Download presentation
Presentation is loading. Please wait.

1
Clinical Care Management at UNC Hospitals Medicine House Staff July 9, 2009

2
Case Managers (CM) Nurses, Social Workers, other professional specialists Nurses, Social Workers, other professional specialists Assigned by service Assigned by service Facilitators for patient throughput Facilitators for patient throughput Coordinate discharge planning Coordinate discharge planning Expert consultants on disposition settings & regulations Expert consultants on disposition settings & regulations
 Nurses, Social Workers, other professional specialists Nurses, Social Workers, other professional specialists Assigned by service Assigned by service Facilitators for patient throughput Facilitators for patient throughput Coordinate discharge planning Coordinate discharge planning Expert consultants on disposition settings & regulations Expert consultants on disposition settings & regulations")
3
Tell Your Case Manager Clinical goals/endpoints Clinical goals/endpoints LOS (if you know it) LOS (if you know it) Post discharge care needs Post discharge care needs Barriers you know about Barriers you know about
 LOS (if you know it) Post discharge care needs Post discharge care needs Barriers you know about Barriers you know about")
4
Your Case Manager Can Tell You Discharge options available, considering Discharge options available, considering –Payor coverage –Family/support –Transportation Documentation needs Documentation needs The status of the discharge plan The status of the discharge plan

5
Don’t Promise What Can’t be Delivered Home vs SNF for infusion Home vs SNF for infusion Home Health vs Outpatient care Home Health vs Outpatient care Medicare covered placement Medicare covered placement Hospital funding Hospital funding

6
Clinical Social Workers Assigned to specific areas Assigned to specific areas –Psychiatry –Transplant –Some pediatric areas Psychosocial assessments and therapeutic interventions Psychosocial assessments and therapeutic interventions Available as consultants to case managers Available as consultants to case managers

7
TPN and Infusion Specialists Consultants to Case Managers Consultants to Case Managers Coordinate arrangements for post- discharge Coordinate arrangements for post- discharge –IV antibiotics –IV hydration –TPN

8
CCM and the UNC Discharge Summary Multidisciplinary Multidisciplinary –Physician –Case Manager –Other team designees Contains Contains –Traditional discharge summary information –Post discharge orders and instructions –Reconciled medications

9
Utilization Managers (UM) Assigned to every patient in a bed Assigned to every patient in a bed Perform payor reviews Perform payor reviews Depend on clear and precise documentation Depend on clear and precise documentation Experts in CMS regulations for Experts in CMS regulations for –Bed billing status –Qualifying stays for placement
 Assigned to every patient in a bed Assigned to every patient in a bed Perform payor reviews Perform payor reviews Depend on clear and precise documentation Depend on clear and precise documentation Experts in CMS regulations for Experts in CMS regulations for –Bed billing status –Qualifying stays for placement")
10
Executive Health Resources (EHR) Contracted physician advisor consultants Contracted physician advisor consultants Experts on CMS regulations and reimbursement Experts on CMS regulations and reimbursement Contact physicians to discuss care plans and documentation Contact physicians to discuss care plans and documentation
 Contracted physician advisor consultants Contracted physician advisor consultants Experts on CMS regulations and reimbursement Experts on CMS regulations and reimbursement Contact physicians to discuss care plans and documentation Contact physicians to discuss care plans and documentation")
11
So, Who Decides The Status? Federal Government Federal Government –Centers for Medicare and Medicaid Services (CMS) Policy –Office of the Inspector General (OIG) Audits & Retractions Evidence based criteria sets Evidence based criteria sets –InterQual Expert Physician Advisors Expert Physician Advisors –Executive Health Resources (EHR)
 Policy –Office of the Inspector General (OIG) Audits & Retractions Evidence based criteria sets Evidence based criteria sets –InterQual Expert Physician Advisors Expert Physician Advisors –Executive Health Resources (EHR).")
12
Other CCM Functions Payor Authorization Payor Authorization Medical Necessity Denials Medical Necessity Denials Bed Management Bed Management Transfer Center Transfer Center Psychiatry Admissions Psychiatry Admissions Avoidable Delay Tracking Avoidable Delay Tracking

13
Why CCTs Care About Bed Billing Status Short stays are a government audit focus Short stays are a government audit focus Overuse of Observation Overuse of Observation –Lost revenue for hospital (& soon physician) –Inappropriate co-pays to patient Inappropriate use of Inpatient Inappropriate use of Inpatient –Subject to fraud charges –Pay-backs, penalties, & press
 –Inappropriate co-pays to patient Inappropriate use of Inpatient Inappropriate use of Inpatient –Subject to fraud charges –Pay-backs, penalties, & press")
14
Billing Status Outpatient Outpatient –Extended Recovery (EXR) –Observation (OBS) Inpatient (INP) Inpatient (INP) Patients in any of these statuses can be “admitted” to a bed in the hospital.
 –Observation (OBS) Inpatient (INP) Inpatient (INP) Patients in any of these statuses can be admitted to a bed in the hospital.")
15
Extended Recovery (EXR) Routine or pre-planned post-operative or procedure recovery Routine or pre-planned post-operative or procedure recovery Short stay services following uncomplicated treatment or procedure such as chemo or infusion therapy Short stay services following uncomplicated treatment or procedure such as chemo or infusion therapy
 Routine or pre-planned post-operative or procedure recovery Routine or pre-planned post-operative or procedure recovery Short stay services following uncomplicated treatment or procedure such as chemo or infusion therapy Short stay services following uncomplicated treatment or procedure such as chemo or infusion therapy")
16
EXR Characteristics Always (almost*) planned/elective Always (almost*) planned/elective Uncomplicated procedure Uncomplicated procedure No licensed bed required No licensed bed required No physician’s order for billing status required No physician’s order for billing status required Billed as outpatient unit price based on procedure code Billed as outpatient unit price based on procedure code No room/board/ancillary billing No room/board/ancillary billing May advance to Observation or Inpatient May advance to Observation or Inpatient *Also used for “social admits”, allows billing of some lab/procedure charges without billing bed charges
 planned/elective Always (almost*) planned/elective Uncomplicated procedure Uncomplicated procedure No licensed bed required No licensed bed required No physician’s order for billing status required No physician’s order for billing status required Billed as outpatient unit price based on procedure code Billed as outpatient unit price based on procedure code No room/board/ancillary billing No room/board/ancillary billing May advance to Observation or Inpatient May advance to Observation or Inpatient *Also used for social admits , allows billing of some lab/procedure charges without billing bed charges")
17
Observation (OBS) Services & monitoring to evaluate and determine the need for inpatient admission Services & monitoring to evaluate and determine the need for inpatient admission Services are covered only by the order of a physician or other individual… authorized to admit patients. Services are covered only by the order of a physician or other individual… authorized to admit patients.

18
OBS Characteristics Always unplanned Always unplanned No licensed bed required No licensed bed required Must have physician’s order for Observation Must have physician’s order for Observation Billed on a per-hour basis to patient’s outpatient benefits Billed on a per-hour basis to patient’s outpatient benefits Some services billed directly to the patient Some services billed directly to the patient Case may advance to inpatient if medical necessity is established Case may advance to inpatient if medical necessity is established Not a qualifying stay for SNF placement Not a qualifying stay for SNF placement

19
OBS Billing Ends When EITHER: Observation status is no longer justified* Observation status is no longer justified* –Observation intensity of service criteria no longer met –Documentation does not substantiate medical necessity for continued observation services * If the patient remains in-house, hourly room & board charges cannot be billed.

20
OR: Inpatient status is justified Inpatient status is justified –Criteria for inpatient status are met –Documentation substantiates a defensible need for an inpatient admission. Clinical condition change Clinical condition change Confirmed diagnosis Confirmed diagnosis Initiation of inpatient treatment Initiation of inpatient treatment Intent Intent

21
The OBS/Inpatient Mix Patient begins stay appropriate for Observation Patient begins stay appropriate for Observation Information or circumstances arise that justify an Inpatient admission Information or circumstances arise that justify an Inpatient admission Inpatient begins at the time of order entry Inpatient begins at the time of order entry

22
Now, for Inpatient May be planned or unplanned May be planned or unplanned Requires a licensed bed Requires a licensed bed Requires medical necessity justification Requires medical necessity justification Begins with a physician’s order for Inpatient billing status Begins with a physician’s order for Inpatient billing status Can be corrected to outpatient under certain circumstances (Condition Code 44) Can be corrected to outpatient under certain circumstances (Condition Code 44)
 Can be corrected to outpatient under certain circumstances (Condition Code 44)")
23
Medical Necessity for Inpatient Status Criteria + Intent/Risk

24
Medical Necessity Criteria Specialist written Specialist written Evidence based Evidence based Very specific Very specific Revised annually Revised annually InterQual used by Medicare Quality Improvement Organization (QIO) InterQual used by Medicare Quality Improvement Organization (QIO) Milliman used by RAC (Connelly Consulting) Milliman used by RAC (Connelly Consulting)
 InterQual used by Medicare Quality Improvement Organization (QIO) Milliman used by RAC (Connelly Consulting) Milliman used by RAC (Connelly Consulting)")
25
Medical Necessity: Intent/Risk Severity of signs and symptoms Severity of signs and symptoms Differential diagnosis Differential diagnosis Clinical predictability of something adverse happening Clinical predictability of something adverse happening Plan for management that requires an inpatient setting Plan for management that requires an inpatient setting *Documentation of intent and risk must come from the admitting team.

26
Why the Urgency for Documentation? Inpatient billing begins with an inpatient order Inpatient billing begins with an inpatient order –Inpatient order requires medical necessity –Medical necessity requires documentation from the admitting team –Documentation delay = inpatient order delay = loss of billable inpatient days

27
Provider Liable Medicare case with inpatient order and no documented medical necessity Medicare case with inpatient order and no documented medical necessity D/C order written D/C order written Billing status order cannot be manipulated Billing status order cannot be manipulated Billing for inpatient without documented medical necessity is fraud Billing for inpatient without documented medical necessity is fraud The hospital (and soon the physician) cannot bill Medicare for the stay The hospital (and soon the physician) cannot bill Medicare for the stay Currently averaging $500,000/month Currently averaging $500,000/month
 cannot bill Medicare for the stay The hospital (and soon the physician) cannot bill Medicare for the stay Currently averaging $500,000/month Currently averaging $500,000/month")
28
*Qualifying Hospital Stay for SNF Placement Medically necessary admission Medically necessary admission –Severity of Illness and Intensity of Service justify inpatient level of care (InterQual) 3 day inpatient stay within the 30 days preceding SNF admission 3 day inpatient stay within the 30 days preceding SNF admission Inpatient criteria met for each of 3 consecutive days Inpatient criteria met for each of 3 consecutive days 3 day stays resulting in SNF are an OIG focus
 3 day inpatient stay within the 30 days preceding SNF admission 3 day inpatient stay within the 30 days preceding SNF admission Inpatient criteria met for each of 3 consecutive days Inpatient criteria met for each of 3 consecutive days 3 day stays resulting in SNF are an OIG focus")
29
Summing Up Bed Status Billing Status Planned vs unplanned Medical necessity required? Billable? EXRPlannedNoNo OBSUnplannedYesSome INPEitherYesYes

30
Observation Advisory Medicare primary patients only Medicare primary patients only Billing status changed from INP to OBS Billing status changed from INP to OBS Advises patients of billing status and implications Advises patients of billing status and implications Delivered by CCM Utilization Managers Delivered by CCM Utilization Managers

31
Documentation Pointers

32
No more “A” word Abolish the “Admit” word Abolish the “Admit” word –CMS = Inpatient –UNC = Place Patient in Bed –Does not define a billing status –Has caused payment retractions

33
Know what Observation means Observation and Monitoring are different Observation and Monitoring are different –“Observation” is a billing status –“Monitoring” is a better term for clinical activity

34
Avoid Contradictions Admit to OBS Admit to OBS Admit for observation Admit for observation Inpatient Observation Inpatient Observation

35
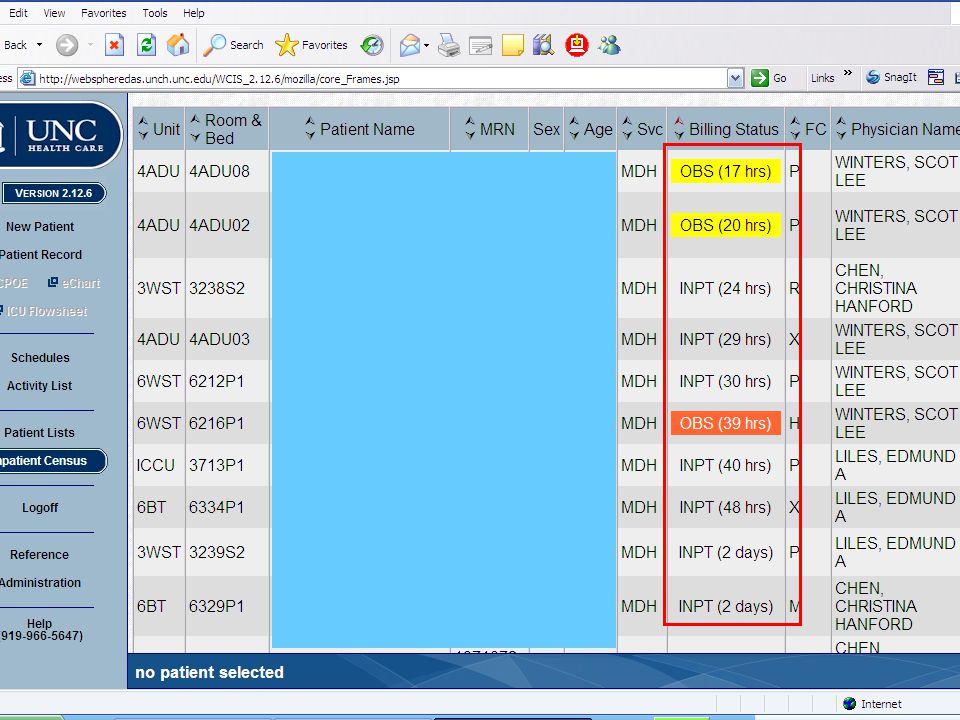
Which Patients are on What Status?

38
Summing Up Your Case Manager can be your best friend Your Case Manager can be your best friend Your Case Manager can’t do good work without good information Your Case Manager can’t do good work without good information Your Utilization Manager helps hospital & MD get paid for the care we provide Your Utilization Manager helps hospital & MD get paid for the care we provide Precise documentation is better than “more” documentation Precise documentation is better than “more” documentation

39
Contacts Director: Marie Bossert (3-2766) Director: Marie Bossert (3-2766) Managers: Managers: –CM Med/Surg Sherri Branski (3-0599) Sherri Branski (3-0599) –UM Med/Surg Chris Wehner (6-8290) Chris Wehner (6-8290) –Transfer center, Bed Mmgt Andrea Soltau-Talbot (6-6544) Andrea Soltau-Talbot (6-6544)
 Director: Marie Bossert (3-2766) Managers: Managers: –CM Med/Surg Sherri Branski (3-0599) Sherri Branski (3-0599) –UM Med/Surg Chris Wehner (6-8290) Chris Wehner (6-8290) –Transfer center, Bed Mmgt Andrea Soltau-Talbot (6-6544) Andrea Soltau-Talbot (6-6544)")
Similar presentations


 3 Admission Coordinators.>")






>")










