Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم ”وقل رب زدنى علما “

2
DR IMRANA AZIZ Assistant Professor Surgical Department

3
CYSTS & ULCERS

4
CYSTS Cyst is a fluid filled sac bound by a wall.
Fluid is often clear, colorless or cholesterol crystals, or tooth paste like. True Cyst: lined with epithelial or endothelial cells. False Cyst: which are walled off fluid collection not by epithelium e.g. Pancreatic pseudocyst

5
Classification Congenital Acquired

6
CONGENITAL CYSTS Sequestration dermoid Tubuloembryonic
Cysts of embryonic remnants Hydatid of Morgagni Cysts of the urachus Cyst of vitellointestinal duct Cysts of wolffian duct Branchial Cyst Thyroglossal Cyst

7
ACQUIRED CYSTS Retention cysts Cystic tumours Implantation dermoids
Traumatic cysts Degeneration Parasitic cysts Hydatid, trichniasis, cysticercosis

8
Sequestration dermoid:
This is due to dermal cell being buried along to the lines of closure of embryonic clefts and sinuses by skin fusion. Lined by epidermis and containing paste like material. Sites midline of body outer canthus anterior triangle of mouth.

9
Tubuloembryonic cyst:
in the track of ectodermal tube development. e.g: thyroglossal cyst, ependymal cyst.

10
Acquired cyst: Retention cyst: due to accumulation of secretion in gland behind an obstruction of a duct. e.g: sebaceous cyst, Pseudu pancreatic cyst, parotid gland cyst.

11
Distension cyst: occur in thyroid from dilatation of acni. cystic hygroma and lymphatic cyst.

12
Exudation Cyst Exudative fluid accumulate in endothelium lined anatomical space. e.g: Hydrocele, bursa.

13
Cystic tumor Implantation dermoid e.g: cystic teratoma, cystadenoma.
Squamous epithelium driven beneath skin by penetrating wound.

14
Clinical Features Varies according to the site & size
Pain → enlarging cysts, Pain → Secondary to haemorrhage, infection, rupture, torsion Acute abdominal emergency: torsion or rupture of ovarian cyst

15
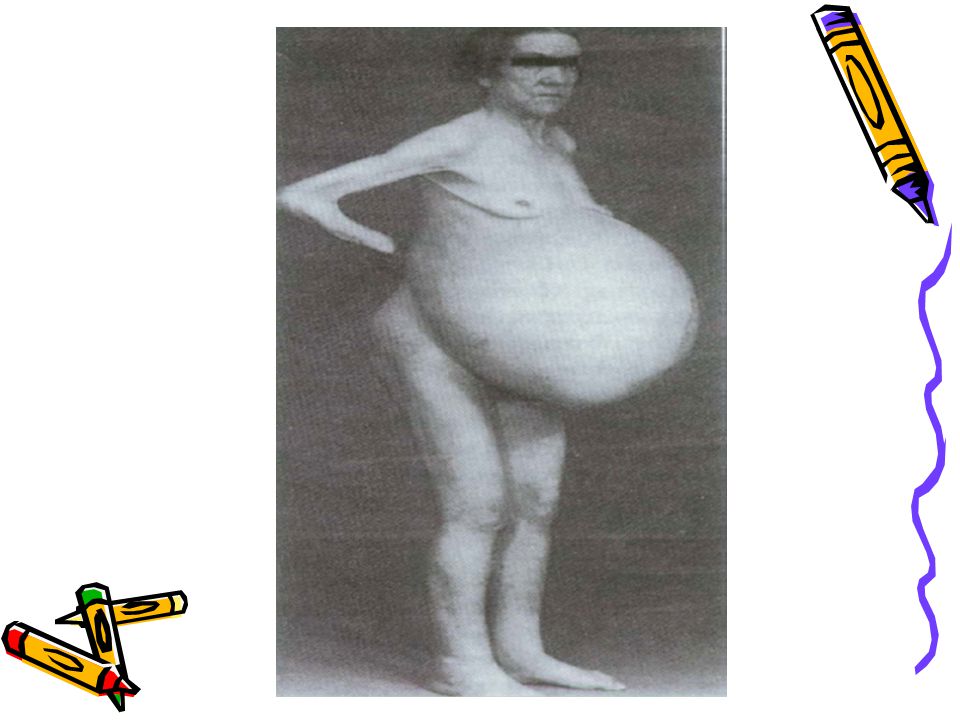
Clinical Features Compression symptoms resulting from compression of adjacent structures Haemorrhage in thyroglossal cyst → increase in size → compress the trachea Large ovarian cyst → abd: fullness & reduced appetite resulting from raises I/abd: pressure Obstruction to pelvic veins → varicose veins of lower limbs

16
COMPLICATIONS Infection Haemorrhage Torsion Obstruction Calcification
Malignancy ( very rarely)
")
17
INVESTIGATIONS Signs: Fluctuant, transilluminant if containing clear fluid Diagnosis: obvious in cases of superficial cysts Deep seated intra-abdominal or thoracic cysts need U/sound, CT scan, MRI

18
Page No. 14

19
Page No. 14

21
Page No. 196

22
Page No. 209

24
ULCER An ulcer is a break in the continuity of an epithelial surface.
Characterized by progressive destruction of the surface epithelium and a granulating base which may clean, healthy or containing necrotic slough

25
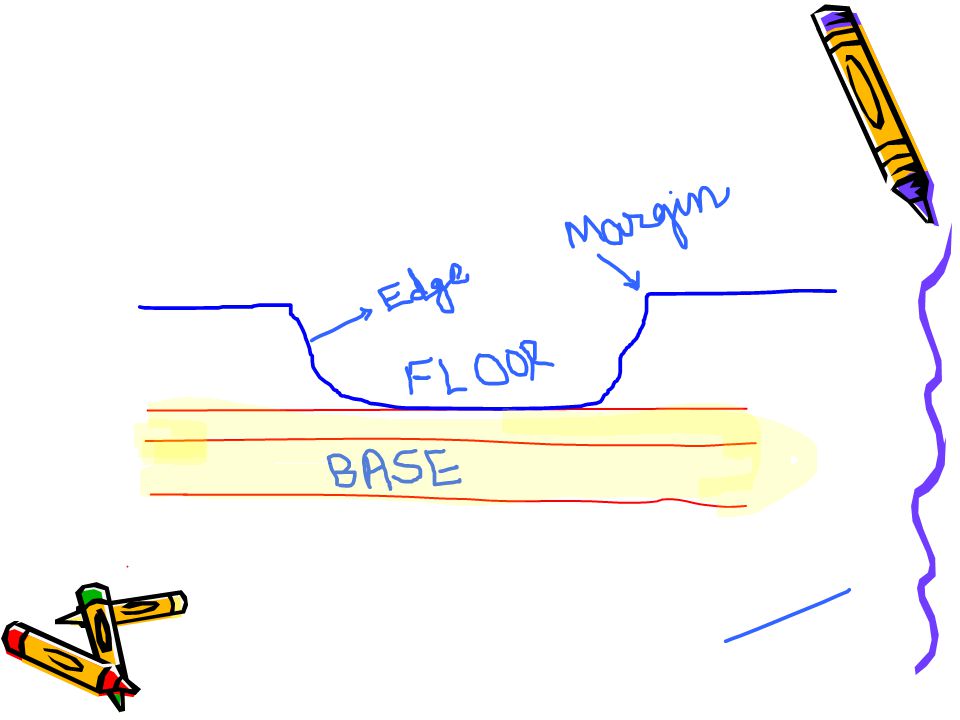
Clinical Examination Size Shape Edge Floor Base Discharge
Surrounding area Lymph nodes Pain General exam: Pathological exam:

28
Marjolin’s ulcer Malignant change occurring in any long standing benign ulcer irrespective of its cause. Change usually occurs at the edge of a chronic ulcer

29
Management Treatment of cause Accurate assessment of the ulcer
Identify & correct the co - morbid factors Adequate drainage & desloughing Antiseptics and topical antibiotics Wound dressings Hydrogel Alginates Lyofoam Tegaderm Alleyvn

30
Page No. 08

31
Page No. 07

32
Page No. 176

33
Page No. 173

34
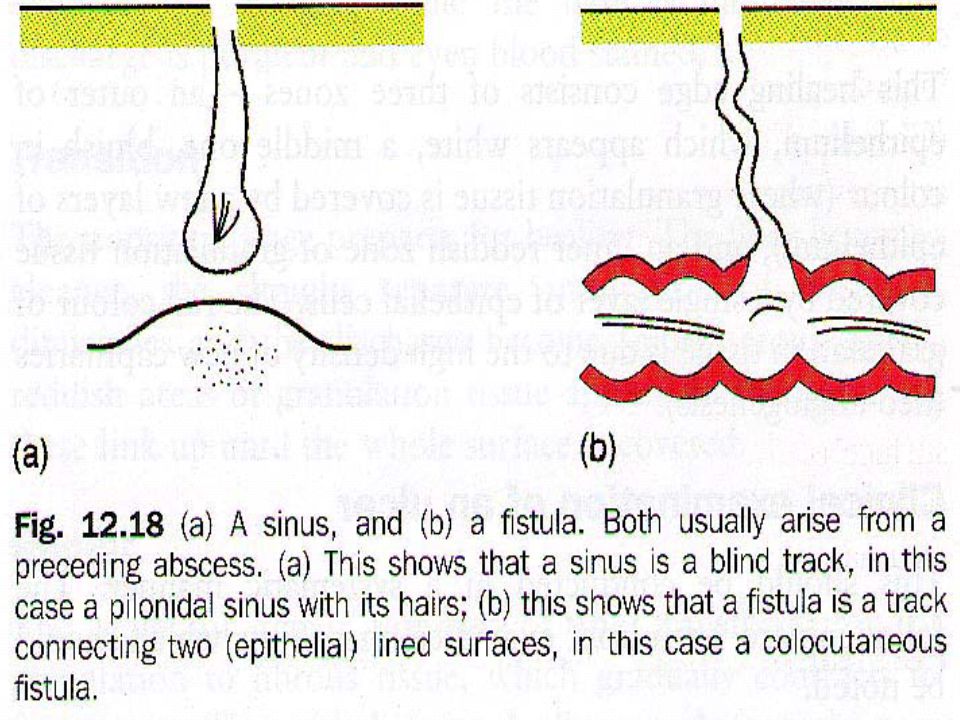
SINUSES A sinus is a blind tract usually lined with granulation tissue that leads from an epithelial surface into the surrounding tissue. e.g. pilonidal sinus

35
FISTULA It is a communicating track between two epithelial surfaces, commonly between a hollow viscus and the skin ( external fistula) or between two hollow viscera ( internal fistula) The track is lined with granulation tissue which is subsequently epithelialzed
 or between two hollow viscera ( internal fistula) The track is lined with granulation tissue which is subsequently epithelialzed.")
37
CLASSIFICATION Congenital Acquired

38
Pathological sinuses ACQUIRED 1. Pilonidal 2. Suture 3. Post-surgical
CONGENITAL 1. Preauricular 2. Umbilical 3. Urachal 4. Coccygeal 5. Sacral ACQUIRED 1. Pilonidal 2. Suture 3. Post-surgical 4. Actinomycosis 5. Tuberculosis 6. Osteomyelitis

39
Persistence of a sinus or fistula
F Foreign Body & Necrotic Tissue R Radiation I Immunosupression Infection Ischemia E Epithelization N Neoplasia D Drugs (eg: Steroids , Cytotoxic drugs) Distal Obstruction S Systemic Diseases (eg: AIDS)
 Distal Obstruction. S Systemic Diseases (eg: AIDS)")
40
Clinical features Asymptomatic Recurrent or persistent discharge Pain
Infection

41
Diagnosis Assess the accurate direction, depth & presence of multiple tracts. Microbiological examination of discharge ( gut organism, actinomycosis, tuberculosis) Sinogram
 Sinogram.")
42
Management of Sinus Complete excision of all sinus tract.
Sinus is laid open or excised Biopsy of tissue is sent Removal of the cause

Similar presentations











Primary Tumours: Benign Glomus tumour Malignant Carcinoma,sarcoma 2)Secondary Tumours: a) From adjacent areas like.>")













