Download presentation
Presentation is loading. Please wait.

1
Pulmonary Embolism Hidden Killer
Dr. Hatem Said Assistant Professor Anesthesia/ICU Ain Shams University

2
Objectives Definition Epidemiology Pathophysiology Clinical Picture
Diagnostic Tools Prophylaxis Treatment Conclusion

3
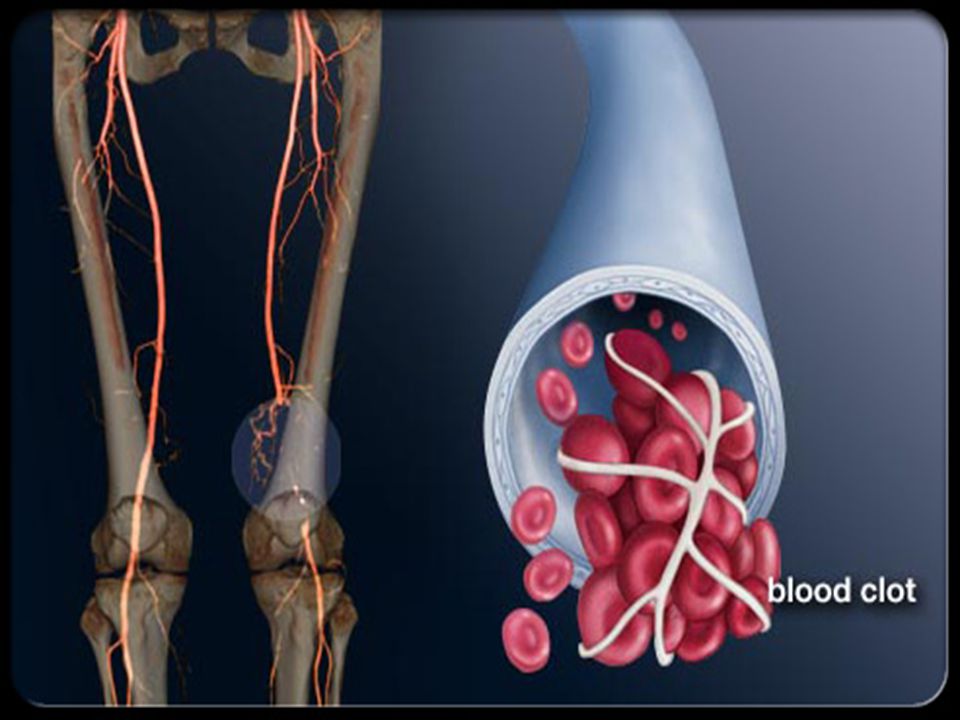
1-Definition Pulmonary embolism (PE): is an obstruction of the pulmonary artery or one of its branches by a thrombus (or thrombi) that originates somewhere in the venous system. Infarction : The pathological changes which develop in the lung as a result of pulmonary embolism The types of emboli :could be a blood clot (most common), air, fat, amniotic, fluid, and septic (from bacterial invasion of the thrombus).
: is an obstruction of the pulmonary artery or one of its branches by a thrombus (or thrombi) that originates somewhere in the venous system. Infarction : The pathological changes which develop in the lung as a result of pulmonary embolism. The types of emboli :could be a blood clot (most common), air, fat, amniotic, fluid, and septic (from bacterial invasion of the thrombus).")
4
2-Epidemiology PE : The cause of, or a major contributory factor to, death in 7-9% of necropsy cases 650,000 cases in the US each year 150,000 – 200,000 US deaths each year Most common preventable cause of hospital death 3rd most common acute cardiovascular emergency (MI and stroke)
")
5
3-Pathophysiology Source of Thrombosis (Thrombo-embolic) that originates in the venous system and embolizes to the pulmonary arterial circulation DVT in veins of leg above the knee (>90%) DVT elsewhere (pelvic, arm, calf veins, etc.) Cardiac thrombi
 DVT elsewhere (pelvic, arm, calf veins, etc.) Cardiac thrombi.")
8
3-Pathophysiology Risk factors for deep venous thromboembolism
Triad of Virchow Endothelial injury: mainly caused by either direct trauma (severed vein) or local irritation (by chemotherapy, past DVT, phlebitis). Stasis: mainly caused by heart failure, prolonged immobility. Hypercoagulation status: inherited :(AT III def., protein C, S deficiency) or acquired: (malignancy, pregnancy, nephritic syndrome, DIC and liver failure.
 or local irritation (by chemotherapy, past DVT, phlebitis). Stasis: mainly caused by heart failure, prolonged immobility. Hypercoagulation status: inherited :(AT III def., protein C, S deficiency) or acquired: (malignancy, pregnancy, nephritic syndrome, DIC and liver failure.")
9
3-Pathophysiology Risk Factors: Strong Predisposing factors
(Odds Ratio>10) Moderate Predisposing factors (Odds Ratio 2-9) Weak Predisposing factors (Odds Ratio <2) Fracture (Hip or Leg) Hip or Knee Replacement Major General Surgery Major trauma Spinal Cord Injury Arthroscopic Knee Surgery Central venous line Chemotherapy Chronic heart or respiratory failure Hormonal replacement therapy Oral Contraceptive Pills Paralytic Stroke Pregnancy/Postpartum Previous VTE Thrombophelia Bed Rest<3 days Immobility due to sitting(e.g prolonged car or air travel) Increasing Age Laparoscopic surgery (Cholecystectomy) Obesity Varicose veins
 Moderate Predisposing factors. (Odds Ratio 2-9) Weak Predisposing factors. (Odds Ratio <2) Fracture (Hip or Leg) Hip or Knee Replacement. Major General Surgery. Major trauma. Spinal Cord Injury. Arthroscopic Knee Surgery. Central venous line. Chemotherapy. Chronic heart or respiratory failure. Hormonal replacement therapy. Oral Contraceptive Pills. Paralytic Stroke. Pregnancy/Postpartum. Previous VTE. Thrombophelia. Bed Rest<3 days. Immobility due to sitting(e.g prolonged car or air travel) Increasing Age. Laparoscopic surgery (Cholecystectomy) Obesity. Varicose veins.")
16
4-Clinical Picture Revised Geneva Score (Clinical Prediction) Variable
Points Predisposing Factors: Age>65 years Previous DVT or PE Surgery or fracture within 1 month Active malignancy +1 +3 +2 Symptoms: Unilateral lower limb pain Haemoptysis Clinical Signs Heart Rate 75-94 bpm >95bpm Pain on LL deep vein and unilateral edema +5 +4 Clinical probability: Low Intermidiate High Total 0-3 4-10 >11

17
4-Clinical Picture Wells Score (Clinical Prediction) Variable Points
Predisposing Factors: Previous DVT or PE Recent Surgery or immobilization Cancer +1.5 +1 Symptoms: Haemoptysis Clinical Signs Heart Rate >100 bpm Clinical signs of DVT Clinical Judgement Alternative diagnosis less likely than PE +3 Clinical probability: Low Intermidiate High Total 0-1 2-6 >7

18
4-Clinical Picture Most PE are small embolism will reach the periphery of the lung, sometimes producing wedge shaped shadow (pulmonary infarction) on CxR . A large embolism suddenly obstructing a major pulmonary vessel has marked effects on cardiac function , often associated with anterior chest pain and collapse. Chronic recurrent pulmonary embolism may develop pulmonary hypertension and right ventricular failure
 on CxR . A large embolism suddenly obstructing a major pulmonary vessel has marked effects on cardiac function , often associated with anterior chest pain and collapse. Chronic recurrent pulmonary embolism may develop pulmonary hypertension and right ventricular failure.")
19
4-Clinical Picture SYMPTOMS : Massive PE: Dyspnea (84%). -Shock.
Pleuritic pain (74%) Dyspnea, Cyanosis. Anterior chest pain (68%) Apprehension, Sweating. Cough (53%) Chest pain, Tachycardia, AF Hemoptysis (30%). Asymptomatic (10%). SIGNS: Tachypnea (70%). Rales (51%). Tachycardia (30%). S4 (24%). Accentuated P2.
. -Dyspnea, Cyanosis. Anterior chest pain (68%). -Apprehension, Sweating. Cough (53%). -Chest pain, Tachycardia, AF. Hemoptysis (30%). Asymptomatic (10%). SIGNS: Tachypnea (70%). Rales (51%). Tachycardia (30%). S4 (24%). Accentuated P2.")
20
4-Clinical Picture Differential Diagnosis: Myocardial Infarction.
Pluerisy/Pericarditis. Tachyarrhythmia. Musculoskeletal/rib fracture. Lobar Collapse secondary to tumor. Asthma. Pneumonia. Pneumothorax. Perforating Peptic Ulcer. Acute Pancreatitis. Differential Diagnosis of Massive Pulmonary Embolism: Acute pulmonary edema Cardiac tamponade. Dissecting Aortic Aneurysm. Shock/sepsis.

21
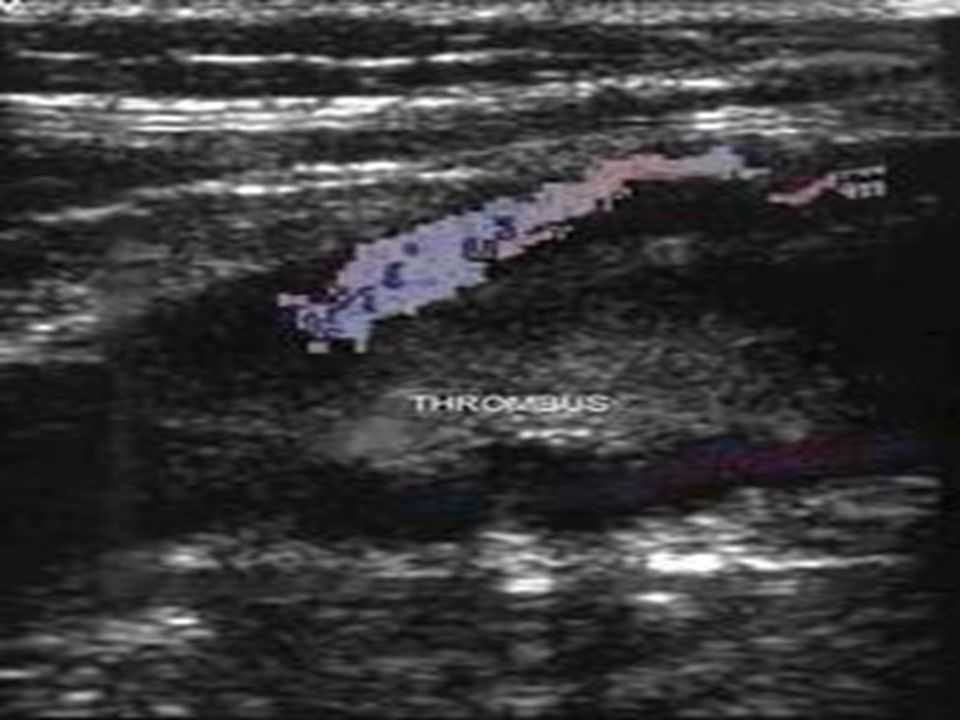
Duplex US with compression of the lower extremities
5-Diagnostic Tools Duplex US with compression of the lower extremities Non-invasive test that accurately detects proximal DVT in LE (70-80% of pts with PE have concomitant proximal DVT) Often used in workup of PE before going to more invasive procedures Invasive test: Venography (definitive diagnosis)
 Often used in workup of PE before going to more invasive procedures. Invasive test: Venography (definitive diagnosis)")
24
5-Diagnostic Tools Laboratory Investigations (Non Specific): leukocytosis , ESR elevation, LDH, SGOT elevation with normal bilirubin. CK, CK MB or Troponin I should be checked to rule out AMI ABG Normal does NOT rule out PE Hypoxia, hypocapnia, respiratory alkalosis. D-Dimer: High sensitivity but poor specificity Negative prediction<500 ng /ml is a powerful excluding tool for PE

25
5-Diagnostic Tools Chest X-ray: Abnormal in 88% of acute PE
Atelectasis (60-70%): most common finding in PE without infarction. Westermark sign (increased lucency in area of embolus) Hampton Hump (wedge-shaped pleural-based infiltrate) Abrupt cutoff of vessel Pleural effusion
: most common finding in PE without infarction. Westermark sign (increased lucency in area of embolus) Hampton Hump (wedge-shaped pleural-based infiltrate) Abrupt cutoff of vessel. Pleural effusion.")
26
Westermark Sign: represents a focus of oligemia (vasoconstriction )seen distal to a pulmonary embolism
seen distal to a pulmonary embolism")
27
Hampton Hump: Radiologic sign which consists of a shallow wedge-shaped opacity in the periphery of the lung with its base against the pleural surface. Occurs 12 to 36 hours after symptoms begin; usually indicates pulmonary infarction

29
5-Diagnostic Tools ECG:
Most common: sinus tachycardia +/- nonspecific ST-segment and T-wave changes “Classic S1-Q3-T3 pattern” Other signs of right heart strain (ie, new RBBB and ST changes ,T wave inversion in V1,2 Echocardiography: It may be helpful after a large PE in a compromised patient, as it can show right heart dilatation , occasionally thrombus and increased pulmonary arterial pressure readings if tricuspid regurgitation developed. Convenient and rapidly available

30
ECG findings

31
Echocardiography Findings

32
Echocardiography Findings
Transesophageal echocardiographic shows the reduction in size of the clot (arrow) (PA, pulmonary artery; RA, right atrium; Ao, aorta) Transesophageal echocardiographic findings showing the floating thrombus (arrow) into central pulmonary artery (PA, pulmonary artery; RA, right atrium; Ao, aorta)
 (PA, pulmonary artery; RA, right atrium; Ao, aorta) Transesophageal echocardiographic findings showing the floating thrombus (arrow) into central pulmonary artery (PA, pulmonary artery; RA, right atrium; Ao, aorta)")
33
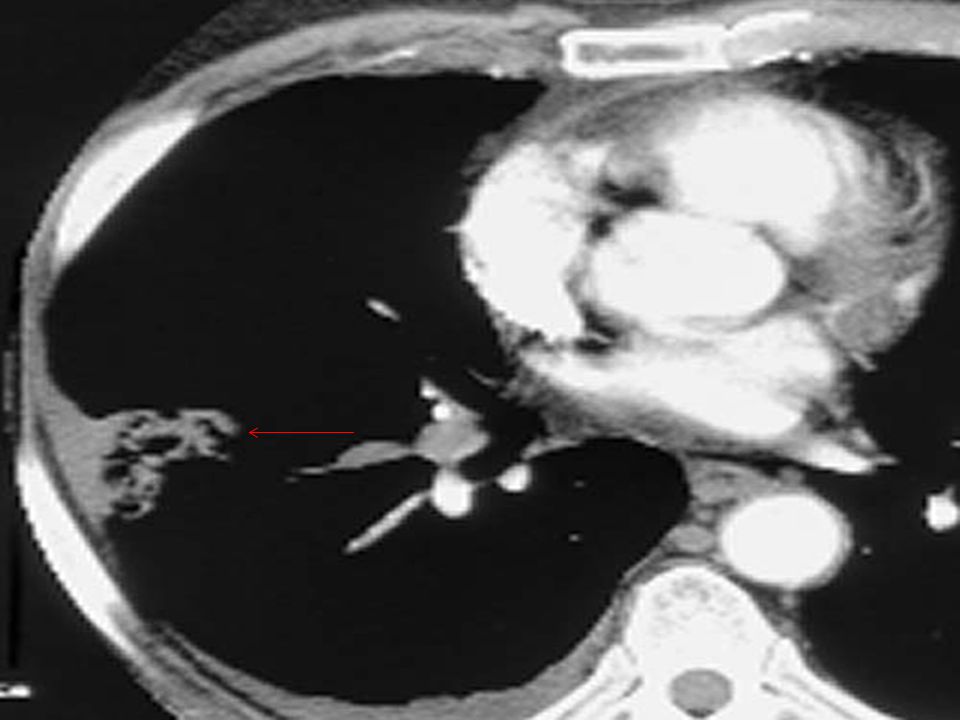
Helical(Spiral) CT Sensitivity 85% (more sensitive for proximal emboli but is less good at detecting peripheral emboli, which may account for up to 30% of PE vessels) Specificity 95% It may be used as a first line investigation when V/Q Scan is delayed and when a large PE is suspected and early diagnosis is needed first-
 Specificity 95% It may be used as a first line investigation when V/Q Scan is delayed and when a large PE is suspected and early diagnosis is needed first-")
38
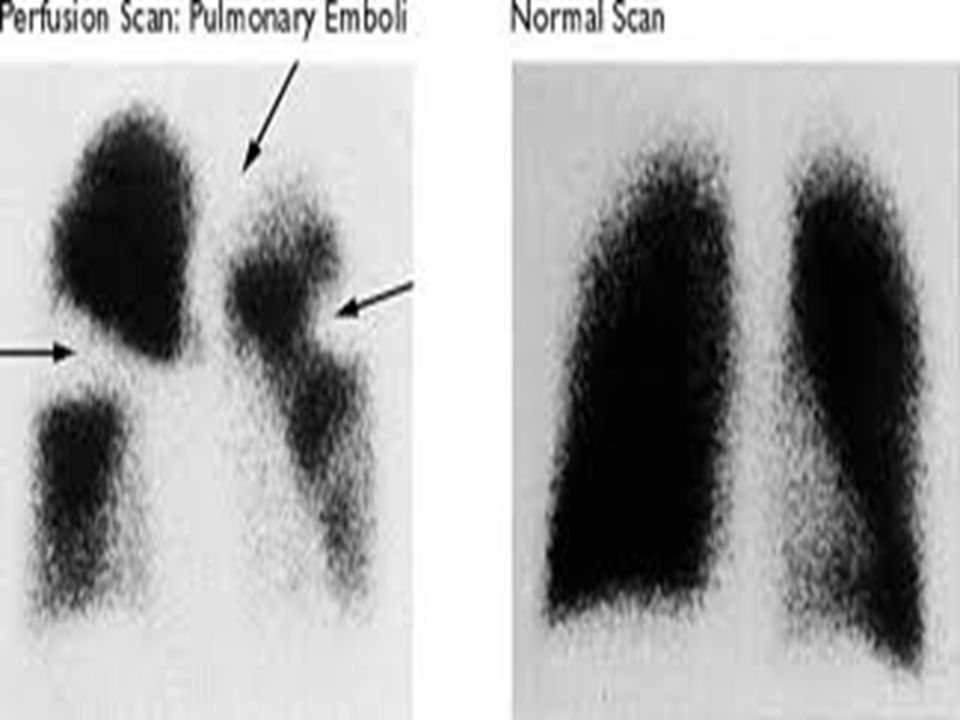
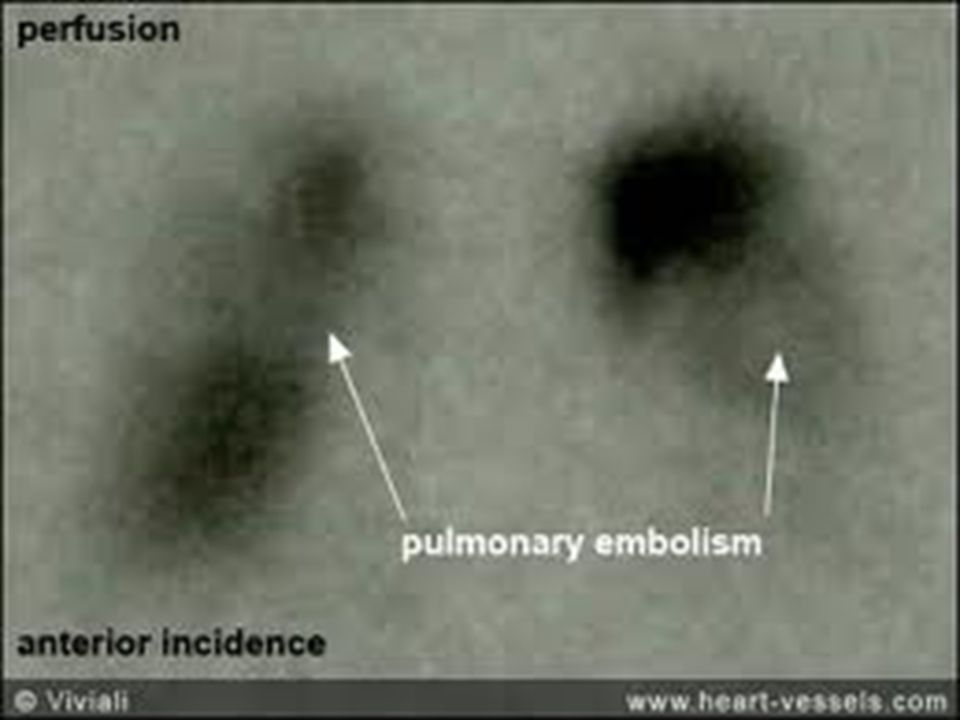
V/Q Scan Identifies mismatches between areas that are ventilated but not perfused Best initial test in patients with clear CXR Normal: rules out PE High-probability scan: is diagnostic of PE if the clinical suspicion is also high Low-probability scan: rules out PE only in a pt with low pretest clinical probability (because PE is found in roughly 15% of pts with low-probability scans) Intermediate-probability scan: requires further evaluation (16-66% chance of PE depending on pretest probability)
 Intermediate-probability scan: requires further evaluation (16-66% chance of PE depending on pretest probability)")
43
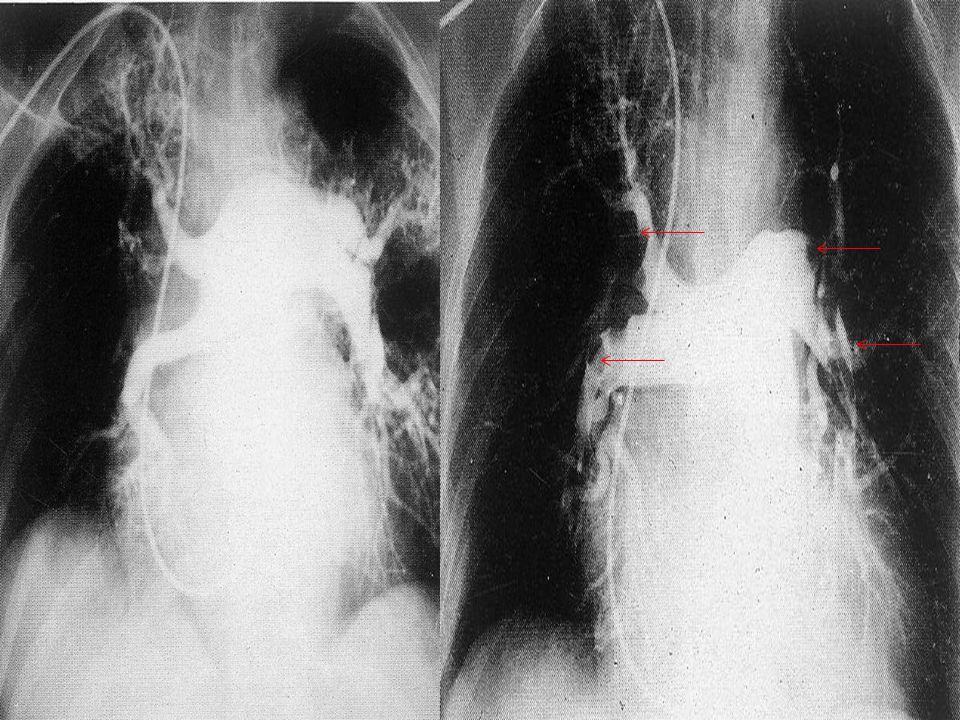
Pulmonary Angiography
“Gold Standard” but is invasive, time consuming, needs experienced radiologists 5% morbidity < 0.5% mortality Indicated if the diagnosis remains uncertain after noninvasive testing

47
6- Prophylaxis Encourage all patients to ambulate as soon as possible
determine patient at risk: Low risk :(<40 years old, ambulating, minor surgery) don't need prophylaxis. Moderate risk: (>40 years old, abdominal, pelvic or thoracic surgery) pneumatic compression, or low dose heparin prophylaxis. High risk: (>60years old, prior DVT or PE malignancy, orthopedic surgery hypercoagulability state) combination of pneumatic compression and low dose heparin prophylaxis or Dextran. Coumadine or IVC filter are considered.
 don t need prophylaxis. Moderate risk: (>40 years old, abdominal, pelvic or thoracic surgery) pneumatic compression, or low dose heparin prophylaxis. High risk: (>60years old, prior DVT or PE malignancy, orthopedic surgery hypercoagulability state) combination of pneumatic compression and low dose heparin prophylaxis or Dextran. Coumadine or IVC filter are considered.")
48
IVC Filter: if anticoagulation is contraindicated (e. g
IVC Filter: if anticoagulation is contraindicated (e.g., active GI bleed, intracranial neoplasm, Ophthalmology patient , known bleeding diathesis), if thrombus formed despite adequate anticoagulation, or with a large burden of thrombosis in the LE that could be fatal if embolized.
, if thrombus formed despite adequate anticoagulation, or with a large burden of thrombosis in the LE that could be fatal if embolized.")
51
6- Prophylaxis Rivaroxaban (Oral factor X a inhibitor)
New Drug that provide a simple, fixed-dose regimen for treating acute DVT and for continued treatment, without the need for lab. Monitoring. Approved (FDA) for prophylaxis in post-operative period after knee & hip replacement and chronic AF. Nearly it will approved for treatment of acute PE. Antidote: Thrombin Complex Concentrate.
 for prophylaxis in post-operative period after knee & hip replacement and chronic AF. Nearly it will approved for treatment of acute PE. Antidote: Thrombin Complex Concentrate.")
52
7-Treatment Primary Treatment: Supplemental oxygen for hypoxemia.
If the PE is large, supportive treatments for hypotension or reduced CO should be given IVF , Levophed , or Dopamine/Mechanical Ventilatory Support Specific treatment is with intravenous unfractionated heparin infusion following an initial bolus dose 80 U/kg bolus, then 18 U/kg/hr a PTT should be monitored 6 hours after initiation, 6 10 hours after any dosage change, then daily with a target of seconds. Heparin does not reduce acute mortality but significantly reduces further events

53
7-Treatment LMWH: Current guidelines for patients with acute nonmassive pulmonary embolism recommend LMWH over UFH. LMWHs have many advantages over UFH: These agents have a greater bioavailability, can be administered by subcutaneous injections, and have a longer duration of anticoagulant effect. - A fixed dose of LMWH can be used ( 30mg, sc, bid), and laboratory monitoring of a PTT is not necessary Chest. Jun 2008;133(6 Suppl):454S-545S
, and laboratory monitoring of a PTT is not necessary. Chest. Jun 2008;133(6 Suppl):454S-545S.")
54
7-Treatment Oral Anticoagulation:
Oral Warfarin can be given with the initiation of Heparin keep INR between 2- 3 with initial dose of 5mg/day for 2 days (The peak effect does not occur until hours after drug administration) . An overlap of 4- 5 days with a therapeutic INR and a PTT is recommended . Persistent oral Warfarin should be prescribed for 3 months till the absence of risk factors LMWH can be used when Warfarin is contraindicated (e.g. pregnancy) .
 . An overlap of 4- 5 days with a therapeutic INR and a PTT is recommended . Persistent oral Warfarin should be prescribed for 3 months till the absence of risk factors. LMWH can be used when Warfarin is contraindicated (e.g. pregnancy) .")
55
7-Treatment Long-term anticoagulation
1st event with reversible risk factors: 3-6 months Warfarin. Idiopathic PE/DVT: 6 months Warfarin. 2nd event, cancer, preexisting irreversible risk factors, such as deficiency of antithrombin III, protein S and C Deficiency: 12 month to life long Warfarin. BMJ. Mar ;334(7595):674
:674.")
56
7-Treatment Potential indications for THROMBOLYTIC THERAPY in venous thromboembolism (acceptable risk of bleeding complications) : significant cardiac compromise , RV strain (Dysfunction) . presence of hypotension related to PE not responding to IVF and vasopressor resuscitation. Presence of severe hypoxemia. Substantial perfusion defect. Extensive DVT. Thrombolytic therapy achieves faster resolution of the thrombus and more rapid recovery of normal vascular flow than simple anticoagulation.
 . presence of hypotension related to PE not responding to IVF and vasopressor resuscitation. Presence of severe hypoxemia. Substantial perfusion defect. Extensive DVT. Thrombolytic therapy achieves faster resolution of the thrombus and more rapid recovery of normal vascular flow than simple anticoagulation.")
57
7-Treatment Regimens for thrombolysis in Pulmonary Embolism:
Drug Regimen Streptokinase IU in min followed by IU/Hour up to 24 Hours t-PA MG IV over 1-2 min followed by an infusion of 90 MG over 2 Hours Cerebral hemorrhage can occur in up to 1% of cases It has been used successfully and safely in a pregnant woman and this is not a contraindication unless immediately postpartum

58
7-Treatment Pulmonary Embolectomy:
This is reserved for severe cardiac compromise where thrombolysis has either failed or is contraindicated. It requires an experienced team to be successful and, although used infrequently, small studies (Doerge et al, 1999) have shown favorable outcomes.
 have shown favorable outcomes.")
59
8-Conclusion Untreated PE is associated with high mortality ,Suspected PE demands prompt diagnostic testing & assessment of risk factors & clinical probability, with empirical clinical assessment & a validated clinical prediction score when possible.

Similar presentations