Download presentation
Presentation is loading. Please wait.

1
Diseases of gastro-intestinal tract
Assistant of professor Nechiporenko G.V.

2
Catarrhal Fibrinous Purulent Follicular Cryptous Necrotic
Acute tonsillitis Catarrhal Fibrinous Purulent Follicular Cryptous Necrotic Complications: retropharyngeal abscess, peritonsillar abscess and cellulitis, sepsis.

3
Classification of Gastritis.
ACUTE GASTRITIS Acute H. pylori gastritis Other acute infective gastritis (bacteria, viruses, fungi, parasites) Acute non-infective gastritis CHRONIC GASTRITIS Type A (autoimmune) : Body-fundic predominant Type В (H. pylori-related) : Antral-predominant gastritis Type AB (environmental) : Antral-body gastritis Chemical (reflux) gastritis : Antral-body predominant Uncommon forms of gastritis
 Acute non-infective gastritis. CHRONIC GASTRITIS. Type A (autoimmune) : Body-fundic predominant. Type В (H. pylori-related) : Antral-predominant gastritis. Type AB (environmental) : Antral-body gastritis. Chemical (reflux) gastritis : Antral-body predominant. Uncommon forms of gastritis.")
4
Morphologic classification of acute gastritis
Catarrhal gastritis Fibrinous gastritis Phlegmonous gastritis Necrotic (or Corrosive) Hemorrhagic gastritis Pseudomembranous gastritis
 Hemorrhagic gastritis. Pseudomembranous gastritis.")
5
This is a more typical acute gastritis with a diffusely hyperemic gastric mucosa.

6
At high power, gastric mucosa demonstrates infiltration by neutrophils
At high power, gastric mucosa demonstrates infiltration by neutrophils. This is acute gastritis.

7
Acute catarrhal gastritis

8
CHRONIC GASTRITIS Chronic gastritis is the commonest histological change observed in biopsies from the stomach. ETIOPATHOGENESIS. All the causative factors of acute gastritis described above may result in chronic gastritis too. Recurrent attacks of acute gastritis may result in chronic gastritis. Some other causes are as under: Reflux of duodenal contents into the stomach. Associated disease of stomach and duodenum, such as gastric or duodenal ulcer, gastric carcinoma. Chronic hypochromic anemia, especially associated with atrophic gastritis. Immunological factors such as autoantibodies to gastric parietal cells.

9
CLASSIFICATION Based on the type of mucosa affected a clinicopathologic classification has been proposed. Type A Gastritis (Autoimmune gastritis). Type A gastritis involves mainly the body-fundic mucosa. It is also called autoimmune gastritis due to the presence of circulating antibodies and is sometimes associated with other autoimmune diseases such as Hashimoto's thyroiditis and Addison's disease. Due to depletion of gastric acid-producing mucosal area, there is hypo- or achlorhydria, and hyperplasia of gastrin-producing G-cells in the antrum resulting in hypergastrinemia.
. Type A gastritis involves mainly the body-fundic mucosa. It is also called autoimmune gastritis due to the presence of circulating antibodies and is sometimes associated with other autoimmune diseases such as Hashimoto s thyroiditis and Addison s disease. Due to depletion of gastric acid-producing mucosal area, there is hypo- or achlorhydria, and hyperplasia of gastrin-producing G-cells in the antrum resulting in hypergastrinemia.")
10
Type В Gastritis (H. pylori-related)
Type В Gastritis (H. pylori-related). Type В gastritis mainly involves the region of antral mucosa and is more common. It is also called hypersecretory gastritis due to excessive secretion of acid, commonly due to infection with H. pylori. These patients may have associated duodenal or gastric ulcer. Type AB Gastritis (Environmental gastritis, Chronic atrophic gastritis). Type AB gastritis affects the mucosal region of A as well as В types (body- fundic and antral mucosa). This is the most common type of gastritis in all age groups, it is also called environmental gastritis because a number of environmental factors have been implicated in its etiopathogenesis.
. Type В gastritis mainly involves the region of antral mucosa and is more common. It is also called hypersecretory gastritis due to excessive secretion of acid, commonly due to infection with H. pylori. These patients may have associated duodenal or gastric ulcer. Type AB Gastritis (Environmental gastritis, Chronic atrophic gastritis). Type AB gastritis affects the mucosal region of A as well as В types (body- fundic and antral mucosa). This is the most common type of gastritis in all age groups, it is also called environmental gastritis because a number of environmental factors have been implicated in its etiopathogenesis.")
11
Reflux-gastritis (formerly known as Type C gastritis).
Associated with reflux of duodenal contents in stomach. May occur after gastric surgery, or with weakened pyloric sphincter tone. Localization is antrum. Achlorhydria and hypergastrinemia is absent.

12
Based on: a) the extent of inflammatory changes in the mucosa (superficial or deep), b) the activity of inflammation (quiscent or active; acute or chronic), c) the presence of type of metaplasia (intestinal or pseudo-pyloric), the following simple classification has emerged: Chronic superficial gastritis Chronic atrophic gastritis Gastric atrophy Chronic hypertrophic gastritis (Menetrier's disease) Uncommon forms of chronic gastritis
 Uncommon forms of chronic gastritis.")
13
Chronic Superficial Non-atrophic Gastritis".
1– desquamation of mucosal epithelium; 2– lymphocytes and neutrophils; 3 - non-changed fundal glands.

14
Gastritis is often accompanied by infection with Helicobacter pylori
Gastritis is often accompanied by infection with Helicobacter pylori. This small curved to spiral rod-shaped bacterium is found in the surface epithelial mucus of most patients with active gastritis. The rods are seen here with a methylene blue stain.

15
Chronic Atrophic Gastritis
1- atrophy of mucosa 2– moderate atrophy of glands; 3– decreased parietal cells; 4– intestinal metaplasia; 5 - moderate lymphohistiocytic infiltrate in lamina propria of mucosa

16
Distinguishing Features of Two Major Forms of Peptic Ulcers.
DUODENAL ULCER GASTRIC ULCER Incidence Four times more common than gastric ulcers Usual age years.More common in males than in females (4:1) Less common than duodenal ulcers Usually beyond 6th decade. More common in males than in females (3.5:1) Etiology Most commonly as a result of H. pylori infection. Other factors— hypersecretion of acid-pepsin, association with alcoholic cirrhosis, Gastric colonisation with H. pylori asymptomatic but higher chances of development of duodenal ulcer.
 Less common than duodenal ulcers Usually beyond 6th decade. More common in males than in females (3.5:1) Etiology. Most commonly as a result of H. pylori infection. Other factors— hypersecretion of acid-pepsin, association with alcoholic cirrhosis, Gastric colonisation with H. pylori asymptomatic but higher. chances of development of duodenal ulcer.")
17
Pathogenesis tobacco, hyperparathyroidism, chronic pancreatitis,
blood group 0, genetic factors Disruption of mucus barrier most important factor. Association with gastritis, bile reflux, drugs, alcohol, tobacco Pathogenesis Mucosal digestion from hyperacidity most significant factor Protective gastric mucus barrier may be damaged Usually normal-to-low acid levels; hyperacidity if present is due to high serum gastrin Damage to mucus barrier significant factor Most common along the lesser curvature and pyloric antrum

18
Patholo-gic chan-ges Complications Clinical features
Most common in the first part of duodenum Often solitary, cm in size, round to oval, punched out Histologically, composed of 4 layers—necrotic, superficial exudative, granulation tissue and cicatrisation Most common along the lesser curvature and pyloric antrum Grossly similar to duodena! ulcer Histologicaily, indistinguishable from duodenal ulcer Complications Commonly hemorrhage, perforation, sometimes obstruction; malignant transformation never occurs Perforation, hemorrhage and at times obstruction; malignant transformation in less than 1% cases Clinical features Pain-food-relief pattern Night pain common No vomiting Melena more common than hematemesis No loss of weight Food-pain pattern No night pain Vomiting common Hematemesis more common Significant loss of weight

19
Acute ulcers: They are predominantly muptiple, circular and small, less than 1 cm in diameter, not deep. Inflammatory reaction absent initially, develops secondarily. Layers of the bed : 1) fibrinous exudate with fragments of leucocytes, 2) necrotic. This type of ulcer usually heals without a visible scar.
 fibrinous exudate with fragments of leucocytes, 2) necrotic. This type of ulcer usually heals without a visible scar.")
20
A 1 cm acute gastric ulcer is shallow and sharply demarcated, with surrounding hyperemia.

21
Here is a much larger 3 x 4 cm gastric ulcer that led to the resection of the stomach shown here. This ulcer is much deeper with more irregular margins.

22
Microscopically, the ulcer here is sharply demarcated, with normal gastric mucosa on the left falling away into a deep ulcer whose base contains infamed, necrotic debris. An arterial branch at the ulcer base is eroded and bleeding.

23
Seen here is a penetrating acute ulceration in the duodenum just beyond the pylorus.

24
Chronic peptic ulcers have 4 histological zones
1. Necrotic zone — lies in the floor of the ulcer and is composed of fibrinous exudate containing necrotic debris and a few leucocytes. 2. Superficial exudative zone —lies underneath the necrotic zone. The tissue elements here show coagulative necrosis giving eosinophilic, smudgy appearance with nuclear debris. 3. Granulation tissue zone —is seen merging into the necrotic zone. It is composed of nonspecific inflammatory infiltrate and proliferating capillaries. 4. Zone of cicatrisation —is seen merging into thick layer of granulation tissue. It is composed of dense fibrocollagenic scar tissue over which granulation tissue rests.

25
The principal complications of peptic ulcer.
I. Ulcerative-destructive: Perforation. Penetration. Hemorrhage. II. Ulcerative- cicatricial (obstruction or healing and scarring) III. Malignization. IV. Inflammatory (gastritis, perigastritis, duodenitis, periduodenitis). V. Mixed.
 III. Malignization. IV. Inflammatory (gastritis, perigastritis, duodenitis, periduodenitis). V. Mixed.")
29
Appendicitis Appendicitis is inflammation of the appendix.
It is thought that appendicitis begins when the opening from the appendix into the cecum becomes blocked. The blockage may be due to a build-up of thick mucus within the appendix or to stool that enters the appendix from the cecum. The mucus or stool hardens, becomes rock-like, and blocks the opening. This rock is called a fecalith. At other times, the lymphatic tissue in the appendix may swell and block the appendix.

30
Acute appendicitis Simple Superficial Destructive types: -phlegmonous,
-phlegmonous-ulcerative, -apostematous, -gangrenous.

31
Seen here is acute appendicitis with yellow to tan exudate and hyperemia, including the periappendiceal fat superiorly, rather than a smooth, glistening pale tan serosal surface.

32
The appendix has been sectioned in half
The appendix has been sectioned in half. The serosal surface at the left shows a tan-yellow exudate. The cut surface at the right demonstrates yellowish-tan mucosal exudation with a hyperemic border.

33
Acute phlegmonous-ulcerative appendicitis

34
Here, the mucosa shows ulceration and undermining by an extensive neutrophilic exudate.

35
Complications of acute appendicitis
Septic peritonitis, mostly localized due to perforation. Appendicular abscess. It forms after mutilation of appendix. The abscess may rupture in the bladder, intestine or on the anterior abdominal wall with fistula formation. Septic thrombophlebitis leading to portal pyemia, abscesses in liver. Sepsis. Fibrotic stricture leads to mucocele or empyema of the appendix. Chronic appendicitis.

36
False appendicitis. The diagnosis of appendicitis can be difficult because other inflammatory problems may mimic appendicitis. Meckel's diverticulitis. A Meckel's diverticulum is a small outpouching of the small intestine which usually is located in the right lower abdomen near the appendix. The diverticulum may become inflamed or even perforate (break open or rupture). If inflamed and/or perforated, it usually is removed surgically.
. If inflamed and/or perforated, it usually is removed surgically.")
37
Pelvic inflammatory disease
Pelvic inflammatory disease. The right fallopian tube and ovary lie near the appendix. Sexually active women may contract infectious diseases that involve the tube and ovary. Usually, antibiotic therapy is sufficient treatment, and surgical removal of the tube and ovary are not necessary. Inflammatory diseases of the right upper abdomen. Fluids from the right upper abdomen may drain into the lower abdomen where they stimulate inflammation and mimic appendicitis. Such fluids may come from a perforated duodenal ulcer, gallbladder disease, or inflammatory diseases of the liver, e.g., a liver abscess. Right-sided diverticulitis. Although most diverticuli are located on the left side of the colon, they occasionally occur on the right side. When a right-sided diverticulum ruptures it can provoke inflammation they mimics appendicitis. Kidney diseases. The right kidney is close enough to the appendix that inflammatory problems in the kidney-for example, an abscess-can mimic appendicitis.

38
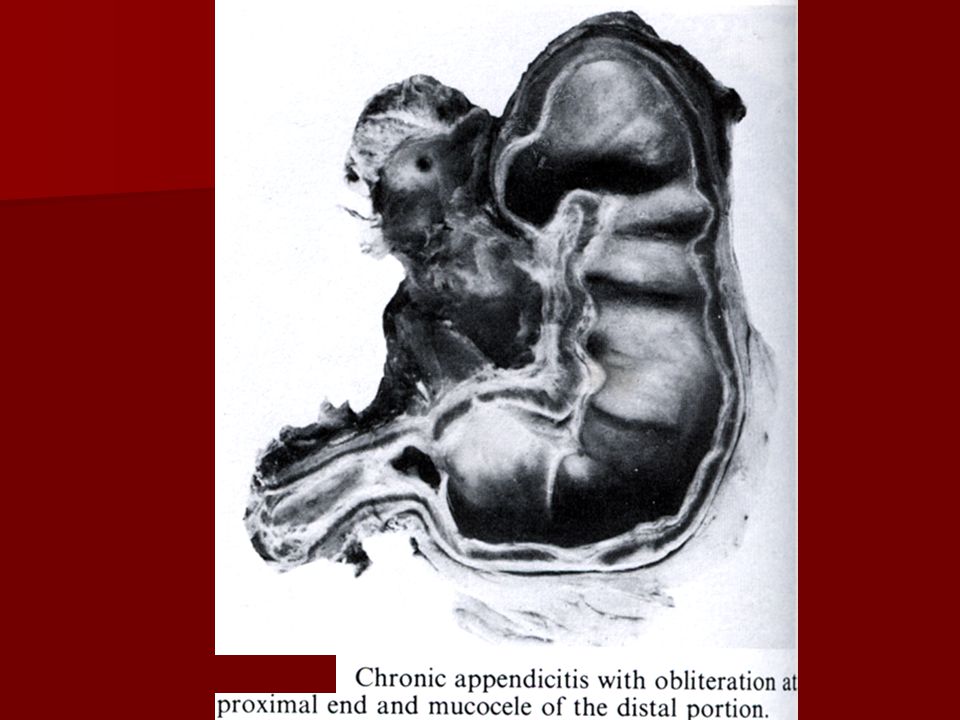
Chronic appendicitis is characterized by sclerosis and atrophy, lipomatosis and diffuse infiltration by lymphocytes and hystiocytes. Obliteration of part or all of the appendiceal lumen by a mixture of fibrous tissue, lymphocytes, lymphoid follicles, and nerve bundles is common. In the fibrosis causes complete obstruction of the lumen, continued mucous secretion may result in cystic dilatation – mucocele. Such a cyst may rupture, giving rise to myxomatosis peritonei: the mucus-secreting epithelium is spilled into the peritoneal cavity and loculations of mucin and adhesions result.

Similar presentations









>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")

>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")







 Hiatal hernia Peptic ulcer disease (PUD) Upper GI Bleeding.>")

