Download presentation
Presentation is loading. Please wait.

1
Evidence Based Medicine – Introduction & Information Resources Dr. Suman Bhusan Bhattacharyya MBBS, ADHA, MBA & http://www.cebm.net/

2
An Evaluation What? Why? Where? How? Pain areas…

3
Evidence Based Medicine – What? Widely credited to have been coined by Dr. David Eddy of Kaiser Permanente It is believed that its philosophical base dates back to the sceptics of post-revolutionary France (Xavier Bichat, Pierre Louis, François Magendie) May have origins in China, B.C. The conscientious, explicit and judicious use of current best evidence in making clinical decisions about the care of individual patients (Dr. David Sackett, 1996)
 May have origins in China, B.C. The conscientious, explicit and judicious use of current best evidence in making clinical decisions about the care of individual patients (Dr. David Sackett, 1996).")
4
Evidence Based Medicine - When? There is evidence that something works, is good and benefits the patient, do it There is evidence that something does not work, is harmful, does not benefit the patient, do not do it There is insufficient evidence, be conservative, relying on individual clinician expertise

5
Evidence Based Practice - What? Any practice that applies up-to-date information from relevant and valid research about the usefulness of various diagnostic tests or the predictive power of prognostic factors or the beneficence of a particular treatment method across healthcare, including education, practice management and health economics, it is said to be EBM-enabled.

6
Evidence Based Enablement, but… Mere application of evidence based medicine is in itself simply not good enough. The end results need to be validated. This is done by performing outcomes analysis, preferably on a continuous basis

7
Evidence Based Practice – Why? The old way of depending on a combination of informed guesswork, unsystematic observation, common sense, the consensus views of clinical experts, and the so-called “standard and accepted practice”, meaning the treatments and procedures used by most other clinicians in a local community – was fine, but with the addition of enormous amounts of information every day, things are threatening to “get out of control”. So, is this way “the only way”?

8
The Pain Areas… 27 Kg of guidelines, 3000+ new papers per day, 1000 new Medline articles, 46 randomized clinical trials The number of biomedical journals alone doubling since 1970. Average workload for a clinician of anything between 100 to 200 consultations a week resulting in 5000 to 10000 per year. Add to it the difficulty of relying solely on experience while using 2 million pieces of information all stored in ones memory, ever increasing pressures to provide value-for-money services, raised patient demands and expectations, pressures due to a myriad of obtrusive and mostly confusing regulatory compliances, and rapidly altering business demands. Hmmm…

9
The Pain Areas… [Contd.] Every encounter with a patient identifies gaps in our knowledge about the etiology, diagnosis, prognosis, or therapy of their illness. Recent research reveals that even as seasoned clinicians we generate about five knowledge “needs” for every in-patient encounter, and two “needs” for every three out-patients encounters.
![The Pain Areas… [Contd.] Every encounter with a patient identifies gaps in our knowledge about the etiology, diagnosis, prognosis, or therapy of their illness.](http://images.slideplayer.com/14/4383075/slides/slide_9.jpg "Recent research reveals that even as seasoned clinicians we generate about five knowledge needs for every in-patient encounter, and two needs for every three out-patients encounters..")
10
The Pain Areas… a plausible answer To bridge these gaps and fulfill the “needs”, we need to practice evidence based medicine, and to evaluate the best evidence that evidence based medicine is supposed to reveal we need to perform outcomes analysis Practicing medicine based on best evidence in the form of clinical protocols helps as a valid legal cover in malpractice suits

11
Best Evidence… Current best evidence is up-to-date information from relevant, valid research about the effects of different forms of healthcare, the potential for harm from exposure to particular agents, the accuracy of diagnostic tests, and the predictive power of prognostic factors.

12
PICO – well built clinical questions

13
Evidence Based Medicine – How? The way of seven A’s… Assess the patienta clinical conundrum or question that arises out of the clinical examination Ask the patientthe care provider needs to construct a well-built clinical question from the findings in step 1 Access the informationthe appropriate resources needs to be selected and searched for the answer to the question framed in step 2 Appraise the evidencethe information gathered in step 3 needs to be critically appraised using the various indices for its validity and applicability to the patient ’ s problems Apply the findingsthe validated evidence needs to be integrated with clinical expertise and patient preferences and then applied as required Assess the outcomesthe performance of the evidence with the patient needs to be evaluated Add the knowledge the information so gathered added to the clinician ’ s knowledge base for future reference to best evidence in similar problems

14
Evidence Based Medicine – The Types Diagnostic –Here the importance of various observations, value of diagnostic tests, etc. are evaluated in ruling in or out a diagnosis Treatment –Here the value of a treatment method or the necessity of a particular medication or procedure is determined

15
Evidence Based Balance Sheet 1.Examine the evidence that a treatment is effective. 2.If so, then determine the magnitude of its benefits, harms, and costs. An evidence based balance sheet is an important tool that supports the practice of evidence based medicine.

16
Evidence Based Balance Sheet Display in a compact form the evidence as quantitative estimates of the effects of alternative treatments on all the important outcomes The decision-makers can more easily grasp the consequences of the different options they face. Specially useful for informed shared decision- making between physicians and patients.

17
Developing an Evidence Based Balance Sheet – The 4 Main Steps 1.Identification of the alternative treatments that are available to the patient 2.Identification of the health outcomes (i.e., the outcomes that can be experienced by, and are important to, the people who will receive the treatments) that are affected by the treatments 3.Estimation of the probabilities or magnitudes of each of the health outcomes, for each of the alternative treatments 4.Displaying the information in a table
 that are affected by the treatments 3.Estimation of the probabilities or magnitudes of each of the health outcomes, for each of the alternative treatments 4.Displaying the information in a table")
18
EBM Balance Sheet – An Example One-year probabilities of outcomes associated with Alendronate 5 mg vs. no drug, for a 55-year-old average- risk woman. Item No DrugDrugDifferenceNNT Hip fracture.00046.00032.000147143 Wrist fracture.00316.00223.000931078 Spine fracture.00144.00084.00033322 Long-term benefits0??? Inconvenience1011 Gastric distress30%0 3 Long-term Harms0??? Cost of drug$0$308+$308 Expected cost of treatment$220$203-$17 Net cost$220$511+$291

19
Problems associated with Evidence Based Practice ProblemsSolutions/Workarounds Resources and commitments in terms of time and money that needs to be delivered away from actual patient care Evaluate against opportunity cost, follow-on and abandonment option costs. Evidence based practice wins hands down as a strategic investment Finding and evaluating the evidence is costly in terms of time Use EPR Lack of skills in computer use and locating evidenceTrain personnel. This is not an issue with the generation next. Resources needed to acquire and maintain databasesAvailability in electronic form and increased usage will bring the prices down Searching may only result in discovering gaps in medical knowledge One must seriously doubt our capabilities and question our insecurities Poor indexing may lead to frustration of futile literature searches Use online searches and make all literature available searchable online The quality and quantity of research mostly unknownUse refined studies performed real-time using EPR Demands a high degree of statistics knowledgeUse EPR that have the calculations as well as their interpretations built-in Viewed as a form of rationingEvidence based medicine is about improving the quality of patient care. It is just as likely to show that effective interventions are underused as to show that ineffective procedures are over-used

20
EBM in Clinical Protocols Clinical protocols need to be made based on the current best evidence These protocols must undergo continuous revalidation in order to continue to be relevant according to the current best evidence Protocols change according to triage assessments and specialty – so they need to be user and problem-specific

21
Push, Pull, Prompt …ways to deal with too much information Evidence-Based Information Resources

22
Evolution of EBM Info PreEBM: Passive diffusion (“publish it and they will come”) Early EBM: Pull diffusion (“teach them to read it and they will come”) Current EBM: Push diffusion (“read it for them and send it to them”) Future EBM: Prompt diffusion (“read it for them, connect it to their individual patients, prompt them and their patients”)
 Early EBM: Pull diffusion ( teach them to read it and they will come ) Current EBM: Push diffusion ( read it for them and send it to them ) Future EBM: Prompt diffusion ( read it for them, connect it to their individual patients, prompt them and their patients )")
23
Information in the Internet Age* Information in the Internet age may be constrained by a variant of Malthus’ law: The amount of information is growing exponentially, but our attention is not. A wealth of information creates a poverty of attention. The low cost of production of poor quality information results in high quality information being drowned out. The cost of finding specific information rises as the amount of information increases. *Coiera E. Information economics and the internet. J Am Med Inform Assoc 2000;7:215-21.

24
The Slippery Slope years since graduation r = -0.54 p<0.001............... knowledge of current best care 100% 0% 50%

25
The McMaster PLUS project only a tiny proportion of all research is “ready for application” only a tiny fraction of the “ready” research is “relevant” to the practice of a given clinician only a tiny proportion of the “relevant” research for a given practitioner is “interesting” in the sense of being something new, important, and actionable.

26
60,000 articles/yr from 120 journals ~3,500 articles/yr meet critical appraisal and content criteria (95% noise reduction) Evidence-Based Journals Critical Appraisal Filters
 Evidence-Based Journals Critical Appraisal Filters")
27
~3,500 articles/yr meet critical appraisal and content criteria (95% noise reduction) McMaster PLUS Project Clinical Relevancy Filter (MORE) ~25 articles/yr for clinicians (99.95% noise reduction) ~5-50 articles/yr for authors of evidence- based clinical topic reviews
 McMaster PLUS Project Clinical Relevancy Filter (MORE) ~25 articles/yr for clinicians (99.95% noise reduction) ~5-50 articles/yr for authors of evidence- based clinical topic reviews")
28
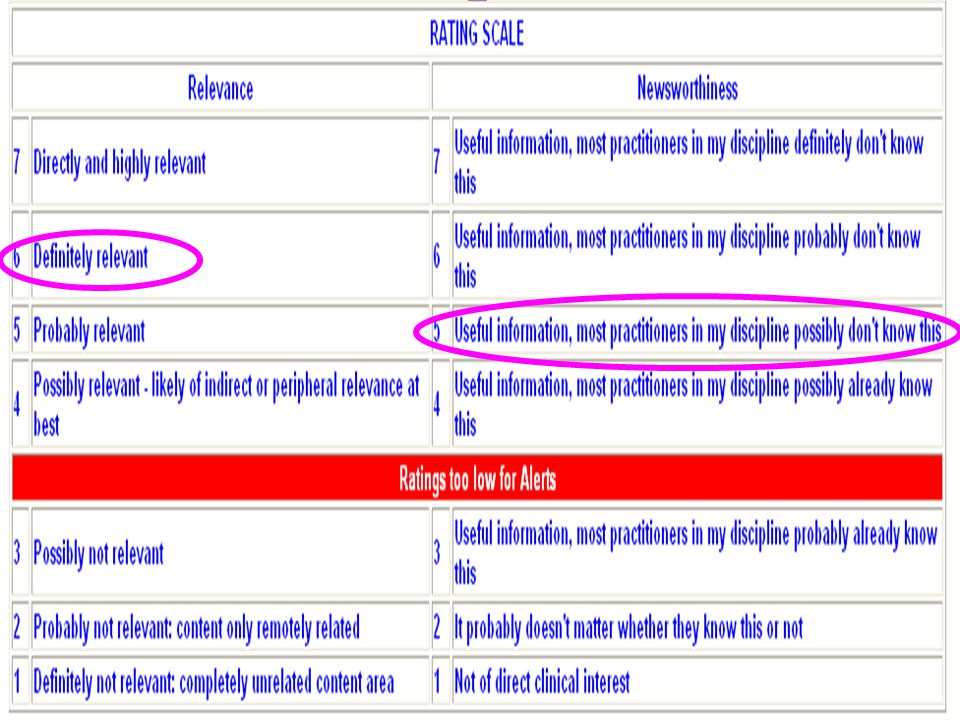
McMaster Online Rating of Evidence: >6000 practicing clinicians

30
http://bmjupdates.mcmaster.ca

31
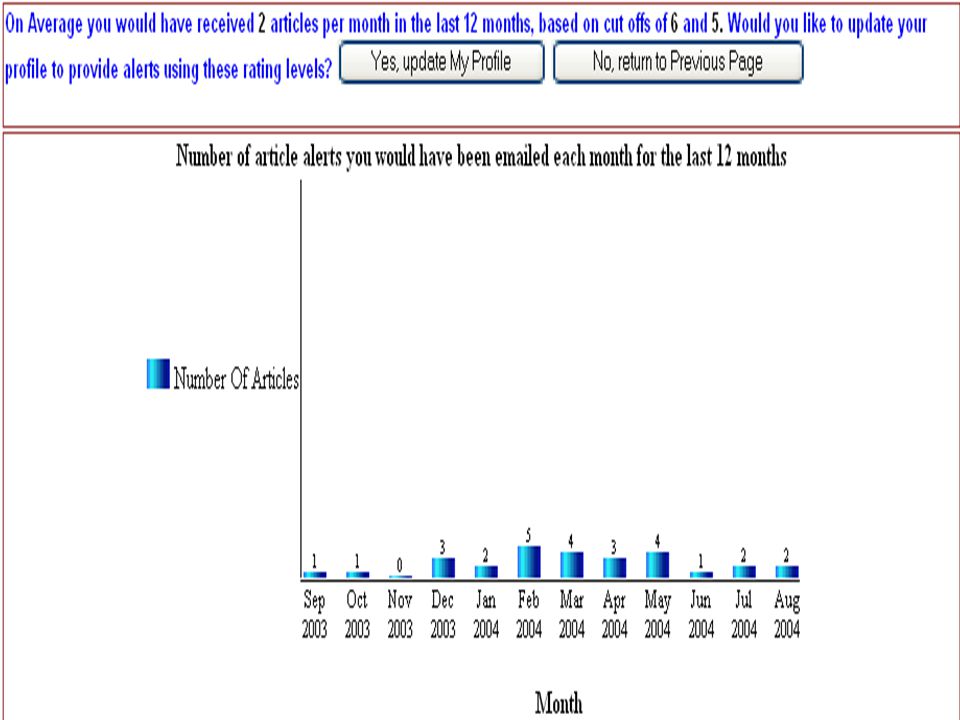
User End Users sign up according to discipline Users control relevance and flow Users can change disciplines at any time, and can sign up for as many as they wish Users can search according to discipline – or not Users can access PubMed Clinical Queries (We can monitor individual use, if agreed)
")
36
Dear Dr. Haynes, We want to alert you to NEW articles in the PLUS system. These articles that have received very high relevancy and newsworthiness scores: 1. Brazg R, et al. Effect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycaemic control and beta-cell function in patients with type 2 diabetes. Diabetes Obes Metab. 2007;9:186-93. Brazg R, et al. Effect of adding sitagliptin, a dipeptidyl peptidase-4 inhibitor, to metformin on 24-h glycaemic control and beta-cell function in patients with type 2 diabetes. Diabetes Obes Metab. 2007;9:186-93. Rated by: IM/General (patients referred from Primary Care) Relevance: 5 of 7Newsworthiness: 5 of 7 We hope that you will find these articles of value in your clinical practice. Best wishes from the PLUS Team
 Relevance: 5 of 7Newsworthiness: 5 of 7 We hope that you will find these articles of value in your clinical practice. Best wishes from the PLUS Team.")
37
CONCLUSIONS: In this 24-week study, once- daily sitagliptin monotherapy improved glycemic control in the fasting and postprandial states {vs placebo}, improved measures of beta-cell function, and was well tolerated in patients with type 2 diabetes.

38
Medscape Best Evidence Alerts Free at https://profreg.medscape.com/px/newsletter.do

39
Systems Summaries Synopses Syntheses Studies Examples Computerized decision support Evidence-based textbooks Evidence-based journal abstracts Systematic reviews Original journal articles The evolution of information resources for evidence-based decisions

40
Premier evidence resources Systems: EMR with decision support Summaries: Clinical Evidence, PIER, UpToDate, Dynamed Synopses: ACP Journal Club, EBM Syntheses: via BMJUpdates+ Studies: via BMJUpdates+, PubMed Clinical Queries

41
58 year old obese male with …type 2 diabetes mellitus …A 1c 9% (elevated) on glyburide and rosiglitazone, with metformin intolerance …continuing to gain weight …very reluctant to take insulin Can the new ‘incretin therapies’ (eg, exenatide, pramlintide or sitagliptin) help?
 on glyburide and rosiglitazone, with metformin intolerance …continuing to gain weight …very reluctant to take insulin Can the new ‘incretin therapies’ (eg, exenatide, pramlintide or sitagliptin) help")
42
Systems Summaries Synopses Syntheses Studies For type 2 diabetes, what are the effects - good and bad - of incretin therapy? Systems: no Computerized Decision Support Summaries: in UTD, PIER, Dynamed, not CE Synopses: sitagliptin in ACP JC Syntheses: one for pramlintide in BMJUpdates+ Studies: exenatide, pramlintide, sitagliptin in UTD, PIER, CE, BMJUpdates+; more on exenatide, pramlintide and sitagliptin in Clinical Queries

43
Januvia is approved for use by people with type 2 diabetes that can't be controlled adequately with diet and exercise. Section updated June 2007 Comments on exenatide, pramlintide, sitagliptin, with drug monographs for each “Many questions remain unanswered regarding clinical use and long-term outcomes with these drugs.” US$5 per pill

44
Includes exenatide, pramlintide, and sitagliptin, with drug monographs for each “Consider metformin as a first-line agent because it causes less hypoglycemia and weight gain, along with possible improvements in cardiovascular risk.” “Consider other oral agents, such as sulfonylureas, thiazolidinediones, and DPP-IV inhibitors {sitagliptin}, as reasonable first-line agents, although some are costly and the long-term benefits of these drugs have not been well studied.”

45
CONCLUSIONS: Incretin therapy offers an alternative option to currently available hypoglycemic agents for nonpregnant adults with type 2 diabetes, with modest efficacy and a favorable weight-change profile. Careful postmarketing surveillance for adverse effects, especially among the DPP4 inhibitors, and continued evaluation in longer-term studies and in clinical practice are required to determine the role of this new class among current pharmacotherapies for type 2 diabetes.

46
Survey of traditional textbooks of medicine Harrison’s Textbook – nothing Books@Ovid – nothing Kelley’s Textbook - nothing

47
My conclusions about exenatide, pramlintide, sitagliptin Interesting new options for diabetes Not well studied (eg, no comparisons with current best medications) Exenatide and pramlintide would likely be out for this patient (injections) Sitagliptin is a possibility, but not until better known options tried (acarbose, Avandamet, repaglinide)
 Exenatide and pramlintide would likely be out for this patient (injections) Sitagliptin is a possibility, but not until better known options tried (acarbose, Avandamet, repaglinide)")
48
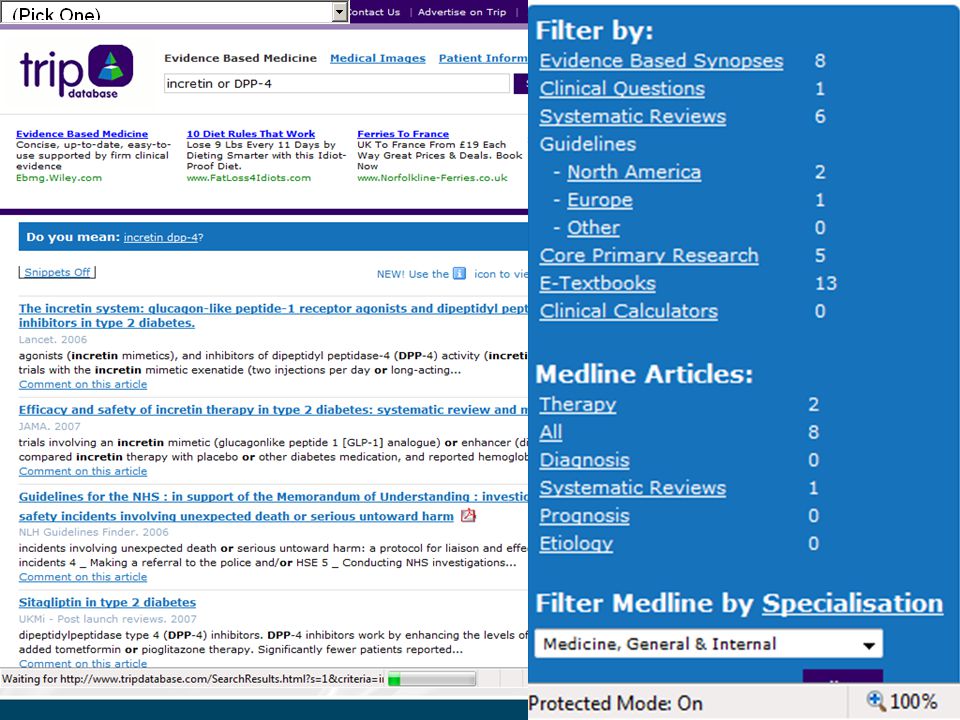
Finding evidence when you’re not sure where to look TRIP SUMSEARCH CLINICAL QUERIES

51
To keep up with evidence Pull Push Prompt…some labs and EMRs with a credible evidence- based pedigree (Zynx) Systems Summaries Synopses Syntheses Studies
 Systems Summaries Synopses Syntheses Studies")
52
Thank You!

Similar presentations




 MEDLINE Searches with.>")

 by Fiscal Year ?? U.S. National Library.>")




 – Medline or PubMed search: find and review articles –>")











