Download presentation
Presentation is loading. Please wait.

1
Gina Throneberry, RN, MBA, CASC, CNOR Director of Education and Clinical Affairs Ambulatory Surgery Center Association (ASCA)
")
2
Participants will: Identify quality reporting by Centers for Medicare & Medicaid Services (CMS) for Ambulatory Surgery Centers (ASCs) Understand the history of quality measure development Learn to collect and report the data for the required quality measures
 for Ambulatory Surgery Centers (ASCs) Understand the history of quality measure development Learn to collect and report the data for the required quality measures")
3
Centers for Medicare & Medicaid Services (CMS) / State Life Safety Code (LSC) Occupational Safety and Health Administration (OSHA) Food and Drug Administration (FDA) Environmental Protection Agency (EPA) Drug Enforcement Agency (DEA) Federal Aviation Administration (FAA)
 / State Life Safety Code (LSC) Occupational Safety and Health Administration (OSHA) Food and Drug Administration (FDA) Environmental Protection Agency (EPA) Drug Enforcement Agency (DEA) Federal Aviation Administration (FAA)")
4
American Recovery and Reinvestment Act of 2009 Stimulus money provided the down payment for a nationwide effort to reduce health care associated infections in stand- alone or same-day surgical centers. Interpretive Guidelines for the Conditions for Coverage provide guidance on the meaning of the rules and further advice on how ASCs should comply. State Operations Manual http://www.cms.gov/Regulations-and- Guidance/Guidance/Manuals/Downloads/som107ap_l_ambulatory.pdf Infection Control Surveyor Worksheet http://www.cms.gov/Regulations-and- Guidance/Guidance/Manuals/downloads/som107_exhibit_351.pdf

5
Medicare requires ASCs to comply with the 2000 edition of the Life Safety Code, updated and published by the National Fire Protection Association.

6
In April 2014, CMS announced the proposal to adopt the National Fire Protection Association’s (NFPA) 2012 editions of the Life Safety Code (LSC) and the Health Care Facilities Code (HCFC). ◦ The requirement is currently a 1-hour minimum separation between ASCs and other adjacent tenants/occupancies. This proposal would require a 2-hour separation in un-sprinkled buildings. ◦ More extensive alarms, and more elaborate medical air compressors and clinical vacuum on piped medical gas systems would be required which would cause needed upgrades to systems. ◦ For windowless anesthetizing locations: “The ASC must have a supply and exhaust system that (i) Automatically vents smoke and products of combustion, (ii) Prevents recirculation of smoke originating within the surgical suite, and (iii) Prevents the circulation of smoke entering the system intake. These requirements would impact the design, installation, and operation of the entire HVAC system for a facility.
 Automatically vents smoke and products of combustion, (ii) Prevents recirculation of smoke originating within the surgical suite, and (iii) Prevents the circulation of smoke entering the system intake. These requirements would impact the design, installation, and operation of the entire HVAC system for a facility..")
7
Occupational Exposure to Bloodborne Pathogens 29CFR 1910.1030 http://www.osha.gov/pls/oshaweb/owadisp.show_doc ument?p_table=standards&p_id=10051 OSHA has two different types of inspections: Enforcement inspections determined by OSHA (unannounced) Consultation services that are requested by the facility (scheduled) http://www.osha.gov/dcsp/smallbusiness/consult.htm http://www.osha.gov/dcsp/smallbusiness/consult.htm
 Consultation services that are requested by the facility (scheduled)")
8
These surveys focus on the ASC’s response to recalls. http://www.fda.gov/Safety/Recalls/default.htm http://www.fda.gov/Safety/MedWatch/default.htm

9
Resource Conservation and Recovery Act (RCRA) gives the EPA the authority to control hazardous waste from the “cradle to the grave”. This includes the generation, transportation, treatment, storage, and disposal of hazardous waste. Hazardous Pharmaceutical Waste under the RCRA: Contains a “P” (acutely hazardous) or “U” (toxic) listed waste as the sole ingredient; or Exhibits at least one “characteristic” of a hazardous waste It is recommended to involve the center’s consulting pharmacist to make certain the center is in compliance with federal and state regulations.
 or U (toxic) listed waste as the sole ingredient; or Exhibits at least one characteristic of a hazardous waste It is recommended to involve the center’s consulting pharmacist to make certain the center is in compliance with federal and state regulations..")
10
Questions and Answers regarding DEA 222 forms- http://www.deadiversion.usdoj.gov/faq/dea2 22.htm http://www.deadiversion.usdoj.gov/faq/dea2 22.htm

11
These surveys examine: the process of transporting radioactive materials training of ASC staff in handling radioactive materials the ASC’s policies on radioactive materials (process for shipping of materials, process for return of product, how to handle hazards, staff training, consultant physicist, etc.)
")
12
Rule Reference Proposed or Final Rule Federal Register (FR) Reference https://www.federalregister.gov Program Highlights CY 2015 OPPS/ASC Final1 new claims-based measure- “dry run” 2015 CY 2014 OPPS/ASC Final78 FR 75122Finalized 3 measures CY 2013 OPPS/ASC Final77 FR 68492No additional measures FY 2013 IPPS/LTCH PPS Final77 FR 53637Finalized requirements CY 2012 OPPS/ASC Final76 FR 74492Finalized 8 measures CY 2011 OPPS/ASC Final75 FR 72109Discussed/Not implemented CY 2010 OPPS/ASC Final74 FR 60656Discussed/Not implemented CY 2009 OPPS/ASC Final73 FR 68780Discussed/Not implemented CY 2008 OPPS/ASC Final72 FR 66875Discussed/Not implemented
 Reference Program Highlights CY 2015 OPPS/ASC Final1 new claims-based measure- dry run 2015 CY 2014 OPPS/ASC Final78 FR 75122Finalized 3 measures CY 2013 OPPS/ASC Final77 FR 68492No additional measures FY 2013 IPPS/LTCH PPS Final77 FR 53637Finalized requirements CY 2012 OPPS/ASC Final76 FR 74492Finalized 8 measures CY 2011 OPPS/ASC Final75 FR 72109Discussed/Not implemented CY 2010 OPPS/ASC Final74 FR 60656Discussed/Not implemented CY 2009 OPPS/ASC Final73 FR 68780Discussed/Not implemented CY 2008 OPPS/ASC Final72 FR 66875Discussed/Not implemented")
15
CMS ASC Quality Reporting Program Quality Measures Specifications Manual To date- 9 versions (April 2012-June 2014) Latest version- 4.0 (June 2014) Located @ www.qualitynet.org under ASC tabwww.qualitynet.org Included in this manual: Measure specifications Data collection and submission Quality Data Codes (QDCs)
 Latest version- 4.0 (June 2014) under ASC tabwww.qualitynet.org Included in this manual: Measure specifications Data collection and submission Quality Data Codes (QDCs)")
16
ASC-1: Patient Burn* ASC-2: Patient Fall* ASC-3: Wrong Site, Wrong Side, Wrong Patient, Wrong Procedure, Wrong Implant* ASC-4: Hospital Transfer/Admission* ASC-5: Prophylactic Intravenous (IV) Antibiotic Timing* * Data submission began in CY 2012
 Antibiotic Timing* * Data submission began in CY 2012")
17
Claims Based Reporting–Quality Data Codes (QDCs) Patient Burn Patient Burn Patient Fall Patient Fall Wrong Site, Side, Patient, Procedure, Implant Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal (www.qualitynet.org)www.qualitynet.org Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) (www.cdc.gov/nhsn/index.html)www.cdc.gov/nhsn/index.html Influenza Vaccination Coverage Among Health Care Personnel
 Patient Burn Patient Burn Patient Fall Patient Fall Wrong Site, Side, Patient, Procedure, Implant Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal ( Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) ( Influenza Vaccination Coverage Among Health Care Personnel")
19
Released August 2012 The final rule can be accessed at (https://s3.amazonaws.com/public- inspection.federalregister.gov/2012-19079.pdf)https://s3.amazonaws.com/public- inspection.federalregister.gov/2012-19079.pdf This is the vehicle for rulemaking on the specifics of the ASC quality reporting program; ASC information begins on page 1534; Section E. ◦ Participation in the ASC Quality Reporting Program; Page 1540 ◦ Limited details for public reporting of data; Page 1541 ◦ Data completeness and validation; Page 1548 ◦ Extraordinary circumstances; Page 1554 ◦ Reconsideration and appeals process; Page 1558

20
Once an ASC submits any quality measure data, the center would be considered participating The ASC will continue to be considered a participant, regardless of whether the ASC continues to submit quality measure data, until formally withdrawing from the program An ASC that wishes to withdraw from the ASC Quality Reporting (ASCQR) Program must fill out an online withdrawal form: Located on the QualityNet website www.qualitynet.orgwww.qualitynet.org Click on left hand side: how to participate then Click on left hand side: how to withdraw An ASC can withdraw at any time up to August 31 prior to the payment determination year An ASC that withdraws will incur a 2% reduction in its Annual Payment Update (APU) and any subsequent year the ASC is not participating
 Program must fill out an online withdrawal form: Located on the QualityNet website Click on left hand side: how to participate then Click on left hand side: how to withdraw An ASC can withdraw at any time up to August 31 prior to the payment determination year An ASC that withdraws will incur a 2% reduction in its Annual Payment Update (APU) and any subsequent year the ASC is not participating")
21
Process was established in the FY 2013 IPPS/LTCH PPS final rule (77 FR 53642 through 53643) CMS may grant a waiver or extension to ASCs for data submission requirements if it is determined that a systemic problem with a data collection system directly or indirectly affects the ability to enter data Needs to be submitted within 45 days of the extraordinary circumstance Form (Extraordinary Circumstances) is located on www.qualitynet.org; click on ASC tab; form is located on the left side of the page www.qualitynet.org In the future this process will be referred to as the Extraordinary Circumstances Extensions or Exemptions Process
 CMS may grant a waiver or extension to ASCs for data submission requirements if it is determined that a systemic problem with a data collection system directly or indirectly affects the ability to enter data Needs to be submitted within 45 days of the extraordinary circumstance Form (Extraordinary Circumstances) is located on click on ASC tab; form is located on the left side of the page In the future this process will be referred to as the Extraordinary Circumstances Extensions or Exemptions Process")
22
Process was established in the FY 2013 IPPS/LTCH PPS final rule (77 FR 53643 through 53644) Reconsideration request form must be submitted by March 17 of the affected payment year CMS intends to complete any reconsideration reviews and communicate results within 90 days following the deadline (March 17 of the affected payment year) Form (Annual Payment Update (APU) reconsideration) is located on www.qualitynet.org; click on ASC tab; form is located on the left side of the pagewww.qualitynet.org
 Reconsideration request form must be submitted by March 17 of the affected payment year CMS intends to complete any reconsideration reviews and communicate results within 90 days following the deadline (March 17 of the affected payment year) Form (Annual Payment Update (APU) reconsideration) is located on click on ASC tab; form is located on the left side of the pagewww.qualitynet.org")
23
ASC-1: Patient Burn ASC-2: Patient Fall ASC-3: Wrong Site, Wrong Side, Wrong Patient, Wrong Procedure, Wrong Implant ASC-4: Hospital Transfer/Admission ASC-5: Prophylactic Intravenous (IV) Antibiotic Timing ASC-6: Safe Surgery Checklist Use ASC-7: ASC Facility Volume Data on Selected ASC Surgical Procedures { Procedure Category Corresponding HCPCS Codes: Eye/Gastrointestinal/Genitourinary/Musculoskeletal/ Nervous/Respiratory/Skin/Multi-system}
 Antibiotic Timing ASC-6: Safe Surgery Checklist Use ASC-7: ASC Facility Volume Data on Selected ASC Surgical Procedures { Procedure Category Corresponding HCPCS Codes: Eye/Gastrointestinal/Genitourinary/Musculoskeletal/ Nervous/Respiratory/Skin/Multi-system}")
24
Safe Surgery Checklist Use Intent: Assess whether an ASC uses a safe surgery checklist May employ any checklist as long as it addresses effective communication and safe surgery practices in each of three peri-operative periods: the period prior to the administration of anesthesia, the period prior to skin incision, and the period of closure of incision and prior to the patient leaving the operating room Applies to all ASCs

25
Safe Surgery Checklist Use Data collection: January 1-December 31, 2014 For 2014 and beyond, the checklist should be utilized for the ENTIRE year for an answer of "Yes". Report “Yes” or “No” on the Quality Net web site (www.qualitynet.org) between January 1 through August 15, 2015.www.qualitynet.org

26
ASC Volume of Selected Procedures Intent: Measure all patient volume of procedures performed in one of eight categories Eye Gastrointestinal Genitourinary Musculoskeletal Nervous System Respiratory Skin Multi-system Measurement from January 1, 2014 through December 31, 2014 Report volumes for entire 2014 calendar year on the QualityNet web site (www.qualitynet.org) between January 1 thru August 15, 2015www.qualitynet.org

27
Organ SystemCMS Procedure CategorySurgical Procedure Codes EyeOrgan transplant (eye)65756, V2785 Laser procedure of eye65855, 66761, 66821 Glaucoma procedures66170, 66180, 66711 Cataract procedures66982, 66984 Injection of eye67028, J2778, J3300, J3396 Retina, macular and posterior segment procedures67041, 67042, 67210, 67228 Repair of surrounding eye structures15823, 67900, 67904, 67917, 67924 GastrointestinalGI endoscopy procedures43239, 43235, 43248, 43249, 43251, 44361, 45330, 45331, 45378, 45380, 45381, 45383, 45384, 45385,46221 Swallowing tube (esophagus)43450 Hernia repair49505 GI screening proceduresG0105, G0121
65756, V2785 Laser procedure of eye65855, 66761, Glaucoma procedures66170, 66180, Cataract procedures66982, Injection of eye67028, J2778, J3300, J3396 Retina, macular and posterior segment procedures67041, 67042, 67210, Repair of surrounding eye structures15823, 67900, 67904, 67917, GastrointestinalGI endoscopy procedures43239, 43235, 43248, 43249, 43251, 44361, 45330, 45331, 45378, 45380, 45381, 45383, 45384, 45385,46221 Swallowing tube (esophagus)43450 Hernia repair49505 GI screening proceduresG0105, G0121")
28
Organ SystemCMS Procedure CategorySurgical Procedure Codes GenitourinaryKidney stone fragmentation50590 Bladder related procedures52000, 52005, 52204, 52281, 52310, 52332 Prostate biopsy55700 Radiologic procedures (GU)74420 Ultrasound procedures (GU)76872 MusculoskeletalJoint or muscle aspiration or injection20610 Removal of musculoskeletal implants20680 Repair of tendons and ligaments23412 Repair of foot, toes, fingers, and wrist26055, 28270, 28285, 28296, 29848 Removal of musculoskeletal lesion26160 Joint arthroscopy29824, 29826, 29827, 29880, 29881, 29823, 29822 Musculoskeletal drug injectionJ0585, J0878, J0131
74420 Ultrasound procedures (GU)76872 MusculoskeletalJoint or muscle aspiration or injection20610 Removal of musculoskeletal implants20680 Repair of tendons and ligaments23412 Repair of foot, toes, fingers, and wrist26055, 28270, 28285, 28296, Removal of musculoskeletal lesion26160 Joint arthroscopy29824, 29826, 29827, 29880, 29881, 29823, Musculoskeletal drug injectionJ0585, J0878, J0131")
29
Organ SystemCMS Procedure CategorySurgical Procedure Codes NervousInjection procedures in or around the spine62310, 62311, 64479, 64480, 64483, 64484, 64490, 64491, 64492, 64493, 64494, 64495, 64622, 64623, 64626, 64627, 64633, 64634, 64635, 64636, 64640, G0260, J2278 Device implant63650 Nerve decompression64718 Repair of foot, toes, fingers, and wrist64721 RespiratorySinus procedure30140, 31255, 31267 SkinSkin procedures including debridement, reconstructive, wound closure, excision and/or repair 11042, 13132, 14040, 14060, 15260, 17311, Q4101, Q4102, Q4106 Multi-system*Brachytherapy Cancer treatment with angiogenesis inhibitor *Multi-System: procedures that can be performed in more than one organ system. C2638, C2639, C2640, C2641 C9257

30
Claims Based Reporting–Quality Data Codes (QDCs) Patient Burn Patient Fall Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal (www.qualitynet.org) www.qualitynet.org Safe Surgery Check List Use Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) (www.cdc.gov/nhsn/index.html)www.cdc.gov/nhsn/index.html Influenza Vaccination Coverage Among Health Care Personnel
 Patient Burn Patient Fall Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal ( Safe Surgery Check List Use Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) ( Influenza Vaccination Coverage Among Health Care Personnel")
31
Web Based Reporting via QualityNet Secure Portal (www.qualitynet.org) www.qualitynet.org Safe Surgery Check List Use Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients ASC Volume of Selected Procedures for all-patients No reporting for these two measures for 2013 Data Collection for these two measures will resume January 1 - December 31, 2014 Data Reporting for calendar year 2014 will be from January 1- August 15, 2015

32
ASC Program Measurement Set for the CY 2016 Payment Determination ASC-1: Patient Burn ASC-2: Patient Fall ASC-3: Wrong Site, Wrong Side, Wrong Patient, Wrong Procedure, Wrong Implant ASC-4: Hospital Transfer/Admission ASC-5: Prophylactic Intravenous (IV) Antibiotic Timing ASC-6: Safe Surgery Checklist Use ASC-7: ASC Facility Volume Data on Selected ASC Surgical Procedures {Procedure Category Corresponding HCPCS Codes: Eye/Gastrointestinal/Genitourinary/Musculoskeletal/ Nervous/Respiratory/Skin/Multi-system} ASC- 8: Influenza Vaccination Coverage among Healthcare Personnel * *New measure for CY 2016 payment determination
 Antibiotic Timing ASC-6: Safe Surgery Checklist Use ASC-7: ASC Facility Volume Data on Selected ASC Surgical Procedures {Procedure Category Corresponding HCPCS Codes: Eye/Gastrointestinal/Genitourinary/Musculoskeletal/ Nervous/Respiratory/Skin/Multi-system} ASC- 8: Influenza Vaccination Coverage among Healthcare Personnel * *New measure for CY 2016 payment determination")
33
Influenza Vaccination Coverage among Healthcare Personnel (HCP) Intent: assess the percentage of HCP immunized for influenza during the flu season 3 Categories of Healthcare Personnel will include: Employee on facility payroll Licensed independent practitioners, e.g. physicians (MDs, DO), advance practice nurses and physician assistants who are affiliated with the facility who do not receive a direct paycheck from the facility Adult students/trainees and volunteers who do not receive a direct paycheck from the facility
, advance practice nurses and physician assistants who are affiliated with the facility who do not receive a direct paycheck from the facility Adult students/trainees and volunteers who do not receive a direct paycheck from the facility.")
34
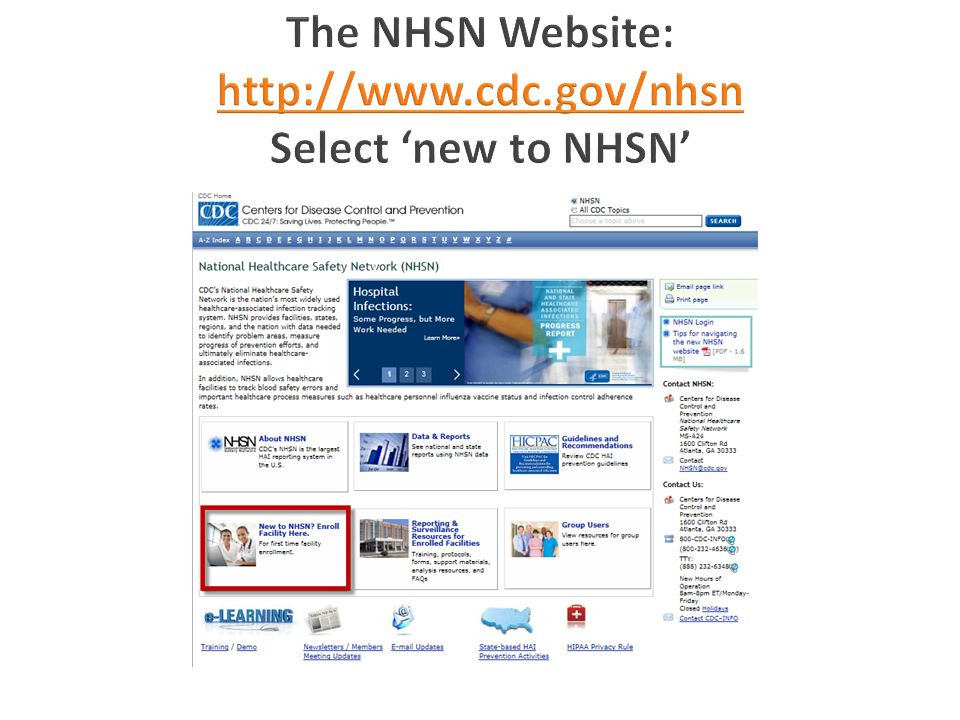
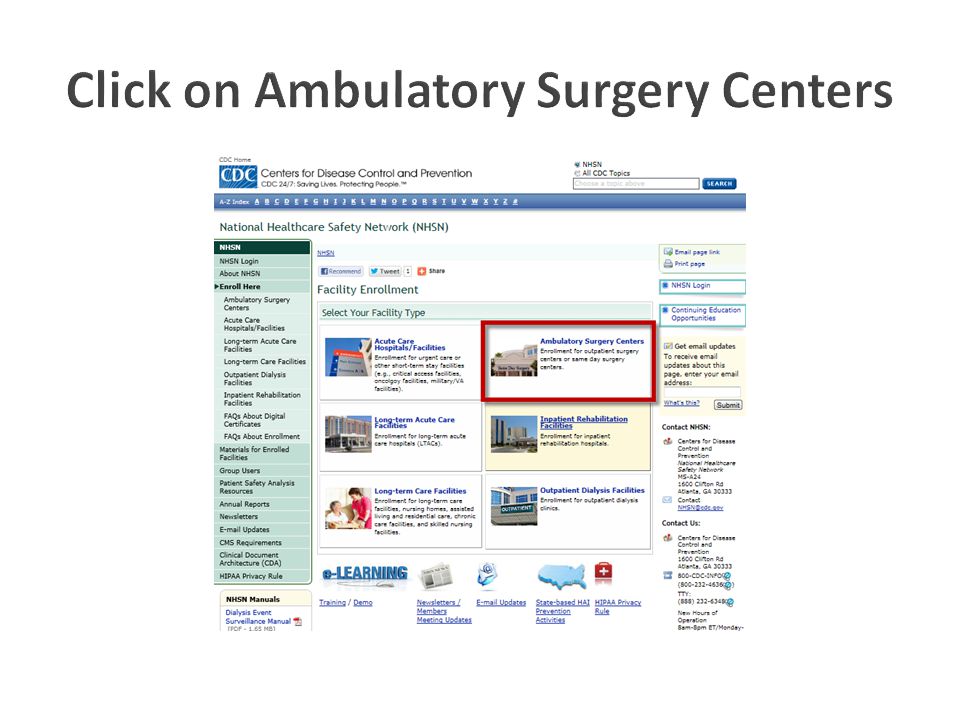
Data collection begins with immunizations for the flu season October 1, 2014 through March 31, 2015 CDC’s NHSN website for enrollment: www.cdc.gov/nhsn/ambulatory-surgery/enroll.html www.cdc.gov/nhsn/ambulatory-surgery/enroll.html ◦ “NHSN facility administrator enrollment guide” (step by step) Deadline for data submission for the 2014-2015 flu season through May 15, 2015.
 Deadline for data submission for the flu season through May 15, 2015.")
38
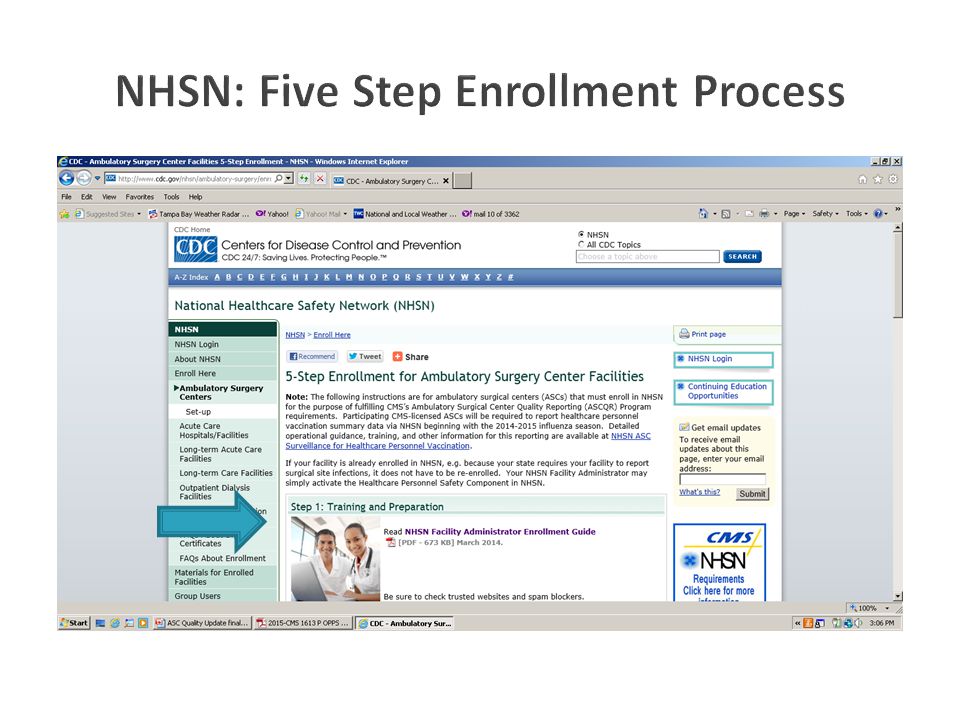
Review and accept the NHSN rules of behavior Register with SAMS SAMS = Secure Access Management Services, a federal information technology (IT) system that gives authorized personnel secure access to non-public CDC applications
 system that gives authorized personnel secure access to non-public CDC applications")
39
Users must fax or mail notarized proof of identity to CDC. You will receive a grid card in the mail in order to access NHSN. Complete and submit required forms (facility information, facility survey, consent form) Reporting (https://sams.cdc.gov ) user authorization through Secure Access Management Services (SAMS) is required for access to NHSN.https://sams.cdc.gov
 Reporting ( ) user authorization through Secure Access Management Services (SAMS) is required for access to NHSN.")
40
Employee HCPNon-Employee HCP Employees (staff on facility payroll) Licensed independent practitioners: Physicians, advanced practice nurses, & physician assistants Adult students/ trainees & volunteers Other contract personnel 1. Number of HCP who worked at this healthcare facility for at least 1 day between October 1 and March 31 2. Number of HCP who received an influenza vaccination at this healthcare facility since influenza vaccine became available this season 3. Number of HCP who provided a written report or documentation of influenza vaccination outside this healthcare facility since influenza vaccine became available this season 4. Number of HCP who have a medical contraindication to the influenza vaccine 5. Number of HCP who declined to receive the influenza vaccine 6. Number of HCP with unknown vaccination status (or criteria not met for questions 2-5 above

41
Employee HCP Non-Employee HCP: Licensed independent practitioners (physicians, advance practice nurses, and physician assistants) Non-Employee HCP: Adult students/trainees and volunteers 41
 Non-Employee HCP: Adult students/trainees and volunteers 41")
42
Influenza vaccinations ◦ Received at this healthcare facility ◦ Received elsewhere Medical contraindications Declinations Unknown status

43
10 + 20 + 15 + 5 + 5 = 55 70 + 10 + 10 + 5 + 5 = 100 20 + 2 + 1 + 1 + 1 = 25

44
Claims Based Reporting–Quality Data Codes (QDCs) Patient Burn Patient Fall Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal (www.qualitynet.org)www.qualitynet.org Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) (www.cdc.gov/nhsn/index.html) www.cdc.gov/nhsn/index.html Influenza Vaccination Coverage Among Health Care Personnel Influenza Vaccination Coverage Among Health Care Personnel
 Patient Burn Patient Fall Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal ( Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) ( Influenza Vaccination Coverage Among Health Care Personnel Influenza Vaccination Coverage Among Health Care Personnel")
45
The CDC conducted live training webinars in August to cover the requirements for collecting and entering HCP influenza vaccination summary data. A recording of the webinar has been posted at: http://www2.cdc.gov/vaccines/ed/nhsn/, so staff can review the recorded training and slides. http://www2.cdc.gov/vaccines/ed/nhsn/ For questions on HCP influenza vaccination summary reporting, please send an e-mail to: NHSN@cdc.gov and include “HPS Flu Summary-ASC” in the subject line. NHSN@cdc.gov

46
Released on November 27, 2013 www.gpo.gov/fdsys/pkg/FR-2013-12-10/pdf/2013- 28737.pdf www.gpo.gov/fdsys/pkg/FR-2013-12-10/pdf/2013- 28737.pdf ASC Quality Reporting Program begins on page 974 ; Section XV. Requirements for ASC Quality Reporting Program 3 Quality Measures for CY 2016: page 979 50% minimum reporting threshold: page 1025 Exempting low volume providers: page 1027 (less than 240 Medicare claims/year)
.")
47
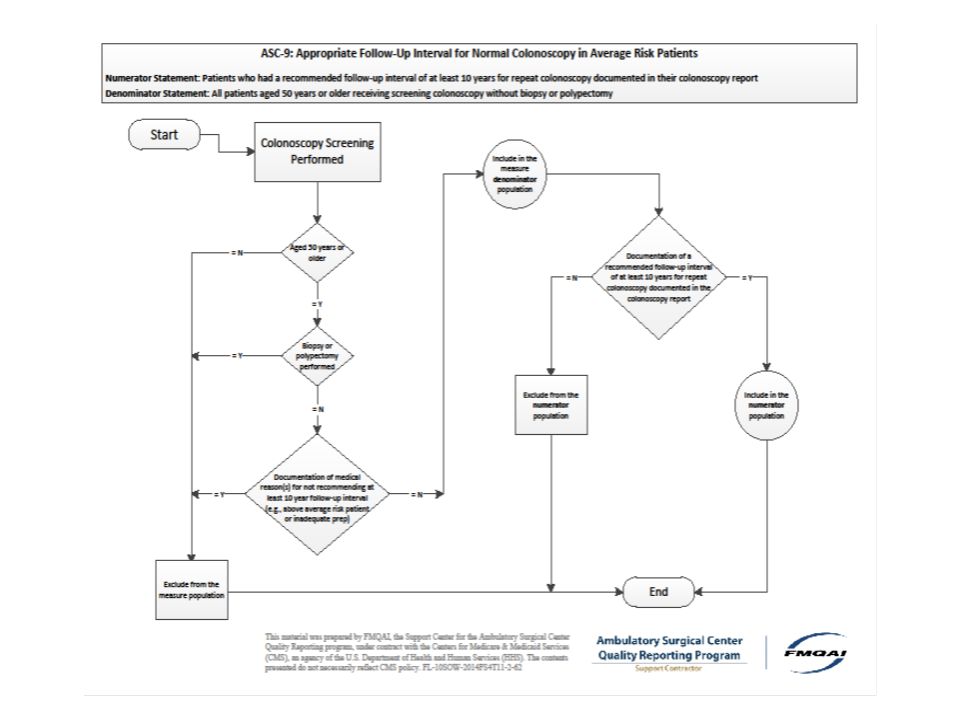
Previous ASC 1- ASC 8 plus 3 Additional Measures: Endoscopy/Poly Surveillance: Appropriate follow-up interval for normal colonoscopy in average risk patients (NQF #0658); Endoscopy/Poly Surveillance: Colonoscopy Interval for Patients with a History of Adenomatous Polyps – Avoidance of Inappropriate Use (NQF #0659); and Cataracts: Improvement in Patient’s Visual Function within 90 Days Following Cataract Surgery (NQF #1536). * NQF= National Quality Forum (www.qualityforum.org)www.qualityforum.org

48
Denominator: patients aged 50 years and older receiving screening colonoscopy without biopsy or polypectomy Numerator: patients who had a recommended follow- up interval of 10 years for repeat colonoscopy documented in their colonoscopy report* *follow-up interval is at least 10 years from the date of the current colonoscopy *physician’s documentation in the colonoscopy report

49
Exclusions: documentation of medical reasons for not recommending at least a 10-year follow-up (above average risk, inadequate prep) Inclusions: Patients aged ≥ 50 on date of encounter And ICD-9-CM Diagnosis code: V76.51 And CPT or HCPCS: 45378, G0121 Without CPT Category I Modifiers: 52, 53, 73, 74 Without ICD-9-CM Diagnosis codes: V18.51, V12.72, V16.0, V10.05 (The ICD-9 codes will be updated when the conversion to ICD-10 occurs)
 Inclusions: Patients aged ≥ 50 on date of encounter And ICD-9-CM Diagnosis code: V76.51 And CPT or HCPCS: 45378, G0121 Without CPT Category I Modifiers: 52, 53, 73, 74 Without ICD-9-CM Diagnosis codes: V18.51, V12.72, V16.0, V10.05 (The ICD-9 codes will be updated when the conversion to ICD-10 occurs)")
50
Denominator: number of patients 18 years and older receiving a surveillance colonoscopy with a history of a prior colonic polyp in a previous colonoscopy Numerator: number of patients who had an interval of three or more years since their last colonoscopy* *Information regarding performance interval can be obtained from the medical record.

51
Exclusions: Documentation of medical reason(s) for an interval of less than three years since the last colonoscopy (for example, last colonoscopy incomplete, last colonoscopy had inadequate prep, piecemeal removal of adenomas, or last colonoscopy found greater than 10 adenomas) Documentation of a system reason(s) for an interval less than three years since last colonoscopy (for example, unable to locate previous colonoscopy report, previous colonoscopy report was incomplete)
 for an interval of less than three years since the last colonoscopy (for example, last colonoscopy incomplete, last colonoscopy had inadequate prep, piecemeal removal of adenomas, or last colonoscopy found greater than 10 adenomas) Documentation of a system reason(s) for an interval less than three years since last colonoscopy (for example, unable to locate previous colonoscopy report, previous colonoscopy report was incomplete)")
52
Inclusions: Patients aged ≥ 18 years on date of encounter And Diagnosis for history of colonic polyp(s) (ICD-9-CM): V12.72, V10.05 And CPT or HCPCS: 44388, 44389, 44392, 44393, 44394, 45355, 45378, 45380, 45381, 45383, 45384, 45385, G0105 Without CPT Category I Modifiers: 52, 53, 73 or 74 (The ICD-9 codes will be updated when the conversion to ICD-10 occurs)
 (ICD-9-CM): V12.72, V10.05 And CPT or HCPCS: 44388, 44389, 44392, 44393, 44394, 45355, 45378, 45380, 45381, 45383, 45384, 45385, G0105 Without CPT Category I Modifiers: 52, 53, 73 or 74 (The ICD-9 codes will be updated when the conversion to ICD-10 occurs)")
53
Denominator: number of patients aged 18 years and older in sample who had cataract surgery and completed both a pre-operative and post-operative visual function instrument Numerator: number of patients 18 years and older who had improvement in visual function achieved within 90 days following cataract surgery, based on completing both a pre-operative and post-operative visual function instrument

54
Examples of tools for visual function assessment include, but are not limited to: National Eye Institute-Visual Function Questionnaire – VFQ-25 www.rand.org/health/surveys_tools/vfq.html Visual Function (VF)-14 www.med.teikyo-u.ac.jp/~ortho/med/reh/VF-14.html Modified VF-8 http://ascrs.org/sites/default/files/resources/2013%20Cataracts%20Measure s%20Group%20Post-Surgery%20VF-8R_0.pdf Modified Catquest-9 http://download.lww.com/wolterskluwer_vitalstream_com/PermaLink/OPX/ A/ OPX_90_8_2013_04_04_LUNDSTROM_201940_SDC1.pdf
-14 Modified VF-8 s%20Group%20Post-Surgery%20VF-8R_0.pdf Modified Catquest-9 A/ OPX_90_8_2013_04_04_LUNDSTROM_201940_SDC1.pdf")
55
55

59
Population Per Year0-900 Yearly Sample Size63 Quarterly Sample Size16 Monthly Sample Size6 Population Per Year≥901 Yearly Sample Size96 Quarterly Sample Size24 Monthly Sample Size8

60
Claims Based Reporting–Quality Data Codes (QDCs) Patient Burn Patient Fall Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal (www.qualitynet.org)www.qualitynet.org Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) (www.cdc.gov/nhsn/index.html)www.cdc.gov/nhsn/index.html Influenza Vaccination Coverage Among Health Care Personnel Web Based Reporting via QualityNet Secure Portal (www.qualitynet.org) www.qualitynet.org Endoscopy/Polyp Surveillance (normal) Endoscopy/Polyp Surveillance (normal) Endoscopy/Polyp Surveillance (adenomatous) Endoscopy/Polyp Surveillance (adenomatous) Cataract: improvement in visual function- voluntary Cataract: improvement in visual function- voluntary
 Patient Burn Patient Fall Wrong Site, Side, Patient, Procedure, Implant Hospital Admission/Transfer Prophylactic IV Antibiotic Timing Web Based Reporting via QualityNet Secure Portal ( Safe Surgery Check List Use ASC Volume of Selected Procedures for all-patients Web Based Reporting Via Centers for Disease Control and Prevention (CDC) National Health Care Safety Network (NHSN) ( Influenza Vaccination Coverage Among Health Care Personnel Web Based Reporting via QualityNet Secure Portal ( Endoscopy/Polyp Surveillance (normal) Endoscopy/Polyp Surveillance (normal) Endoscopy/Polyp Surveillance (adenomatous) Endoscopy/Polyp Surveillance (adenomatous) Cataract: improvement in visual function- voluntary Cataract: improvement in visual function- voluntary")
61
Released on October 31, 2014 http://www.ofr.gov/(S(j4muxl5s4vqongwcshdlh533))/O FRUpload/OFRData/2014-26146_PI.pdf http://www.ofr.gov/(S(j4muxl5s4vqongwcshdlh533))/O FRUpload/OFRData/2014-26146_PI.pdf ASC Quality Reporting Program begins on page 781: Section XIV. Requirements for ASC Quality Reporting Program

62
Previous ASC 1- ASC 10 plus ASC 11: Cataracts: Improvement in Patient’s Visual Function within 90 Days Following Cataract Surgery (NQF #1536) voluntary NQF = National Quality Forum (www.qualityforum.org)www.qualityforum.org
 voluntary NQF = National Quality Forum (")
63
Previous ASC 1- ASC 10 plus ASC 11: Cataracts: Improvement in Patient’s Visual Function within 90 Days Following Cataract Surgery (NQF #1536) voluntary 1 Additional Measure: ASC 12: Facility Seven-Day Risk-Standardized Hospital Visit Rate after Outpatient Colonoscopy NQF = National Quality Forum (www.qualityforum.org)www.qualityforum.org
 voluntary 1 Additional Measure: ASC 12: Facility Seven-Day Risk-Standardized Hospital Visit Rate after Outpatient Colonoscopy NQF = National Quality Forum (")
64
Claims based measure No additional data submission from ASCs The measure outcome is all unplanned hospital visits (admissions, observation stays, and emergency department [ED] visits) within 7 days of the procedure.
![ Claims based measure No additional data submission from ASCs The measure outcome is all unplanned hospital visits (admissions, observation stays, and emergency department [ED] visits) within 7 days of the procedure.](http://images.slideplayer.com/14/4397851/slides/slide_64.jpg " Claims based measure No additional data submission from ASCs The measure outcome is all unplanned hospital visits (admissions, observation stays, and emergency department [ED] visits) within 7 days of the procedure.")
65
In 2015, Medicare will perform a “dry run” of this measure. A dry run is a preliminary analysis of data in which ASCs may review their measure results, and ask questions about and become familiar with the measure methodology. The most recent complete claims samples (usually 6-9 months prior to the start date) for dry runs will be used.
 for dry runs will be used..")
66
The dry run will generate confidential reports at the patient level, indicating whether the patient had a hospital visit, the type of visit (admission, ER visit, or observational stay), the admitting facility, and the principal discharge diagnosis. The ASC will have the opportunity to receive individual patient data and information contained within individual patient records in order to identify performance gaps and develop quality improvement strategies. Dry runs results ARE NOT linked to public reporting or payment determinations. ASCs can review their confidential dry run reports at www.qualitynet.org. www.qualitynet.org

67
For the CY 2018 payment determination, paid Medicare Fee For Service claims from January 1 – December 31, 2016 will be used (calendar years 2 years before the payment determination calendar year.

68
Patient experience of care: ASC Consumer Assessment of Healthcare Providers and Systems (CAHPS) patient experience survey Care Plan- (percentage of patients 65 years and older who have a care plan or surrogate decision documented in the medical record) Hair removal Normothermia Unplanned anterior vitrectomy
 patient experience survey Care Plan- (percentage of patients 65 years and older who have a care plan or surrogate decision documented in the medical record) Hair removal Normothermia Unplanned anterior vitrectomy")
69
ASC Quality Collaboration website (measure summary and implementation guide)http://ascquality.org/qualitymeasures.cfmhttp://ascquality.org/qualitymeasures.cfm Ambulatory Surgery Center Association (ASCA) http://www.ascassociation.org QualityNet website (CMS Specifications Manual & Email Notifications) http://qualitynet.org FMQAI website (CMS national support contractor) http://oqrsupport.org CMS certification number (CCN) Look-Up Tool (allows a facility to enter its National Provider Identifier (NPI) in the search box to find its CCN) http://www.oqrsupport.com/asc/ccn
 Ambulatory Surgery Center Association (ASCA) QualityNet website (CMS Specifications Manual & Notifications) FMQAI website (CMS national support contractor) CMS certification number (CCN) Look-Up Tool (allows a facility to enter its National Provider Identifier (NPI) in the search box to find its CCN)")
70
Contact FMQAI for Program Questions at oqrsupport@sdps.com oqrsupport@sdps.com or via phone (866) 800-8756 Monday through Friday, 7 a.m. to 6 p.m. Eastern Time Contact the QualityNet Help Desk for Technical Issues at qnetsupport@sdps.org or via phone (866) 288-8912 Monday through Friday, 7 a.m. to 7 p.m. Central Time
 Monday through Friday, 7 a.m. to 7 p.m. Central Time.")
71
Federal Register / Vol. 76, No. 230 / Wednesday, November 30, 2011 / Rules and Regulations. Available at http://www.gpo.gov/fdsys/pkg/FR-2011-11-30/pdf/2011-28612.pdfhttp://www.gpo.gov/fdsys/pkg/FR-2011-11-30/pdf/2011-28612.pdf Federal Register / Vol. 77, No. 170 / Friday, August 31, 2012/ Rules and Regulations. Available at http://www.gpo.gov/fdsys/pkg/FR-2012-08-31/pdf/2012-19079.pdf http://www.gpo.gov/fdsys/pkg/FR-2012-08-31/pdf/2012-19079.pdf Federal Register / Vol. 77, No. 221 / Thursday, November 15, 2012 / Rules and Regulations. Available at http://www.gpo.gov/fdsys/pkg/FR-2012-11-15/pdf/2012-26902.pdfhttp://www.gpo.gov/fdsys/pkg/FR-2012-11-15/pdf/2012-26902.pdf Federal Register / Vol. 78, No. 237 / Tuesday, December 10, 2013/ Rules and Regulations. Available at http://www.gpo.gov/fdsys/pkg/FR-2013-12-10/pdf/2013-28737.pdf Federal Register / Vol. 79, No. 134 / Monday, July 14, 2014/ Rules and Regulations. Available at http://www.gpo.gov/fdsys/pkg/FR-2014-07-14/pdf/2014-15939.pdf http://www.gpo.gov/fdsys/pkg/FR-2014-07-14/pdf/2014-15939.pdf ASC Quality Collaboration Implementation Guide, Version 2.1, April 2014. Available at http://ascquality.org/documents/ASCQC.Implementation.Guide.2.1April2014.pdf http://ascquality.org/documents/ASCQC.Implementation.Guide.2.1April2014.pdf CMS ASC Quality Reporting Program Quality Measures Specifications Manual, Version 4.0, June 2014. Available at www.qualitynet.orgwww.qualitynet.org Quality Net at www.qualitynet.orgwww.qualitynet.org National Healthcare Safety Network www.cdc.gov/nhsn/www.cdc.gov/nhsn/ http://www.ofr.gov/(S(j4muxl5s4vqongwcshdlh533))/OFRUpload/OFRData/2014-26146_PI.pdf http://www.ofr.gov/(S(j4muxl5s4vqongwcshdlh533))/OFRUpload/OFRData/2014-26146_PI.pdf

72
Gina Throneberry, RN, MBA, CASC, CNOR Ambulatory Surgery Center Association (ASCA) Director or Education and Clinical Affairs gthroneberry@ascassociation.org gthroneberry@ascassociation.org
 Director or Education and Clinical Affairs")
Similar presentations








 Reviews Under the Benefits Improvement and Protection Act §521 Presented by Alabama Quality Assurance Foundation.>")



 Final Regulations.>")










 ◦28 CAH’s (35miles or “necessary.>")
