Download presentation
Presentation is loading. Please wait.

1
Implementing a Deteriorating Patient Program: a personal perspective Dr Paul Curtis Director Clinical Governance 24 Apr 13

2
NSW: a large state NSW Area = 809,000 km 2 Population = 7.25 m Pop density = 9.1/km2 Population of Sydney, Newcastle and Wollongong = 5.4m (74%) 200 hospitals Health budget = $17.3 b Scotland Area = 79,000 km 2 Population = 5.25 m Pop density = 67.5/km 2 130 hospitals NHS budget = $11.3 b
 200 hospitals Health budget = $17.3 b Scotland Area = 79,000 km 2 Population = 5.25 m Pop density = 67.5/km hospitals NHS budget = $11.3 b")
3
17 Local Health Districts

7
Clinical Excellence Commission Mission To build confidence in healthcare in NSW, by making it demonstrably better and safer for patients and a more rewarding workplace. Vision To be the publicly respected voice providing the people of NSW with assurance of improvement in the safety and quality of healthcare.

8
CEC programs include Partnering with patients BTF HAI Hand hygiene AMS & QUAIC CLAB Sepsis Special Committees CHASM, SCIDUA Clinical Leadership Blood watch Patient Identification Policy Falls prevention Medication Safety Children’s emergency care QSA Chartbook ‘Patient safety’ IIMS RCA Review Supervision National Accreditation NSW Safety Checklist Pressure Injury www.cec.health.nsw.gov.au

9
Aim To improve early recognition and response to clinical deterioration and thereby reduce potentially preventable deaths and serious adverse events in patients who receive their care in NSW public hospitals. Between the Flags Program

10
Recurring theme locally & from around the world: Failure to recognise and respond to clinical deterioration: number one clinical risk to patients (NSW Patient Safety Programme) Clinical signs of deterioration are the same everywhere Urgent action was needed The solution needed to meet the needs of patients and clinicians One size CERS would not fit all
 Clinical signs of deterioration are the same everywhere Urgent action was needed The solution needed to meet the needs of patients and clinicians One size CERS would not fit all")
12
Intervention on the Slippery Slope Patient Condition Time Clinical Review ALS Prevention Rapid Response The Solution

13
CEC approach Broad clinician engagement and consultation Keep it simple Standardisation across NSW A ‘sick’ person is sick wherever they are Allow facilities to customise their CERS Promote teamwork Promote and support clinical judgement

14
Interlude 1: Not plain sailing Delay in developing program – mid 2009 Director General mandate: 31/10/09 “Core business” Clinician engagement “Ownership” Department-CEC partnership

15
5 elements Governance Standard Calling Criteria Clinical Emergency Response System Education Evaluation

16
Element 1: Governance State wide policy and mandated implementation but local ownership with executive sponsorship and a facility based committee for oversight, education, rollout and ongoing auditing

17
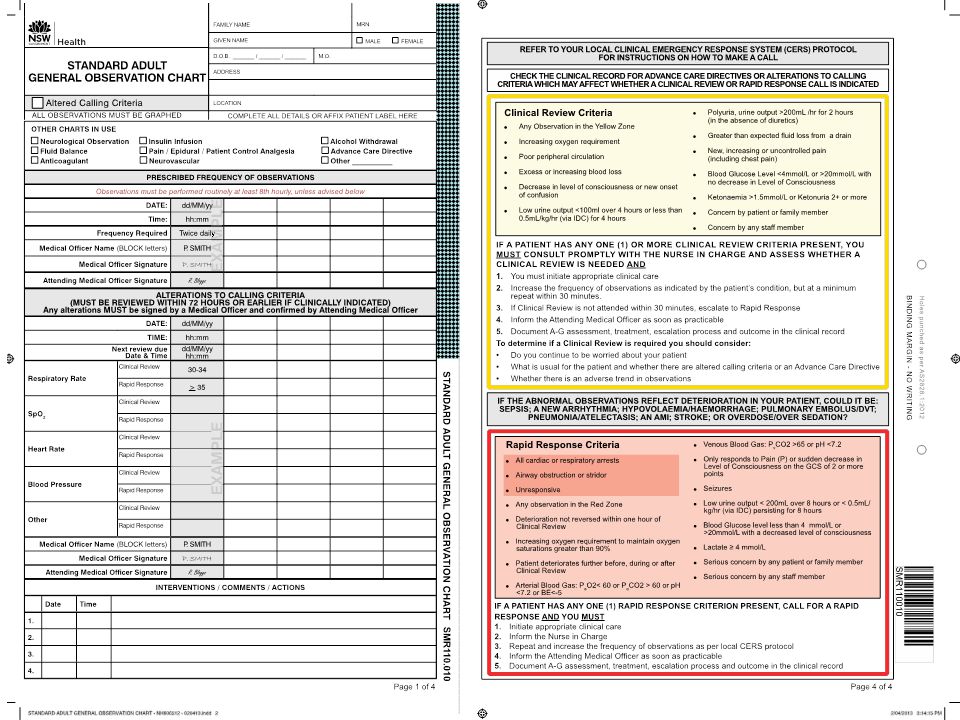
Element 2: Standard Calling Criteria and Charts Simple to use - single trigger for escalation of care Most sensitive indicator of deterioration first Graphed vs. written observations (“track and trigger”)
.")
19
Observation Charts 5 Paediatric Charts Maternity Emergency Dept eMR

20
Standard Calling Criteria and Charts Simple to use - single trigger for escalation of care Most sensitive indicator of deterioration first Graphed vs. written observations (“track and trigger”) Clinical usefulness and relevance Consolidation of observations for a ‘global’ view. Ordered ABCDEFG to support patient assessment ‘Photocopiable’ (including patient details)
 Clinical usefulness and relevance Consolidation of observations for a ‘global’ view. Ordered ABCDEFG to support patient assessment ‘Photocopiable’ (including patient details).")
21
Element 3: Escalation: Clinical Emergency Response System Unique – 2 thresholds: Yellow – sick patient – clinical review by home team. Some local discretion Red – very sick – Rapid Response Teams. No discretion Built into chart Formalise staff concerns as a legitimate triggering mechanism

22
Intervention on the Slippery Slope Patient Condition Time Clinical Review ALS Prevention Rapid Response The Solution

24
Element 4: Education 65,000 clinical staff Tier One – Awareness Training Tier Two – DETECT Training eLearning Face to face Tier Three – Responder Training

26
Patient/carer activation Piloting in some organisatons R – recognise E – engage A – Act C – call H – help in on the way About 1 call per month

27
Element 5: Evaluation - QSA

28
QSA: benefitted pt safety

29
14% reduction in RCAs

31
On line survey by UNSW QuestionsResponse % of staff that agreed/strongly agreed that Yellow Zone assisted in earlier detection & management of patients at risk of deterioration 87% % of staff that agree/strongly agree that the extra tier (Clinical Review) has improved patient safety overall 82% % of staff that use ISBAR as the communication tool for handover85% % of staff that agree/strongly agree that the Clinical Review component of the CERS has contributed to meeting the aim of the BTF program 77% % of staff that have completed DETECT training87% % of staff that agreed/strongly agreed that DETECT training improved their knowledge & skills in recognising and responding to the deteriorating patient 73%
 has improved patient safety overall 82% % of staff that use ISBAR as the communication tool for handover85% % of staff that agree/strongly agree that the Clinical Review component of the CERS has contributed to meeting the aim of the BTF program 77% % of staff that have completed DETECT training87% % of staff that agreed/strongly agreed that DETECT training improved their knowledge & skills in recognising and responding to the deteriorating patient 73%")
34
Lessons Learned Executive and Clinical Leadership A good plan Branding and marketing Partnership with Department of Health and Local Health Districts Governance structures Awareness and Education

35
Lessons Learned (cont.) An opportunity to deal with all the age old issues: Nurses unable to get a response when they are worried Doctors being called when it is not appropriate Breakdown in communication within the team Engagement ( WIIFM?)!
 An opportunity to deal with all the age old issues: Nurses unable to get a response when they are worried Doctors being called when it is not appropriate Breakdown in communication within the team Engagement ( WIIFM )!")
36
Interlude 2 Patient observations still issue Patients with clinical deterioration still are not recognised/ responded to Changing calling criteria IP issues Sustainability End of life issues

37
Conclusions Between the Flags has captured the imagination of the staff of NSW BTF is part of the language Staff believe it is making a difference Encouraging signs are there is indeed a negative correlation between Rapid Response Rate and Cardiac Arrest Rate BTF is unmasking the age old barriers to responding to end of life issues - the next challenge

38
We gratefully acknowledge Remember “Always swim between the red and yellow flags”

Similar presentations










 Module 3: Responding to clinical deterioration – managing common acute conditions Communicating clinical concerns—using ISBAR.>")




![[Hospital Name | Presenter name and title | Date of presentation]](/19/5722524/big_thumb.jpg "[Hospital Name | Presenter name and title | Date of presentation]>")










