Download presentation
Presentation is loading. Please wait.

1
Patient Engagement & Decision Support in the Emergency Department Fahd Ahmad, MD, MSCI Pediatric Emergency Medicine Washington University in St. Louis & St. Louis Children’s Hospital

2
The Problem Healthcare providers are slowly being overwhelmed by data Too many patients in given amount of time Increasing volumes of medical research to apply Long and/or complex medical histories Fragmented patient records The ED – all of the above, compounded by not enough data Lack of patient familiarity, lack of time for in-depth discussions Emergent condition the focus but rarely the only problem Pediatrics – some too young to talk, parents not always reliable historians

3
Patient Engagement Having healthcare consumers more aware of and involved in their own care Health IT integral to better patient engagement Most common use now are patient portals Remote access for patients to see their test results Download and review medical records Asynchronous communication with healthcare providers

4
Patient Engagement Patient engagement in the ED requires a different focus Spend less time obtaining information, more time using it Provide immediate details of acute illness Concise summary of medical history Screen for non-emergent but significant health/social issues Real-time decision support within EMR (preferably w/NLP) Improve the doctor-patient/parent relationship and decision making
 Improve the doctor-patient/parent relationship and decision making")
5
Overview Adolescent health screening Emergency Information forms Highlight of other projects (in progress or planning) Herpes Simplex Virus Concussions New initiatives
 Herpes Simplex Virus Concussions New initiatives")
6
Sexually Transmitted Infections Adolescents have highest burden of sexually transmitted infections (STIs) in the United States Chlamydia and gonorrhea two most commonly reported infections in US St. Louis among “leaders” in gonorrhea and chlamydia Cases per 100,000 people Red=St. Louis Blue=Missouri Green=United States

7
STI Screening in the ED Untreated infections with significant morbidities Chronic abdominal pain Ectopic pregnancy Infertility Improved screening and education methods needed Adolescents frequently receive episodic care in the emergency department (ED) Often do not receive preventive/primary care ED visits an opportunity to screen these youth for STIs
 Often do not receive preventive/primary care ED visits an opportunity to screen these youth for STIs")
8
STI Screening in the ED ED environment poses challenges to STI screening: High patient volume Primary complaint often not related to STIs No pre-existing relationship Lack of private space Parent/guardian presence Healthcare providers not familiar with screening guidelines

9
STI Screening in the ED Audio-enhanced Computer-assisted self-interviews (ACASIs) Self-directed electronic questionnaire Completed in private Audio component to aid comprehension Prior studies demonstrate quality of ACASI collected data Adolescents willing to disclose sensitive information via ACASI
 Self-directed electronic questionnaire Completed in private Audio component to aid comprehension Prior studies demonstrate quality of ACASI collected data Adolescents willing to disclose sensitive information via ACASI")
10
STI Screening – Pilot Study Branch-logic questionnaire – sexual history via ACASI Integrated decision tree created testing recommendation Testing recommendation given to patient Patient provides contact information via ACASI Summary of information integrated into EMR ED providers notified via EMR of available information Testing ordered by doctor/nurse if at-risk of infection

11
11

12
12

13
13

14
14

15
ACASI Pilot Results Enrolled 800 patients Median 8 minutes to complete Almost all comfortable with system, prefer electronic format Over 400 patients in need of STI testing, tested 50% of at-risk patients Eighteen percent of those tested positive for chlamydia and/or gonorrhea Most positive tests in those without complaints related to STI 100% of patients notified of positive test, given treatment plans Only one parental complaint

17
Future Directions Rebuild architecture for sustainable use (version 2.0) Evaluate cost-effectiveness of method Expand to include HIV, other sensitive issues, other healthcare locations PECARN – alcohol/drug abuse screening Children’s Hospital of Philadelphia – depression screening Cincinnati Children’s Hospital – suicide screening
 Evaluate cost-effectiveness of method Expand to include HIV, other sensitive issues, other healthcare locations PECARN – alcohol/drug abuse screening Children’s Hospital of Philadelphia – depression screening Cincinnati Children’s Hospital – suicide screening")
18
Emergency Information Forms Children with Special Health Care Needs (CSHCN) Children who have, or at risk for chronic physical, developmental, behavioral, or emotional condition who also require health and related services of a type or amount beyond that required by children generally.” Increased risk for poor outcomes during medical emergencies ED providers often do not have critical aspects of medical histories available CSHCN at-risk for significant complications
 Children who have, or at risk for chronic physical, developmental, behavioral, or emotional condition who also require health and related services of a type or amount beyond that required by children generally. Increased risk for poor outcomes during medical emergencies ED providers often do not have critical aspects of medical histories available CSHCN at-risk for significant complications")
19
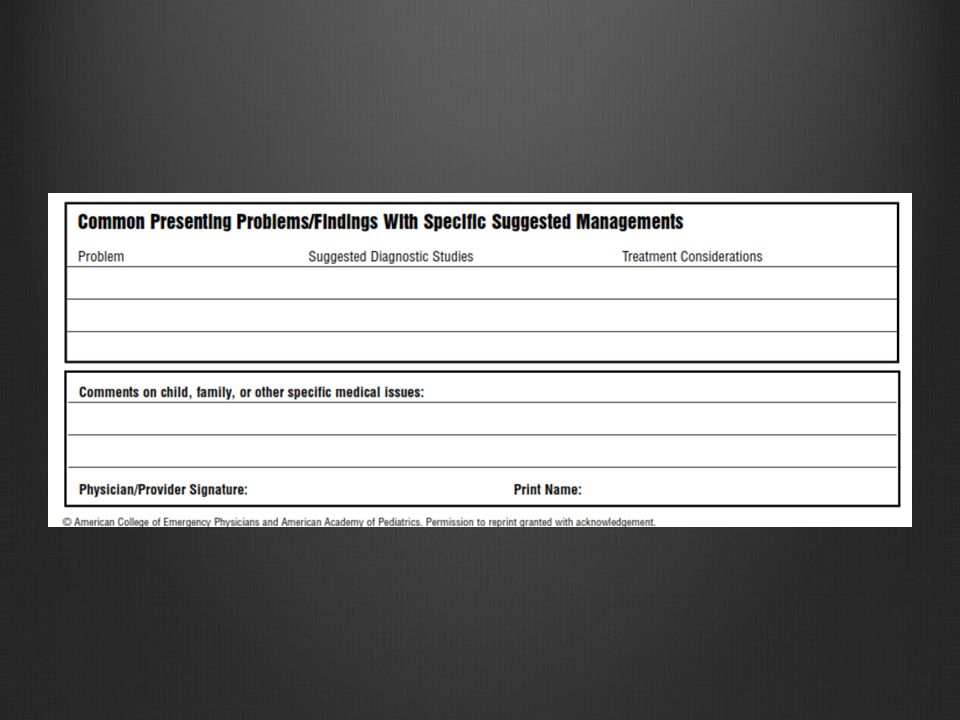
Emergency Information Forms Emergency Information Forms (EIFs) provide essential information in emergencies Summary document for patient’s medical history Major medical/surgical issues What to do (or not to do) in case of specific emergencies Contact information for subspecialists Many barriers prevent widespread adoption Paper easily torn/lost Difficulty maintaining form Has to be available at all times and in any setting Commonly used for metabolic/genetic patients at SLCH
 provide essential information in emergencies Summary document for patient’s medical history Major medical/surgical issues What to do (or not to do) in case of specific emergencies Contact information for subspecialists Many barriers prevent widespread adoption Paper easily torn/lost Difficulty maintaining form Has to be available at all times and in any setting Commonly used for metabolic/genetic patients at SLCH")
20
EIF Template from AAP

25
Google Health

26
Microsoft’s Health Vault

27
Clever countries…. Int J Biomed Comput.Int J Biomed Comput. 1995 Oct;40(2):101-5. Int J Biomed Comput. Australian healthcare: a smart card for a clever country. Morris S Morris S 1, Cooper J, Bomba D, Brankovic L, Miller M, Pacheco F. Cooper JBomba DBrankovic LMiller MPacheco F Morris SCooper JBomba DBrankovic LMiller MPacheco FAbstract In this paper we give an overview of smart card technology how a smart card could be used as a healthcare card and the benefits that would most likely result from doing so. The smart card memory can be zoned into different security levels. The top security zone may contain an individual's full medical history while the lowest security zone may contain the cardholders name and address. Access to the different zones depends on the level of security of the zone. The higher the security level the more restrictive the access method. Were smart cards adopted for the storage of medical histories it would change the form of medical information recorded, not merely convert paper files to electronic ones. Storage of an individual's medical history on a smart card raises important privacy issues. These privacy issues are discussed particularly as they relate to the Australian community. PMID: 8847116 [PubMed - indexed for MEDLINE]
: Int J Biomed Comput. Australian healthcare: a smart card for a clever country. Morris S Morris S 1, Cooper J, Bomba D, Brankovic L, Miller M, Pacheco F. Cooper JBomba DBrankovic LMiller MPacheco F Morris SCooper JBomba DBrankovic LMiller MPacheco FAbstract In this paper we give an overview of smart card technology how a smart card could be used as a healthcare card and the benefits that would most likely result from doing so. The smart card memory can be zoned into different security levels. The top security zone may contain an individual s full medical history while the lowest security zone may contain the cardholders name and address. Access to the different zones depends on the level of security of the zone. The higher the security level the more restrictive the access method. Were smart cards adopted for the storage of medical histories it would change the form of medical information recorded, not merely convert paper files to electronic ones. Storage of an individual s medical history on a smart card raises important privacy issues. These privacy issues are discussed particularly as they relate to the Australian community. PMID: [PubMed - indexed for MEDLINE].")
28
Clever countries…. Int J Biomed Comput.Int J Biomed Comput. 1995 Oct;40(2):101-5. Int J Biomed Comput. Australian healthcare: a smart card for a clever country. Morris S Morris S 1, Cooper J, Bomba D, Brankovic L, Miller M, Pacheco F. Cooper JBomba DBrankovic LMiller MPacheco F Morris SCooper JBomba DBrankovic LMiller MPacheco FAbstract In this paper we give an overview of smart card technology how a smart card could be used as a healthcare card and the benefits that would most likely result from doing so. The smart card memory can be zoned into different security levels. The top security zone may contain an individual's full medical history while the lowest security zone may contain the cardholders name and address. Access to the different zones depends on the level of security of the zone. The higher the security level the more restrictive the access method. Were smart cards adopted for the storage of medical histories it would change the form of medical information recorded, not merely convert paper files to electronic ones. Storage of an individual's medical history on a smart card raises important privacy issues. These privacy issues are discussed particularly as they relate to the Australian community. PMID: 8847116 [PubMed - indexed for MEDLINE]
: Int J Biomed Comput. Australian healthcare: a smart card for a clever country. Morris S Morris S 1, Cooper J, Bomba D, Brankovic L, Miller M, Pacheco F. Cooper JBomba DBrankovic LMiller MPacheco F Morris SCooper JBomba DBrankovic LMiller MPacheco FAbstract In this paper we give an overview of smart card technology how a smart card could be used as a healthcare card and the benefits that would most likely result from doing so. The smart card memory can be zoned into different security levels. The top security zone may contain an individual s full medical history while the lowest security zone may contain the cardholders name and address. Access to the different zones depends on the level of security of the zone. The higher the security level the more restrictive the access method. Were smart cards adopted for the storage of medical histories it would change the form of medical information recorded, not merely convert paper files to electronic ones. Storage of an individual s medical history on a smart card raises important privacy issues. These privacy issues are discussed particularly as they relate to the Australian community. PMID: [PubMed - indexed for MEDLINE].")
29
EIF in the US – What to do next?

30
EIF Qualitative Study Emergency Information Forms for Children with Special Health Care Needs: A Qualitative Study Copper TC, Jeffe DB, Ahmad F, Abraham G, Yu F, Hickey B, Schnadower DS. Objective: to identify facilitators and barriers to optimal emergency care for CSHCN to inform the development of EIFs for CSHCN.

31
EIF Qualitative Study Twenty-six stakeholder interviews: Emergency medicine providers Community pediatricians Subspecialty pediatricians Paramedics Parents of CSHCN Health information technology specialists Privacy compliance experts To learn stakeholders’ preferred content, structure, ownership, and maintenance of an EIF

32
EIF Qualitative Study Barriers Documentation 18/26 ( 11 providers, 4 IT, 3 PC) Poor caregiver understanding 15/26 (10 providers, 1 parent, 3 IT, 1 PC) Poor provider understanding 9/26 (3 providers, 4 parents, 2 IT) Facilitators Summary document 18/26 (12 providers, 4 parents, 2 IT) Provider distrust of summary documents (2 parents)
 Poor caregiver understanding 15/26 (10 providers, 1 parent, 3 IT, 1 PC) Poor provider understanding 9/26 (3 providers, 4 parents, 2 IT) Facilitators Summary document 18/26 (12 providers, 4 parents, 2 IT) Provider distrust of summary documents (2 parents)")
33
EIF Qualitative Study Content Include: Demographics, primary facility, PMH, meds, allergies, baseline exam, advanced directives, general disease info, anticipated emergencies with action plan Exclude: notes, old images/labs, social hx, vaccines, anything irrelevant to chief complaint Interface, Maintenance, and Access Electronic 23/26 – 19 requested web-based with paper/USB Should be created and updated by provider 19/26 Patient owned 13/26

34
EIFs The ideal EIF: Web-based with paper and/or USB copies available at all times, particularly for pre-hospital or out of network emergencies Integrate into EMR and health information exchanges Accessible anywhere, anytime, by appropriate healthcare provider “Owned” by patients, updated by physicians Secure for patient confidentiality

35
EIF Simulation Study Impact of Emergency Information Forms for Children with Special Health Care Needs: A Simulation Study. Abraham GG, Fehr JJ, Ahmad FA, Jeffe DB, White AJ, Yu F, Copper TC, Schnadower D Objective : To measure the impact and utility of EIFs in simulated emergency scenarios of CSHCN.

36
EIF Simulation Study Simulated ED scenarios of critically ill CSHCN Compare provider and patient outcomes with and without an EIF Compare pediatric residents to pediatric emergency medicine fellows and attendings

37
EIF Simulation Study Assessed using checklist of critical actions and time to completion 1Estimates / obtains weight1 point 2* Determines underlying disorder is PA toxicity 2 points 3 Asks to keep patient NPO and stop all G tube feeds. 1 point 4* Asks to access central line port1 point 5 Orders Electrolytes, VBG, Accucheck, UA 1 point 6* Orders Ammonia2 points 7* Orders D10NS fluid bolus2 points 8* Orders IV fluids D10 NS at 1.5 times maintenance 2 points 9* Orders IV Carnitine at 100mg/kg/dose 2 points 10* Orders IV Ammonul (Sodium Phenyacetate + Sodium Benzoate) 250 mg/kg/dose over 90 minutes through the central line 3 points 11* Orders IV Meropenem 20mg/kg2 points Max total16*/19
 250 mg/kg/dose over 90 minutes through the central line 3 points 11* Orders IV Meropenem 20mg/kg2 points Max total16*/19.")
39
EIF Simulation Study Provider performance with and without EIF Scenarios with EIF N=36 Scenarios without EIF N=36 P Median critical action score (IQR) 84.2% (71.7-94.1%)12.5% (10.5-35.3%)P<0.001 Median Time to completion in min (IQR) 6.9 (5.8-10)10 (constant)P<0.001 Presence of complications (95% CI) 30.6% (17.4-46.3%)100% (92.2-100%)p<0.001
 84.2% ( %)12.5% ( %)P<0.001 Median Time to completion in min (IQR) 6.9 (5.8-10)10 (constant)P<0.001 Presence of complications (95% CI) 30.6% ( %)100% ( %)p<0.001")
40
EIF Simulation Study Score by provider type Senior physicians performed as poorly as residents without an EIF When EIF available, two groups performed equally well Junior N=12Senior N=12P With EIF (IQR) 87.5% (80.7-94.1%)81.3% (70.0-94.3%)P=0.406 Without EIF (IQR) 11.5% (6.2-22.9%)20.4% (10.5-41%)P=0.104
 87.5% ( %)81.3% ( %)P=0.406 Without EIF (IQR) 11.5% ( %)20.4% ( %)P=0.104")
41
EIF Next Steps Pilot demonstration project Genetics/Metabolic clinic PCF Interface between a portable device and Health Record Adaptable to Epic and other EHRs Extraction software Health Information Exchanges Transition of care documents

42
Herpes Simplex Virus Rare but serious viral infection Causes significant morbidity and mortality in neonates Significant uncertainty in which ill neonates require testing Hospital guideline developed to provide guidance EMR prompts when ordering HSV specific tests or meds ED Testing decreased by 90% in low-risk patients No missed HSV diagnoses

43
Concussions A mild traumatic brain injury caused by biomechanical forces Regional and temporal cellular dysfunction that can include cell death Disturbance in brain function that is generally time-limited Does not result in structural changes observable on CT or MRI Clinical diagnosis – no imaging or lab tests required

44
Concussion Symptomatology Most common symptom of pediatric concussion is headache Symptoms are most severe in the first 3 days but improve and resolve over 2 weeks 20-30% of children will have prolonged symptoms > 2 weeks that effect their quality of life 250,000+ pediatric ED visits per year for concussion Return to activity for most based based on symptom tracking

45
Adapted from: M.R. Lovell, M.W. Collins, K. Podell, J. Powell, J. Maroon ImPACT: Immediate post-concussion assessment and cognitive testing NeuroHealth Systems, LLC, Pittsburgh, PA (2000)
.")
46
New Initiatives Abdominal pain Gun violence/trauma

47
Apple ResearchKit

Similar presentations