Download presentation
Presentation is loading. Please wait.

1
Section 11 Radiation Therapy Clinical Treatment Management
Covered by pages 1-49 Section 11 Radiation Therapy Clinical Treatment Management Carl Bogardus, Jr, MD 10:15 -10:45 AM 031114 Modified For 83

2
TOTAL CARE OF THE RADIATION ONCOLOGY PATIENT CLINICAL TREATMENT MANAGEMENT
1 The total care of the radiation oncology patient mandates direct clinical management by the radiation oncologist throughout the course of therapy. It is the radiation oncologist’s role and responsibility to provide daily supervision of treatment and hands-on, face-to-face patient care.

3
Clinical Treatment Management
2 Clinical Treatment Management starts with the acceptance of the patient for treatment. Clinical Treatment Management ends with the Clinical End of Treatment report. Clinical Treatment Management is tied to 5 days of treatment delivery only as a convenient means of tracking time for billing purposes.

4
CPT Radiation Therapy Treatment Management Codes
4 CPT Radiation Therapy Treatment Management Codes Weekly Radiation Therapy Management, fractions Radiation Therapy Management; Short course, 1 or 2 fractions Radiation Therapy Management; Stereotactic, (SRS) 1 fraction 77435 – Radiation Therapy Management; SBRT, SRS, full course of therapy, up to a max of 5 fractions, (2007) Radiation Therapy Management; Intraoperative.
 1 fraction – Radiation Therapy Management; SBRT, SRS, full course of therapy, up to a max of 5 fractions, (2007) Radiation Therapy Management; Intraoperative.")
5
Professional billing 77427 4 Professional billing relates to 5 fractions of therapy delivered, regardless of the number of elapsed calendar days and must be billed as X 1 per 5 FX block of treatments. The billing date for weekly management , 77427, is usually the first day of each of the 5 day blocks.

6
Most of the Carriers want you to report this way
NIB Most of the Carriers want you to report this way 5 fractions equal one Week, bill first date of week

7
Historical Background
7 It is imperative that each physician document their direct involvement in all of the procedures related to a week of treatment management. It is expected that each patient will have as many regularly spaced progress notes as there are weeks of treatments. The complexity and completeness of the note must reflect the complexity of care for the patient.

8
WEEKLY UNDER BEAM PROGRESS NOTES Five Required Review Elements
7 WEEKLY UNDER BEAM PROGRESS NOTES Five Required Review Elements The physician will be expected to have reviewed as many of these elements as are applicable to the current course of treatment management It is extremely important that these five critical elements be covered in each note. I Chart and dosimetry review II Treatment setup and delivery review III Port film or electronic image review IV Under beam evaluation of the patient V Recommendation of therapy

9
8 The weekly progress note does not necessarily have to occur on the same day of each week, but for a course of therapy there should be an equal or greater number of progress notes than the weeks of management being billed.

10
A weekly note must occur sometime during each 5 day interval
9 Mon Tues Wed Thurs Fri Week TX TX TX TX TX NO PROGRESS NOTE WEEK 1 This causes problems with 77427 Week TX TX TX TX TX PN 77427 Week TX TX TX TX TX PN Week TX TX TX TX TX PN A weekly note must occur sometime during each 5 day interval

11
A weekly note must occur sometime during each 5 day interval
9 Mon Tues Wed Thurs Fri Week TX TX TX TX TX PN Having a note on week 1 is crucial 77427 Week TX TX TX TX TX PN Week TX TX TX TX TX PN Week TX TX TX TX TX PN Having a note on the last TX date is very important PN 77427 EOT A weekly note must occur sometime during each 5 day interval

12
WEEKLY PROGRESS NOTE 9 There is no written directive stating which day during the treatment week that the physician/patient encounter must occur. There is no stipulation of the manner of interaction, only that it be “face to face”

13
Which is a valid location for patient/physician encounter?
9 Parking garage Hall way Waiting room Exam room Treatment console Treatment room Which is a valid location for patient/physician encounter?

14
10 ALL OF THEM At each encounter this patient had the opportunity ask question related to her course of treatment. At each encounter the patient acknowledges her interaction with the physician. At each encounter the physician has the opportunity to evaluate the patient’s general condition. At each encounter the physician will use his best judgment to determine what is needed to evaluate response to treatment and radiation reactions There is no written requirement related to length of time or location of the patient/physician encounter As long as privacy concerns are met to the satisfaction of both the physician and the patient. 20/104

15
WEEKLY PROGRESS NOTE 10 The patient /physician encounter is only one of the 5 required elements of weekly management The weekly progress note is a document covering all aspects of patient care and management. Each of the 5 basic elements is further subdivided into many sub routines that require individual documentation

16
10 WEEKLY PROGRESS NOTE The production of this supporting document does not need to coincide with the physical examination of the patient. It is customary done this way only as a general convenience, not a requirement

17
UNDER BEAM PROGRESS NOTES
NIB Narrative on page 6 INITIAL EVALUATION DOSIMETRY TREATMENT IMAGING EXAMINATION UNDER BEAM PROGRESS NOTES CLINICAL END OF TREATMENT SUMMARY The under beam progress note is a clinical weekly summary documenting the physician’s involvement in the weekly management of the patient FOLLOW UP NOTES Using the cascading Information format, vital clinical and technical data may be transferred, discarded, or added to each new weekly document as it is created

18
Compliance and audits. These are two words that most physicians and administrators really don't like to hear. With cascading, elements of an E/M document will copy verbatim into subsequent documents. Verbatim copying will cause cascading of old information into new encounter forms without any change. Medicare considers that an identically copied note indicates that the physician was not actively involved in the creation of the new note. Templating has HCFA considering severe penalties when they find large sections of notes that are 100% copies in subsequent workups. NIB

19
Medical decision-making Other areas may also change.
NIB All physicians and users should be very much aware of this potential problem. They are well advised to carefully read any areas of their notes that are likely to change such as; Chief Complaint, HPI, Physical Exam Review of Systems Medical decision-making Other areas may also change. Do not always use exactly the same time for every patient or type of encounter.

20
Compliance Warning, Cascaded Information
NIB Compliance Warning, Cascaded Information

21
NIB Original work up Six week follow-up

22
EMRs make compliance very easy, but they also make auditing very easy.
All that is really required is a quick review of the areas of a document where you know some changes have probably occurred based upon the patient's clinical findings and treatment parameters. Document those changes in the record. If no changes have occurred, indicate that you have reviewed that section and it is truly unchanged from the previous work up. EMRs make compliance very easy, but they also make auditing very easy. NIB

23
We Recommend NIB Any cascaded topic that has not been reviewed on a new document will clear upon save and record. If the topic has been opened and any change has been made, then the changed topic and its questions and answers will be saved. You may indicate “reviewed and save, no change needed”.

24
# 1--Chart & Dosimetry Review
15 Verification of correct summation of dose Verify that time and/or monitor units are correct. Stop or re-evaluation points are clearly indicated. The correct modalities of treatment are indicated. The correct beam energy is indicated. Proper beam modifiers are in place. Tumor dose is compared to the tolerance dose of critical tissues. Critical tissue dose points are carried The number of treatment volumes is correct. The number of ports is correct. Document of the first day of treatment with the first under beam note

25
#2 Treatment Setup & Positioning Evaluation
15 #2 Treatment Setup & Positioning Evaluation It is understood that it is impossible for the physician to be physically present during each and every setup, but the physician should be readily available for corrective action should the need arise. Document of the first day of treatment with the first under beam note

26
# 3--Portal Film Review for Imaging
16 # 3--Portal Film Review for Imaging Radiographic films or electronic or portal imaging studies are taken at regular intervals of all of the portals being treated. Port film review must be documented each week in the under beam progress note, if imaging is performed.

27
# 4--UNDER BEAM EVALUATION PROGRESS NOTE
16 # 4--UNDER BEAM EVALUATION PROGRESS NOTE Examination of the patient consists of clinical evaluation, assessment of tumor response, and case management. The radiation oncologist should physically examine the patient each week for treatment related side effects, and tumor response.

28
Under Beam Examination
17 Under Beam Examination - Every patient under treatment, without exception, should be seen and examined at least once per week by the physician. This is a key element of the weekly note. The PA can do much of the work, but the physician must be involved

29
17 For under beam visits, these components are the same as for other E/M services. E/M services are included in weekly management and cannot be charged separate. 44/104

30
17 Many factors make up a weekly progress note, the use of multiple choice questions with many choices of answers, makes each note unique and reduces the appearance of “macro copying”

31
NIB Pages 17 to 20 give a short summary of the needed elements to make up a compliant progress note. You should follow these guide lines to format the content of your notes.

32
UNDER BEAM PROGRESS NOTE
21 UNDER BEAM PROGRESS NOTE Every progress note should have the basic demographic information about the patient.

33
History of Present Illness
21 History of Present Illness A very short version of the patient's present illness should be presented limited to only a few sentences summarizing the case to-date.

34
Current Treatment Parameters
22 Current Treatment Parameters Area(s) under treatment Energy/mode Evaluation of appropriateness and accuracy of all Treatment Devices Current dosage Planned dosage Critical structure dosage Microdosimetry as done Any corrective action as required
 under treatment. Energy/mode. Evaluation of appropriateness and accuracy of all Treatment Devices. Current dosage. Planned dosage. Critical structure dosage. Microdosimetry as done. Any corrective action as required.")
35
A weekly review of technical factors is required, once entered, this component usually will not vary week to week, if any factors change, then the note must reflect the changes 22

36
Physical Examination 23 Constitutional General appearance
Examination of area under treatment must always be included Examination of other areas as needed

37
24 Current Status of any Treatment Reactions Skin reactions GI reactions Oral cavity reactions Hematologic profile Present weight as related to previous weight

38
Tumor Response 24 Indicate any changes from previous work-up
Significant or subtle changes in tumor size Expected response at current dose level

39
Pain Assessment and Management
See Section 3 Page 8 Full assessment of pain Medications and corrective actions Order and document medications Print prescriptions Maintain a compliant list of all medications and prescriptions. ONCOCHART

40
#5 Recommendation of Treatment
25 #5 Recommendation of Treatment Patient to continue therapy Patient placed on hold – state the reason Treatment requires modification Patient has completed the course of treatment THIS MUST BE COMPLETED BY THE PHYSICIAN EACH WEEK, NO OTHER PERSON CAN MAKE THIS DECISION.

41
Physician orders (CPO)
25 With electronic records, Clinical Physician Orders have been made much easier to deal with. Multiple paper forms are eliminated Orders can be tailored to fit the case Orders can be sent electronically

42
25 Physician work page has all the common procedures that require orders. This can be initiated by any authorized person in the department A narrative is produced which can be sent electronically, faxed, or printed THIS IS A MEANINGFUL USE REQUIREMENT ONCOCHART

43
Drug Orders in Dept. Electronic record of physician order for medication dispensed by nursing staff and signed off by physician. Compliant with JCAHO and Meaningful Use.

44
Clinical comment regarding Current Status
26 Clinical comment regarding Current Status This is a brief narrative summary of a review of any of the preceding elements that show significant change, or new developments of importance to the care of the patient. ONCOCHART

45
Coordination of Care 26 Routine progress notes should be sent to the patient’s other physicians to keep them informed of the case under treatment. 60/104

46
Physician Demographics
26 Physician Demographics Every progress note should conclude with a signature of the physician of record and indication of copies to other physicians or charts. Electronic signature is acceptable if original signature is on file.

47
27 Check-off and fill-in weekly summaries are marginally acceptable, but they must be legible and complete. They must show that the physician has documented his/her direct involvement in the production of the weekly assessment.

48
NIB THIS NOTE DOES NOT MEET MEANINGFUL USE, WHICH IS NOW REQUIRED This check off note just barely will suffice as a valid progress note. Demographics, vitals, dose, and some recommendation of therapy are noted, but the rest is almost unintelligible, and far too brief, with many key elements missing, such as a legible signature and physician name.

49
NIB This weekly under beam note is also marginal in terms of useful data, and does not meet compliance requirements.

50
Electronically Generated Progress Notes are Preferable
NIB NIB Electronically Generated Progress Notes are Preferable

51
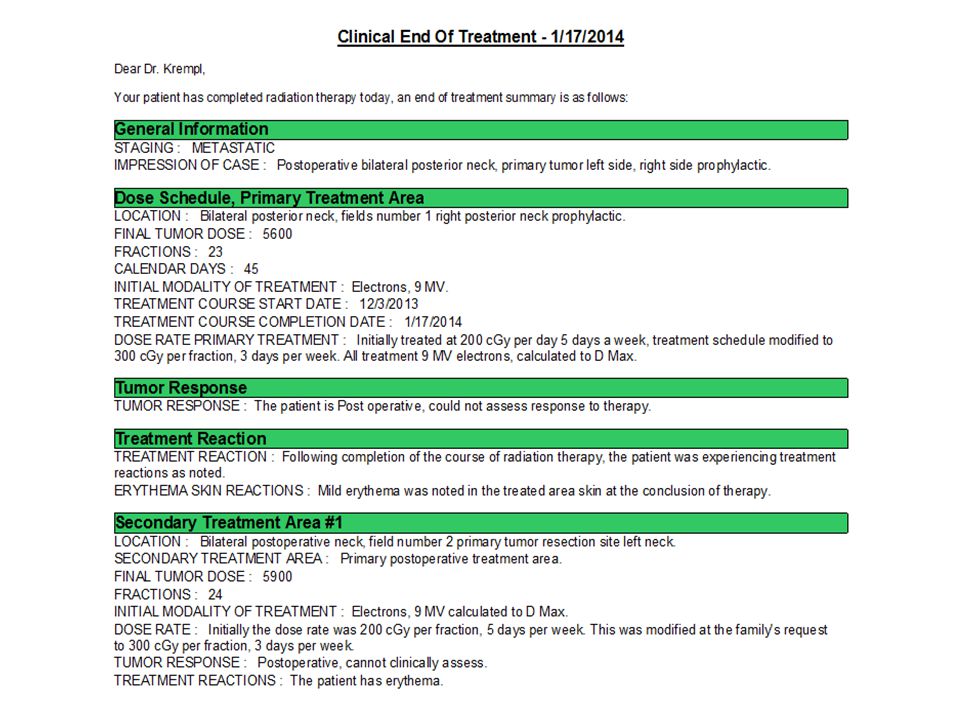
Clinical end of treatment summary.
The clinical end of treatment summary is a non reimbursable procedure, but is absolutely necessary to indicate the termination of the course of radiation treatment. This document should contain sufficient information to allow the requesting physician, or any other physician involved in the care of the case to fully understand the course of treatment that was just completed.

53
Transition of care If you are attesting for meaningful use a transition of care record is required, but it is also very good clinical practice. The transition of care record, combined with an end of treatment summary allows you to transfer a great deal of meaningful information to the referring physician for their continued care of the patient.

54
Transition of Care Document

55
Weekly Treatment Management 77427
What’s it for? The physician’s ongoing clinical care during a course of therapy. Who normally documents/bills/captures this code? The physician. What Documentation is suggested for this code? A weekly progress note (every 5 fractions) by the physician What are the common documentation errors with this code? Inadequate amount of information in the weekly notes. Missing progress notes for the given number of fractions. What are the common billing errors identified? Billing this code based only on the number of fractions without adequate documentation (progress notes) existing in the record. BID therapy requires a progress note every 5 fractions (2 ½ calendar days)
 by the physician. What are the common documentation errors with this code Inadequate amount of information in the weekly notes. Missing progress notes for the given number of fractions. What are the common billing errors identified Billing this code based only on the number of fractions without adequate documentation (progress notes) existing in the record. BID therapy requires a progress note every 5 fractions (2 ½ calendar days)")
56
28 FIBEROPTIC ENDOSCOPY PROCEDURE CPT 31575

57
Typical format of endoscopy report
29 Typical format of endoscopy report FIBEROPTIC ENDOSCOPY This patient is currently being treated for a T1, N0, M0, squamous cell carcinoma of the right true vocal cord. The patient has just completed his third week of radiation therapy. He is currently being treated at 180 cGy per day and is currently at 2700 cGy Procedure: Utilizing a premedication of Pontocaine and Epinephrine applied through nasal atomizer into the right nares, the fiberoptic endoscope was inserted without difficulty. The nasal vestibule and nasal passages were carefully evaluated and found to be unchanged from the previous examination of two weeks ago. The endoscope was advanced further and the nasopharynx was clearly visualized. Both eustachian orifices were clear. A mild amount of dried secretion was noted along the posterior pharyngeal wall. None of this appears to be significant. There is a mild injection of the mucosa of the nasopharynx but no abnormalities were noted. The endoscope was then advanced further and the hypopharynx and base of the tongue area were carefully evaluated and found to be unchanged from previous evaluations. The endoscope was then advanced into the region of the larynx. The epiglottis was noted to be symmetrical and without lesions. A moderate amount of mucositis is beginning to develop in the area of the larynx. This is most noticeable along the base of the epiglottis. Laryngeal ventricles are completely within normal limits. Pyriform sinuses are within normal limits. The false cords are beginning to show a very light edema. There is a moderate amount of mucositis throughout the perilaryngeal area. The vocal cords move well and oppose midline. The lesion that was previously noted along the anterior aspect of the right cord is beginning to decrease in size. There is a white membrane that has formed along the area of the right anterior cord primarily in the region of the tumor. There is no membrane formation on the left cord. The procedure was terminated without difficulty. Impression: Expected response at three weeks of therapy with beginning resolution of tumor. Recommendation: The patient will continue on the planed course of radiation therapy without modification. C.R. Bogardus, Jr., M.D./nz MAY BE REPORTED DURING AN ACTIVE COURSE OF TREATMENT ONCOCHART

58
77417 Therapeutic radiology port Film(s)
30 77417 Therapeutic radiology port Film(s) Port films are taken on the treatment machine using the treatment beam to ensure that the treatment setup is as prescribed by the simulation and dosimetry. Any changes indicated by the port films must be corrected or incorporated into the treatment plan. For coding purposes, real-time or on-line portal imaging is the same as obtaining port films. The technical component (i.e. the costs associated with generating port films) is reportable using code 70/104
 Port films are taken on the treatment machine using the treatment beam to ensure that the treatment setup is as prescribed by the simulation and dosimetry. Any changes indicated by the port films must be corrected or incorporated into the treatment plan. For coding purposes, real-time or on-line portal imaging is the same as obtaining port films. The technical component (i.e. the costs associated with generating port films) is reportable using code /104.")
59
Conformal Treatment Management
34 Conformal Treatment Management Conformal radiation therapy treatment management (3-D designed) consists of clinical management of custom designed and blocked treatment portals, directed to a treatment volume of interest. 3-D Conformal management (not SRS, or SBRT) is to be reported using code 77427
 consists of clinical management of custom designed and blocked treatment portals, directed to a treatment volume of interest. 3-D Conformal management (not SRS, or SBRT) is to be reported using code")
60
77469 Intraoperative treatment management, single session
34 This code is to be utilized when only 1 fraction makes up the entire course of treatment management. All management codes are mutually exclusive per course of therapy

61
35 Short Course of Clinical Treatment Management This code is to be utilized when only 1 or 2 fractions make up the entire course of treatment management. Note: This code may not be used to be reimbursed for the remaining one or two treatments at the end of a long course of therapy (ACR, 2001). 77/104
. 77/104.")
62
Prevention of Heterotrophic Bone formation
36 Most commonly done following major bone trauma Single treatment of 6 to 8 Gy All procedures done on one day. Consult, treatment planning, simulation, blocks, dosimetry, and treatment ICD-9 code or V-07.8

63
HETROTROPHIC BONE PREVENTION
36 HETROTROPHIC BONE PREVENTION POST OPERATIVE

64
Short Course of Clinical Treatment Management 77431
39 Short Course of Clinical Treatment Management 77431 What is this code for? The physician’s clinical care during a short course of only 1 or 2 fractions. Who normally documents this code? The physician. When is this code normally billed? The last day of the short course. What Documentation is needed for this code? A progress note outlining the short course of therapy. What are the common documentation errors identified with this code? No physician’s note being documented. What are the common billing errors identified? Billing this code with Brachytherapy, this is only for external beam patients. Do not report for 1 or 2 leftover fractions of at the end of a long course of therapy.

65
Chemotherapy with Radiation Treatments
41 Chemotherapy with Radiation Treatments 85/104

66
Chemotherapy with Radiation Treatments
41 Chemotherapy with Radiation Treatments Chemotherapy, or the use of drugs to treat cancer, is a concept that has been with us for over 40 years. In the beginning, the drugs were extremely toxic, and relatively ineffective. New drugs have been perfected which are highly disease selective. There are many drugs in use today that target specific cell lines of malignancy. Some of these drugs are used alone, others are used in combination, and others are used in conjunction with radiation therapy.

67
41 Almost all of the chemotherapeutic agents are highly toxic and create various medical problems for the patient in addition to their beneficial effects against the malignancy. The beneficial effects of these drugs usually will out weigh the toxic side effects, and for this reason chemotherapy plays a very important role in the overall management scheme of patients with malignancy.

68
41 When chemotherapy is used, the acute and long-term effects, must be taken into account by the radiation oncologist. Patients receiving chemotherapy tend to be sicker and require closer and more careful attention The treatment planning and treatment management of the course of therapy will always be complex. This will be true even in what otherwise, would have been a simple case. 88/104

69
Special Treatment Procedure 77470
42 Special Treatment Procedure 77470 77470 Special treatment procedure (e.g. total body irradiation, hemibody irradiation, per oral endo-cavitary or intra-operative cone irradiation) This code covers the additional physician effort and work required for the special procedures of, total body irradiation, hemibody irradiation, intracavitary cone use, Brachytherapy, hyperthermia, concurrent chemotherapy, radiation response modifiers, stereotactic radiosurgery (single fraction or fractionated), intra-operative radiation therapy, 3-D CRT, IMRT (removed 2012), heavy particles (e.g. protons/neutrons), and any other special time-consuming and complex treatment procedure. )
 This code covers the additional physician effort and work required for the special procedures of, total body irradiation, hemibody irradiation, intracavitary cone use, Brachytherapy, hyperthermia, concurrent chemotherapy, radiation response modifiers, stereotactic radiosurgery (single fraction or fractionated), intra-operative radiation therapy, 3-D CRT, IMRT (removed 2012), heavy particles (e.g. protons/neutrons), and any other special time-consuming and complex treatment procedure. )")
70
77470 IS A GLOBAL BILLLING CODE
42 The code 77470, is designated to cover the additional time and effort required of the physician and the hospital technical staff while performing and/or managing special treatment situations. This code may be reported only one time per course of therapy. 77470 IS A GLOBAL BILLLING CODE

71
SPECIAL TREATMENT PROCEDURE WORKPAGE
43 Note the many different indications for reporting the special treatment procedure, 77470 SPECIAL TREATMENT PROCEDURE WORKPAGE ONCOCHART

72
Can anything better exemplify special treatment procedure than pediatric anesthesia?
NIB

73
A narrative note is absolutely necessary as the backup documentation for Simply including a line in a weekly progress note is not sufficient documentation to justify the billing of this code. The reasons are all here, just make certain that they are verbalized.

74
Special Procedure Note
43 Special Procedure Note This patient has just completed three months of multi-drug chemotherapy by Dr. Ishmael. We have been watching the patient over the last few weeks as the counts have slowly risen to a respectable level. The patient now has 4500 WBC's and 217,000 platelets. Patient still has marked alopecia from the chemotherapy. Considerable time was spent this morning with the patient and the patient's family explaining the possibility of continued, severe, interactions between the radiation and the just completed course of chemotherapy. It is anticipated that the patient will be experiencing a marked increase in skin reactions because of the course of Adriamycin. The treatment portals will be close to the heart, but every effort will be made to avoid treating any of the myocardium. The patient and the patient's family do understand the possibility of severe reactions and difficulties that will probably be experienced during the forthcoming course of radiation treatments. The course of radiation therapy over the next six weeks will be carefully coordinated with Dr. Ishmael. Dr. Ishmael will be available to handle any medical problems that may arise during this period of time. We will be observing the patient on a daily basis during the first part of the course of treatment to make certain that reactions are not excessive. The patient and the patient's family fully understand that the treatments are absolutely necessary but that the patient will experience considerable discomfort and other interrelated problems during the next few weeks. Carl R. Bogardus, Jr., M.D. 92/104 ONCOCHART

75
Multiple reasons for 77470

76
Special Treatment Procedures 77470
44 Special Treatment Procedures 77470 What’s it for? The additional effort involved in caring for patients under highly complex circumstances. Who normally documents this code? Varies widely, but usually the physician. When is this code normally billed? Upfront at the same time as the physician’s clinical treatment planning. What Documentation is suggested for this code? A physician narrative explaining medical necessity. What is the common documentation error identified with this code? Not documenting the code with a separate written document. What are the common billing errors identified? Missing the code due to inadequate documentation of the procedure. There is no “physical” event to trigger billing, it must be recognized by circumstances. SP89/104

77
46 If the patient is a Medicare recipient and becomes hospitalized as an inpatient, but being transported to a freestanding center each day for treatment, then the patient must be billed as an inpatient, not as an outpatient. Most freestanding centers have contracts with hospitals to cover these situations. Hospital owned departments make these corrections internally.

78
77600 – 77620 ARE GLOBAL BILLING CODES
HYPERTHERMIA 46 Covered by codes to 77620 Payment value of coverage of treatment by negotiation with local insurance carriers 77600 – ARE GLOBAL BILLING CODES 99/104

79
48 BSD Phased Array hyperthermia unit

80
HYPERTHERMIA ISOTHERMIC PLAN
NIB

81
AVAILABLE CODES 49 Only the Hyperthermia delivery codes are specific to Hyperthermia. Superficial up to 4 cm depth Deep over 4 cm in depth Probes (interstitial) 5 or less probes Probes (interstitial) 6 or more probes Probes ( intracavitary) any number New codes were planned for 2009
 5 or less probes Probes (interstitial) 6 or more probes Probes ( intracavitary) any number. New codes were planned for")
82
CODES THAT CAN BE USED 49 77263 Complex treatment planning
Special treatment procedure Initial set up simulation Subsequent simulations same area Isothermic plan, superficial Isothermic plan deep one port Isothermic plan deep, multiple ports Isothermic plan, 3-D planning Isothermic plan interstitial up to 4 probes Isothermic plan interstitial, 5-10 probes Isothermic plan interstitial, over 10 probes Isothermic plan intracavitary Basic Dosimetry for heating time calculations Calculation of areas of maximal or minimal heating

83
PRINCIPLES OF BILLING, CODING AND COMPLIANCE IN RADIATION ONCOLOGY
BMSi 2014 END 11

84
END OF SECTION 11

86
MEDICARE (CMS), 2010, REQUIRES
7 There shall be a full-time physician, preferably a radiation oncologist, per facility, physically available on a daily basis for direct supervision of daily treatment, and management of any patient related treatment problems. The 5 elements of weekly management must be documented by this physician for each week of treatment.

87
Trail Blazer opinion June 2010
11 For billing radiation treatment management, 77427, Medicare expects the radiation oncologist to bill the weekly management code for the management related to five consecutive treatment delivery sessions and to have seen the patient at least once during that time period. The actual visit could occur anytime during that time period.

88
R128BP page 13

89
Assessment of Quality of Life
23 Assessment of Quality of Life Generally done by the nursing staff but must be reviewed by the physician Pain Ambulation Social interactions Memory Psycho-social adjustment Nutritional status should always be mentioned as related to present weight Physician/patient self assessment of Q of L 51/104

90
Review of Portal Images
31 Review of current portal films or images Comparison with previous portal films or images Comparison with simulation films or images Comparison with appropriate diagnostic imaging Corrective action if necessary Review of corrected portal films or images Indicate if films not required (electrons, superficial) ONCOCHART
 ONCOCHART.")
91
Total Body or Hemi body Radiation Therapy
37 Total Body or Hemi body Radiation Therapy Total or hemi body therapy is an extremely complex procedure requiring a great deal of physician input, often requiring special testing, consultations, and physics evaluations. When only one or two treatments are given for the entire course of therapy, you should bill short course of treatment management 80/104

92
38 Valid charges for total body radiation therapy
992XX High Complexity Evaluation 77263 Therapeutic Radiology Treatment Planning; Complex 77290 Therapeutic Radiology Simulation; Complex Simulation may be repeated on different days during the initial setup procedures. 77300 Basic Radiation Dosimetry Calculation This may be calculated on many occasions. This may be reported as many times as performed and Documented. 77321 Special Teletherapy Port Plan (Electrons, if used) 77336 Continuing Medical Physics Support, 1 charged for 1 to 5 fractions. 77370 Special Medical Radiation Physics Consultation As Requested By the radiation oncologist. Usually only 1 of these would be required for a total body course of treatment.
 Continuing Medical Physics Support, 1 charged for 1 to 5 fractions Special Medical Radiation Physics Consultation. As Requested By the radiation oncologist. Usually only 1 of these would be required for a total body course of treatment.")
93
38 77331 Special Dosimetry (TLD or Diode Microdosimetry)
This may be billed as often as requested to cover all measured dose points. 77334 Special Shields Special shields for the lungs may be constructed. 77427 Weekly Megavoltage Treatment Management –22, If over 2 treatments given, Modifier –22 is used to increase the billed value. 77431 Short Course Clinical Treatment Management -22 Modifier –22 may be used to increase the value of this code. 77417 Port Films, 1 charge is allowed per week (5 fractions) of treatment. 77470 Special Treatment Procedure -22 Modifier –22 may be used for a one-time charge for the special treatment procedure.
 of treatment Special Treatment Procedure -22 Modifier –22 may be used for a one-time charge for the special treatment procedure.")
94
Review of Laboratory Data (page 18-19)
Laboratory tests, should be discussed and summarized Comparison to previous laboratory work Indicate corrective actions if necessary Ordering of any new testing as required Review of Diagnostic Imaging Studies ( page 19) Compare with previous imaging studies Compare with current portal films if indicated Ordering of any new testing or imaging as required
 Compare with previous imaging studies. Compare with current portal films if indicated. Ordering of any new testing or imaging as required.")
95
Look at errors on note

96
Rework incident to Decrease number of slides Clean up wording

97
Month End Crossing NIB On March 2009 the National Government Services, a CMS contracting agent "clarified" the proper reporting of This is reported in the Medicare Claims processing manual (100-04), Chapter 13, Section.1. In the event that five fractions occur in two different calendar months or years, the billing "from and to" dates should reflect the month in which the most fractions were performed.
, Chapter 13, Section.1. In the event that five fractions occur in two different calendar months or years, the billing from and to dates should reflect the month in which the most fractions were performed.")
98
“Clarified” method of Billing
Week Mgmt Orphaned date Orphaned date Bill first date of “clarified” week 3 Fractions make up this week

99
This makes the billing more difficult
NIB Orphaned date Orphaned date Week Mgmt We then return to a conventional 5 day week but what do we do with the 2 orphaned dates?

100
Even More Difficult with 2 days in each Crossing Segment
NIB Even More Difficult with 2 days in each Crossing Segment Which set has the week of management billed, and if only 2 fractions make up the end of a course, you cannot bill a week of management, so do we loose the last week of management billing?????

101
Summary of R128BP page 13 INCIDENT TO SERVICES The Physician direct supervision requirements are required if the services are performed within a hospital, the physician must be within the hospital, but not necessarily in the radiation therapy department, this has been clearly stated by CMS in the ruling of April 7, 2000

102
NIB ASTRO Comments,

103
If your carrier is forcing you to use this method, you should protest
NIB This illogical scheme of reporting will make billing and auditing very difficult for no rational purpose. I recall this same proposal about the year 1991 as the code was brought into use. This was soon changed to ignore the monthly crossing recommendation as being far too difficult to bill and audit. If your carrier is forcing you to use this method, you should protest

104
Summary of R128BP page 13 INCIDENT TO SERVICES If the hospital owned radiation therapy department is not physically located within, or connected to, the hospital, i.e., a free standing center then the physician must be “Interruptible” and able to intervene “right away” when Medicare patients are being treated. Free standing, non hospital owned centers are subject to this requirement

105
PORTAL-VISION IMAGES (ARIA-VARIAN)
31 DRR PORTAL IMAGE BLENDED IMAGES PORTAL-VISION IMAGES (ARIA-VARIAN) 72/104
 72/104.")
106
RULE OF 5 ROUND OFF 5

107
RADIATION THERAPY DRG There are 523 DRG Codes
45 There are 523 DRG Codes Code 409 is the only DRG with radiation therapy 409 is defined as concomitant chemotherapy and radiation therapy during the admission DRG codes do not include additional reimbursement for radiation therapy This is why you are discouraged from starting therapy while a hospital inpatient

108
2 Clinical Treatment Management does not cease for nights, holidays, week ends, or any other time of non active treatment delivery The physician remains responsible for clinical management as long as the patient is under your direct care.

109
Historical Background
2 The original three levels of complexity descriptors for treatment management were formulated in the early 1970’s. The term “treatment management” was used to describe both the supervision of treatment delivery and the clinical management of the patient.

110
Historical Background
3 In the Fall of 1990, AMA-CPT requested that the ACR and ASTRO CPT Committees work to devise a weekly treatment management system that could identify physician procedures performed, and their complex interactions. The ACR recommended that the AMA-CPT adopt the new code weekly treatment management, effective Jan 1, 1991, we have had this code for 21 years, and many physicians still have problems documenting it’s use.

111
Historical Background
3 As a key part of the negotiations to achieve , it was agreed that all the items of weekly care and management will be performed on a regular basis and documented by regular under beam progress notes

112
Availability of Physician During Treatment Management, HOPPS
11 Availability of Physician During Treatment Management, HOPPS Medicare is tightening the availability rules as part of the “Revised Incident To” ruling of Jan 1, 2009, April 7, 2009, April 1, 2010. Commercial carriers are also beginning to pay very close attention to physician availability. 25/104

113
THIS IS OUR BEST INTERPRETATION OF THE EXISTING REGULATIONS
NIB THIS IS OUR BEST INTERPRETATION OF THE EXISTING REGULATIONS Check your local carrier if in doubt about coverage, especially in rural areas of limited medical accessibility

114
12 General supervision means the procedure is furnished under the physician’s overall direction and control, but the physician’s presence is not required during the performance of the procedure. ISODOSE PLAN, BLOCKS, DOSIMETRY Direct supervision in the office setting means the physician must be present in the office suite and immediately available to furnish assistance and direction throughout the performance of the procedure. It does not mean that the physician must be present in the room when the procedure is performed. TREATMENT DELIVERY Personal supervision means a physician must be in attendance in the room during the performance of the procedure. SIMULATION, PATIENT EXAMINATION

115
The Radiation Oncologist (CMS 2010)
12 There shall be a full-time radiation oncologist per facility (Hospital out patient or Free standing center) immediately available, interruptible, and able to furnish assistance and direction throughout the procedure. The attending physician or a responsible physician (Ideally THIS PHYSICIAN SHOULD BE A RADIATION ONCOLOGIST) must be either in direct attendance or reasonably accessible during the time that radiation treatments are being delivered. 30/104
 immediately available, interruptible, and able to furnish assistance and direction throughout the procedure. The attending physician or a responsible physician (Ideally THIS PHYSICIAN SHOULD BE A RADIATION ONCOLOGIST) must be either in direct attendance or reasonably accessible during the time that radiation treatments are being delivered. 30/104.")
116
The Responsible Physician
13 It is not in accordance with the law for a Non Physician practitioner to provide physician services supervision.

117
Summary of R128BP page 13 INCIDENT TO SERVICES The CMS requirements clearly state that if the responsible physician leaves a free standing center, even to go to the hospital, then all Medicare related services must stop unless coverage is provides The 15 minute exclusion is not mentioned, as this was only a concession to ACR many years ago and never became part of CMS policy

118
Coverage under –Q5 -Q5 Services provided by a substitute physician
14 A Medical Oncologist who has been credentialed to cover daily treatment delivery patient care, Who is working in the same clinic, Who is interruptible and able to respond “Right away” -Q5 Services provided by a substitute physician

119
14 If a physician is unavailable for one week (5 treatments) then the physician who is covering will be the Physician of Record and the Week of Management must be billed under his name. The only exception is for locum tenens coverage where the billing remains in the original physician’s name.
 then the physician who is covering will be the Physician of Record and the Week of Management must be billed under his name. The only exception is for locum tenens coverage where the billing remains in the original physician’s name.")
120
e-RX Prescribe for Narcotics
Covered in section 3 page 8 e-RX Prescribe for Narcotics This is the token, a random number generator used to verify electronic narcotic prescribing.

121
New DEA controlled drug requirements
NIB New DEA controlled drug requirements DEA regulations require a pharmacy to receive a new valid signed prescription. DEA has further stated that a pharmacy may not provide a partially or fully pre-populated form for the prescribing practitioner. The physician may either fax narcotic prescriptions or send electronically if pharmacy has the capability.

122
IMRT, Electron or Kilovoltage treatment may not produce port films.
31 The review and interpretation of port films is considered as part of the weekly clinical treatment management by the physician. IMRT, Electron or Kilovoltage treatment may not produce port films. Weekly orthogonal images for IMRT setup may be billed as port films

123
45 BILLING INPATIENT CARE FROM A FREESTANDING CENTER OR HOSPITAL BASED PROGRAM By law, Medicare stipulates that the technical component of inpatient radiation therapy must be included as part of the DRG of the admission 94/104

124
Skilled Nursing Facility This may not apply to private insurance
46 Skilled Nursing Facility Patients admitted to a skilled nursing facility (SNF) under the part A benefit or a Medicare part A stay are considered to be hospital inpatients, and as such are covered under a specific DRG of admission. Treatment of these patients requires the technical component of treatment to be billed to the SNF, not Part B. This may not apply to private insurance SP98/104
 under the part A benefit or a Medicare part A stay are considered to be hospital inpatients, and as such are covered under a specific DRG of admission. Treatment of these patients requires the technical component of treatment to be billed to the SNF, not Part B. This may not apply to private insurance. SP98/104.")
125
Clinical example

126
Notice, the weekly management is being billed on the 1st date of each five-day treatment interval
NIB The progress notes are occurring regularly on Monday regardless of the elapsed number of treatments

127
Port Films 77417 33 What’s is this code for?
Weekly Port Film or Electronic Portal Imaging. Who normally documents/bills/captures this code? Treatment Therapist. When is this code normally billed? One time per five fractions, regardless of how many images are taken. What Documentation is suggested for this code? A notation in the chart that portal images were taken, and if any corrective action was needed. What are the common documentation errors identified. The lack of physician participation in the documentation. What are the common billing errors identified? Billing an incorrect number of units. Billing these images professionally (they are technical only).
.")
128
Verbatim Cut and Paste NIB This is from HHS and DOJ

129
NIB They Really Mean It

Similar presentations




 Use 99211 Many physicians and coders still struggle with.>")









 APA CPT Alternate.>")



: Selection of Principal Diagnosis/Additional Diagnoses for Inpatient.>")

