Download presentation
Presentation is loading. Please wait.

1
Vaccine Adverse Events and Risk Communication In Vaccination Najwa Khuri-Bulos MD,FIDSA Jordan University Hospital Amman, Jordan

2
explaining properly the benefits and risks of a recommended vaccine; addressing public concerns and upcoming or persistent rumours about vaccine safety; preparing to address vaccine safety crises if and when they occur.

3
The recommended criteria fall into four categories: Essential criteria (i.e. with respect to credibility) Essential criteria (i.e. with respect to credibility) Important criteria (i.e. with respect to content) Important criteria (i.e. with respect to content) Practical criteria (i.e. with respect to accessibility) Practical criteria (i.e. with respect to accessibility) Desired criteria (i.e with respect to design) Desired criteria (i.e with respect to design)
 Essential criteria (i.e. with respect to credibility) Important criteria (i.e. with respect to content) Important criteria (i.e. with respect to content) Practical criteria (i.e. with respect to accessibility) Practical criteria (i.e. with respect to accessibility) Desired criteria (i.e with respect to design) Desired criteria (i.e with respect to design).")
4
VACCINE ADVERSE EVENTS AND RISK COMMUNICATION IN VACCINATION Najwa Khuri-Bulos Jordan University Hospital

5
Jenner

6
STRONG TOOLS AVAILABLE/EXPECTED

7
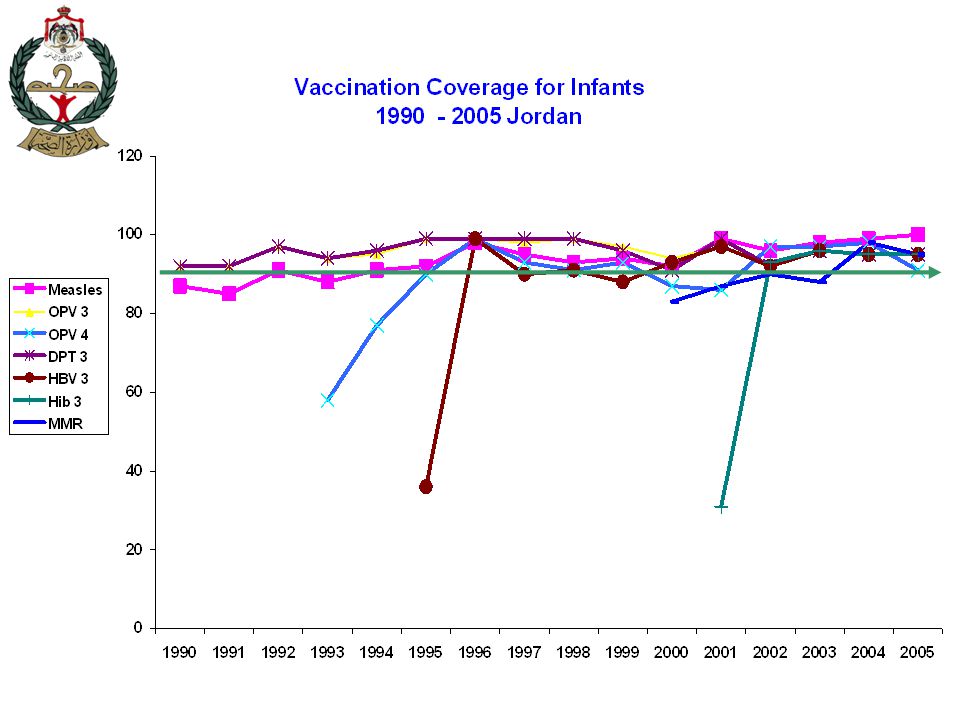
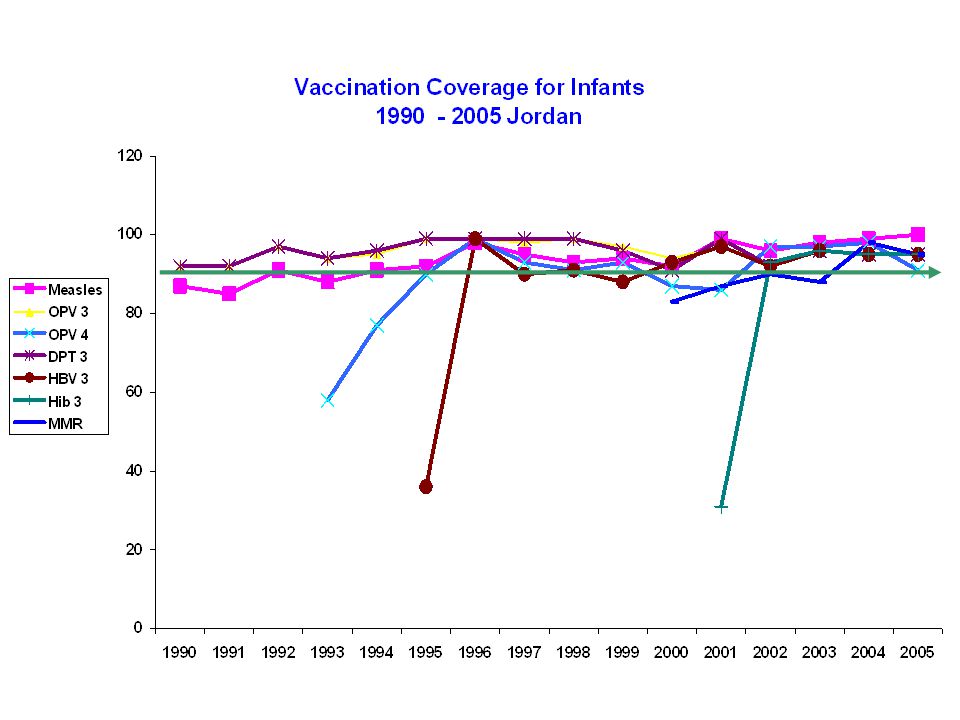
Measles poliomyelitis Impact of the EPI Case Study, Jordan, a great success story Diphtheria

8
Diphtheria 175,8854 -99.99 Measles 503,28281-99.98 Mumps 152,209 323-99.79 Pertussis 147,271 6,755-95.41 Polio (wild) 16,3160 -100 Rubella 47,745 152-99.68 Cong. Rubella Synd.823 7-99.15 Tetanus 1,314 26-98.02 Invasive Hib Disease 20,000 167-99.16 Disease 20 th Century Annual Morbidity* 2000** % change * Maximum cases reported in pre-vaccine era and year + Estimated because no national reporting existed in the prevaccine era ^ Adverse events after vaccines against diseases shown on Table = 5,296 ** Provisional Total 1,064,8457,515-99.29 Vaccine Adverse Events 0 13,497^ +++ Comparison of Annual and Current Reported Morbidity, Vaccine-Preventable Diseases and Vaccine Adverse Events, United States

9
Vaccines don’t prevent disease Vaccination prevents disease

10
Evolution of Immunization Program and Prominence of Vaccine Safety Concerns

11
Trust “It takes many good deeds to build a reputation, and only one bad one to lose it” Benjamin Fran klin “It is far easier to build trust before it is needed”. WHO

12
Trust and how to build it Transparency and Key points on vaccine adverse events 1. There is no such thing as a “perfect” vaccine 2. effective vaccines may produce some undesirable effect which are mostly mild 3. The majority of events thought to be related to administration of a vaccine are actually not related to it 4. It is not possible to predict every individual who might have a mild or serious reaction

13
Trust and how to build it Evidence based support from international organizations Transparency in vaccine licensing and clarity of why recommendations are made Transparency on collaboration and conflict of interest For that to happen must establish relations with stakeholders before one needs it

15
Requirements for Successful vaccination on a wide scale Trust is at the core of the relationship between the patient and the health system which Recommends Procures Stores Transports Administers And conducts surveillance for vaccine use, impact and adverse events Disruption in any of the above shakes that trust

16
But still vaccination, while the best health intervention may carry some small risk for adverse event following immunization (AEFI) Some of these may be due to the vaccine itself, but many if not most are coincidental and have no relationship to the vaccine itself Must distinguish between vaccine adverse effects and vaccine adverse events
 Some of these may be due to the vaccine itself, but many if not most are coincidental and have no relationship to the vaccine itself Must distinguish between vaccine adverse effects and vaccine adverse events")
17
Vaccine hesitancy and refusal While anti vaccine sentiment is not new, and did occur even in the nineteenth century, the ease with which information is globalized via the internet, social media, television, radio and other means makes it mandatory that practitioners who are convinced of the value of vaccination to be prepared to advocate fully on behalf of vaccines.

19
History of some adverse effects in the 20 th century Vaccine effects are related biologically to vaccines. These are rare Kyoto disaster 1948 Japan Diptheria vaccine incompletely inactivated 68/606 died Cutter incident 1955 USA Administration of polio vaccine which was not completely inactivated caused paralysis

20
Examples of Vaccine adverse events Vaccine adverse events may be coincidental and not necessarily related to the vaccines DTP and encephalopathy UK in mid 1970s Tetanus and sterility in Filipinas 1994 MMR and autism 1998 Polio and sterility in Nigeria in 2001 None of these was proved to be due to vaccines but all led to major disruption of immunization on a wide scale and disrupted public health with increased attack rates

21
Diseases reappear when coverage drops

22
EPI, case study Jordan 1979, EPI started with DTP,OPV,BCG 1982 Measles 1995 HBV 2000 MMR 2001 HIB 2005 IPV Uptake more than 85% for all vaccines In private sector, a different agenda MMR since 1990, HIB since 1993, Pneumo, Rota,Hep A and VZV since 2006

23
Vaccination schedule Jordan 2007 agevaccine 1 st contact 2 months 3 months 4 months 9 months 18 Months BCG DTP + HepB 1 +Hib 1 + IPV DTP+HepB 2 +Hib 2 + OPV +IPV DTP+HepB 3 +Hib 3 + OPV measles + OPV MMR +DTP booster1 +OPV booster1

25
Examples of Vaccine adverse events in a developing country, Jordan Td mass vaccination in schools 1998 The polio immunization days and parents concern in 2000 The MMR and the politics of the EPI 2012

26
1 st Experience * Mass psychogenic illness following tetanus-diphtheria toxoid vaccination * A total of 25,667 Td doses given through school immunization for 1st and 10 th grades, using Td vaccine More than 800 students reported AEFI Out of them 122 hospitalized Discharged within 48 hours * Source: Bulletin of the WHO, 2001, 79 (8)
")
27
Number of Td doses administered per day, 7 - 29 September 1998 September 1998 Total doses administered 25,667 Up to 27 Sept. 19,578 doses were administered with NO report of adverse event s Source: Bulletin of the WHO, Clemens, Kharabsheh S, Jarour, Khuri-Bulos et al 2001, 79 (8)
.")
28
Life Cycle of a Vaccine Safety Concern Case report Standard assessment Case series Plausibility Alternative hypothesis + (Communications) Controlled studies Communications Pathophysiology Risk factors Risk/benefit policy Societal Individual Treatment Compensation Safer vaccine Appropriate C/I Screening
 Controlled studies Communications Pathophysiology Risk factors Risk/benefit policy Societal Individual Treatment Compensation Safer vaccine Appropriate C/I Screening")
29
MOH Response Ask for expert help from national and international agencies Stop school vaccination (Td )vaccination Comprehensive case investigation and crisis control Case definition Standard form Vaccine samples sent for testing to reference laboratories Press releases Respond to Parliament inquires & questions Investigation by Independent team
vaccination Comprehensive case investigation and crisis control Case definition Standard form Vaccine samples sent for testing to reference laboratories Press releases Respond to Parliament inquires & questions Investigation by Independent team")
30
Cause of the Td AEFI The cause of the outbreak Clustering of the adverse events was due to the fact that a large number of Td doses was given over a short period of time rather than an increased attack rate * Source: Bulletin of the WHO, 2001, 79 (8)
")
31
Action taken to restore public confidence Media Plan was developed in the beginning of 1999 For re-launch of the Td immunization to be disseminated by varied media, TV, radio and newspapers Adoption of a more proactive media policy to foster partnership with media A series of Seminars were conducted to educate the media about EPI Training of the EPI manager in communication skills

32
Lesson Learned Public must be assured that the team is knowledgeable and has expertise. Ask for help if need be Openness and honesty The communicator must be trustworthy Concern and care to the cases must be provided. All cases were hospitalized at no expense at MOH hospitals

34
Threat to Polio vaccine 1999

35
140 120 100 80 60 40 20 0 19781979198019811982198319841985198819891990199119921993 Years No. of Cases POLIOMYELITIS IN JORDAN 1978-2001 19942001 1978 data added by Khuri-Bulos. Melnick and Hatch (bull WHO 1984) EPI started Outbreak
 EPI started Outbreak.")
36
Vaccine policy changed in 1995 following outbreak NIDs + routine vaccination starting 1995 2 OPV mass vaccination yearly for all children <5 years of age (15 OPV doses by age 5 yrs of age) National Certification Committee (NCC) to monitor coverage and disease (AFP) 1996 Performance was above 90% till 1999 NCC chairman was informed of vaccine refusal for the NID dose in some centers
 National Certification Committee (NCC) to monitor coverage and disease (AFP) 1996 Performance was above 90% till 1999 NCC chairman was informed of vaccine refusal for the NID dose in some centers")
37
Response Assemble the National expert group Identify reason for drop in immunization coverage Advise on what to do and implement soonest Budget was set aside for this by MOH

38
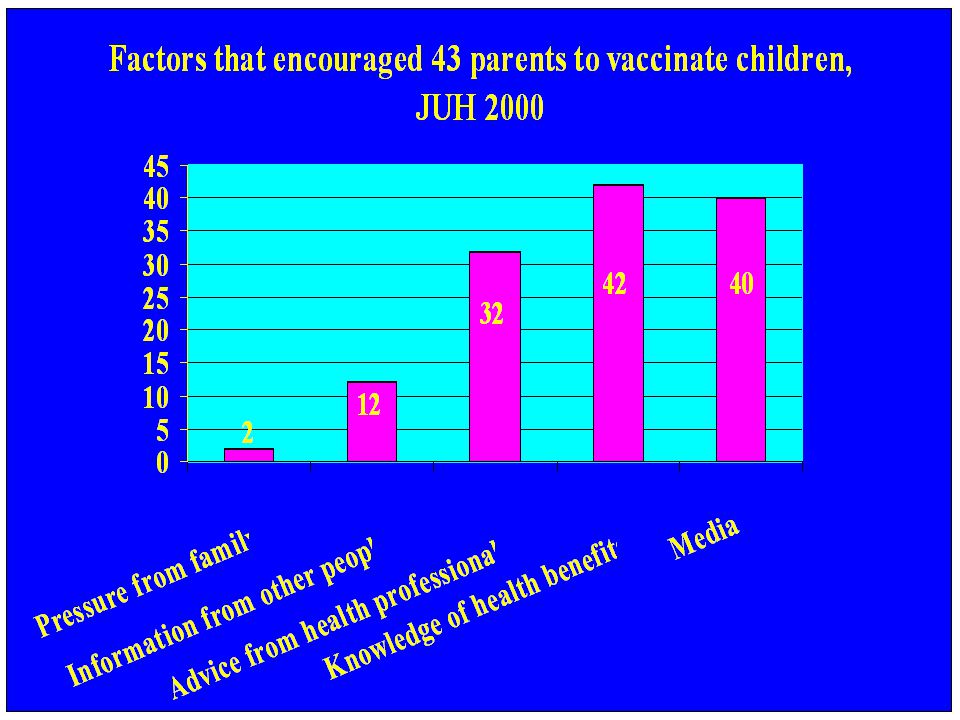
Identify reason for decreased coverage.. Ask the public Rapidly set up pilot survey at the JUH over a three week period between April 9-27, 2000, Convenience sample used 43 Parents (mothers) of children who are hospitalized at the JUH pediatric ward interviewed by the same interviewer Immunization card reviewed Open and closed questions on Vaccine and provider used Knowledge of side effects Knowledge of dangers Source of information on benefits to use vaccines Source of information on vaccine dangers Most trusted source of information when in doubt
 of children who are hospitalized at the JUH pediatric ward interviewed by the same interviewer Immunization card reviewed Open and closed questions on Vaccine and provider used Knowledge of side effects Knowledge of dangers Source of information on benefits to use vaccines Source of information on vaccine dangers Most trusted source of information when in doubt.")
40
Health Facilities used in Vaccination

44
Sterility Growth Retardation Mental Retardation Spoilt/contaminated/expi red Dangers of vaccines perceived by 43 Parents JUH 2000

45
Vaccine and Dangers Vaccine most implicated: OPV OPV was the only one implicated in sterility 6 of those who thought sterilitywas a danger refused OPV in the NID

46
Trusted Sources of information by 43 Parents, JUH 2000 Pediatrician31 Nurse 3 Other health professional 1 Own knowledge 1 Television 2 Books 1 Note that the internet and social media did not exist on a wide scale at that time

47
Action taken Media campaign started immediately using TV, Radio and newspapers reminding the public about the dangers of polio Media campaign continued for several months Media campaign included medical community with lecture tours by the committee members to Medical associations and lay public Coordination with the whole EPI team was done in order to prevent similar problem with other vaccines

48
Rumor reporte d Rumor

49
Lessons learned Must pay attention to vaccine rumors before they get “out of hand” Must have political support and help and budget for these activities Independent team with the NCC was able to help the EPI Must be attentive to local concerns

50
The MMR and Sterility!! 2012 Political Payback

51
MMR ( Chiron) withdrawal 2005 121309 students vaccinated with MMR Chiron AEFI Investigation of the AEFI reported 20 mumps like illness 2 mild skin allergy One anaphylaxis Response Stop vaccination Immunization committee meeting & press release Active surveillance for any AEFI Communication Discard unused vaccine (but it was already paid for)
 withdrawal students vaccinated with MMR Chiron AEFI Investigation of the AEFI reported 20 mumps like illness 2 mild skin allergy One anaphylaxis Response Stop vaccination Immunization committee meeting & press release Active surveillance for any AEFI Communication Discard unused vaccine (but it was already paid for)")
52
Political payback and the charges of corruption In 2012, parliament review of government actions in 2005 for corruption charges. TV appearance by member of parliament, head of the health committee accusing the previous government in 2005 of negligence and corruption by obtaining vaccines that render children sterile naming the MMR Government accused for profiteering from a “poorly” made cheaper vaccine

53
Response Jordan NITAG Chairman and the Head of the Primary health care requested immediate media TV coverage time to answer the charge WHO GACVS e mail query if there were any other similar global claims, answer received in time for TV appearance E mail and other scientific evidence discussed on live TV with MOP and relationship of sterility to MUMPS disease explained but not MMR. Offer made for willingness to appear in front of the committee. No invitation made and no more media complaint MMR uptake remained unchanged

54
Lessons learned Must respond immediately to political pressure Increase credibility by obtaining support from international organizations Keep all lines of communication open since political instability may hurt well established programs The whole public, politicians included must be made aware of the great benefit of this program and maintain its integrity in the interest of their own families children in addition to those of the public

55
Conclusions Public trust is fragile and is necessary for vaccination programs Vaccine adverse events even if not related to vaccines and not scientifically sound can disrupt programs Communication strategy should include educating the parents and the public about the DISEASES prevented and the vaccines Prompt action is needed due to the increased use of the internet and social media in developing countries Above all maintain credibility and choose a trusted messenger The pediatrician is ideally suited to play a central role.

56
Risk communication strategy Be sensitive Be sincere Be credible and knowledgeable Be prepared

57
Thank youThank you

Similar presentations




















 introduction.>")



