infection occurs, the wound is allowed to heal by secondary intention.")
73
Delayed Contaminated lacerated or crushed wounds ( after 24 hours).
Debridement . open pockets of infection and collections but do not open new plains. leave to granulate and to heal by 2ry intention, however, remove excessive elevated granulations. Controlling infection with dressing and antibiotics. If the infection is controlled early 2ry sutures

74
Summary Delayed (more than 6H) Early (6H) wait infection No infection
TTT 2ry sutures may be done 1ry sutures Immediate 2ry intension 3ry intension 1ry intention

75
Wound dressing Aiming to decrease further physical trauma and
to prevent infection, and to create optimum environment for wound healing. Dressings: occlusive and semiocclusive Tape Bandages Binders

76
Two type of wound dressing
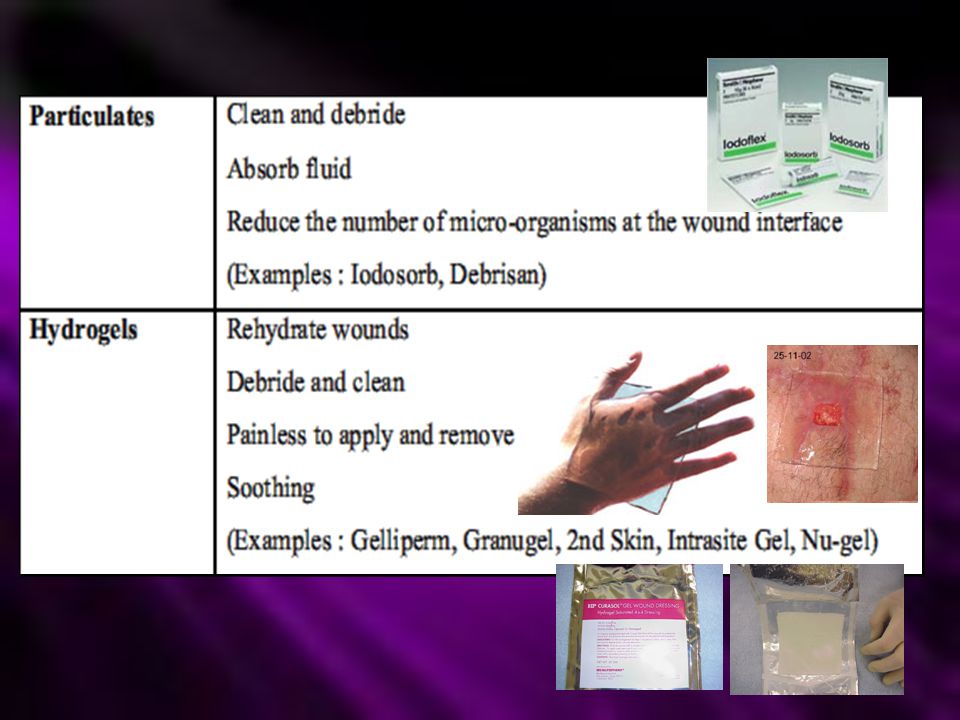
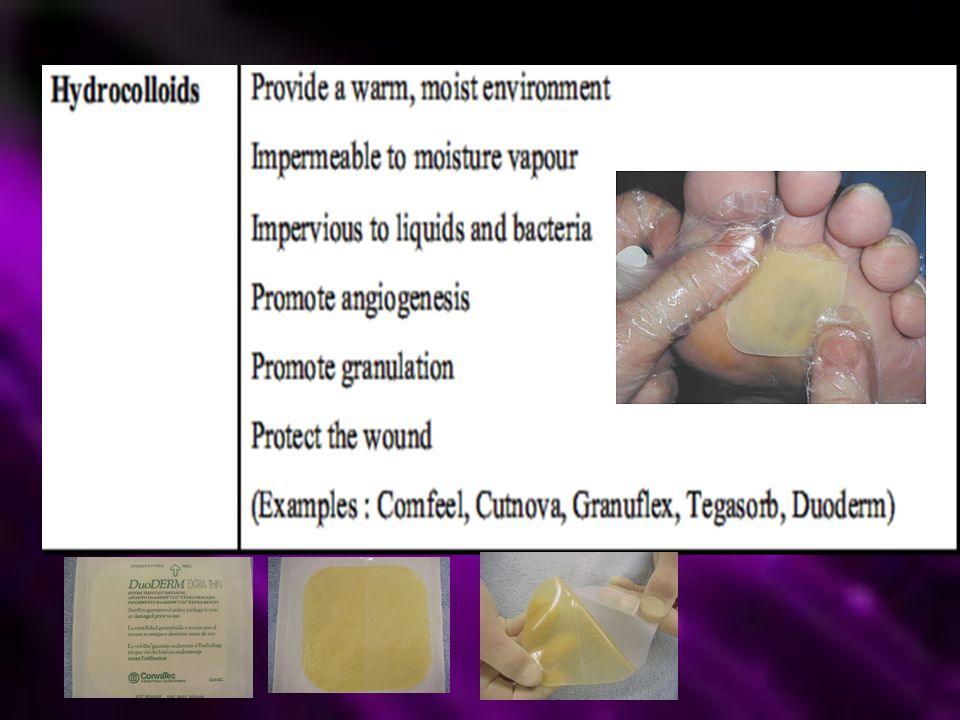
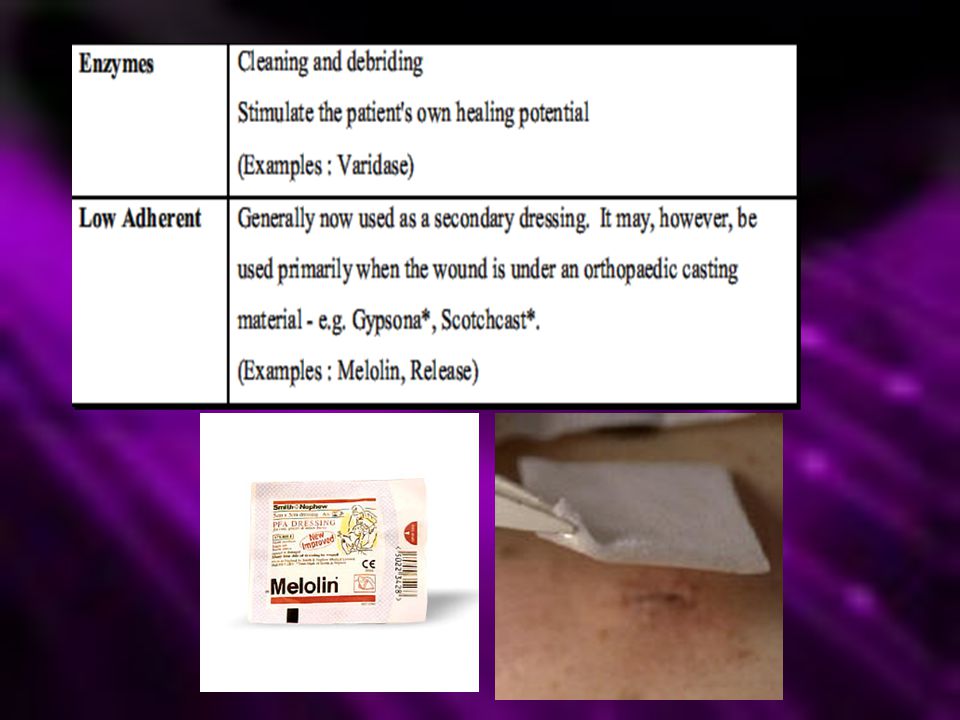
Moist wound dressing with Occlusive or semi occlusive and hydrocolloid dressings : Increase healing Rapid re-epithelization. Angiogenesis. promote dermal matrix synthesis and Dermal repair. improve the patient’s comfort. Once epithelization occurs no need for covering as the epithelium do protection.[ a natural semiocclussive dressing] Dry wound dressing The hard eschar act as a barrier against the epidermal creeping. If the surface layers of the wound dry out the epithelial cells will move downward to reach a moist environment delaying healing The dressing usually adhere with the wound surface. its removal leads to reinjury. This may delay healing and cause more ugly scare.

77
Dressing materials The ideal dressing should be:
Remove excess exudate from the wound maintain a high humidity at the wound/dressing interface. Sustain an optimum temperature for healing. Be impermeable to microorganisms Be free from contaminants. Not shed fibers into wound. Easily removed without wound trauma. Preserve an optimum pH value.

78
Opsite: Tegaderm:

79
Tielle Allevyn

84
Transparent film membranes Transparent film membranes
Foam Hydrocolloid Hydrocolloid Transparent film membranes Transparent film membranes Hydrogel Hydrogel

85
Adjuvant therapy Electrotherapy
Ultrasound: increase the blood flow – good bio-effect on tissue repair and protein synthesis Hyperbaric O2 Laser and Light therapy: doubtful.

86
Wound assessment & follow up
Invasive Biopsy: no of cell type Biochemical analysis: as collagen Tensile strength estimation: Angiography: monitoring angiogenesis. Noninvasive Provisional size of the wound: length, width and depth Digitalized transparency tracing of the edges of the wound. Photographic and video recording: doubtful Depth gouges: wound volume molds: hydrocolloid gel Thermal imaging: detect infrared irradiation from the wound. High frequency ultrasound scanning: more for assessing the quality and quantity of healing.

87
Thank you

Similar presentations





 Closed wound: Skin is intact (not opened) include crushing injury and contusions. Wounds A) Skin involvement: 1) Open wound: when the whole thickness.>")



 Immediate threat: –Dehydration and electrolyte.>")












