Download presentation
Presentation is loading. Please wait.

1
CLARIFYING CONFUSION: A RESEARCH APPROACH TO DELIRIUM Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Yale University School of Medicine F:/shared/inouye/talks&slides/McMaster_Medical Grand Rounds.doc

2
WHAT IS DELIRIUM? (Acute Confusional State) Definition: acute decline in attention and cognition Characteristics: common problem serious complications often unrecognized may be preventable
 Definition: acute decline in attention and cognition Characteristics: common problem serious complications often unrecognized may be preventable.")
3
EPIDEMIOLOGY OF DELIRIUM Prevalence (on admission)10-40% Incidence (in hospital)25-60% Hospital mortality:10-65% 2-20 x controls Excess annual health care expenditures:>$8 billion
10-40% Incidence (in hospital)25-60% Hospital mortality:10-65% 2-20 x controls Excess annual health care expenditures:>$8 billion")
4
CURRENT IMPACT OF DELIRIUM 35% of the U.S. population aged ≥ 65 years is hospitalized each year, accounting for > 40% of all inpatient days Assuming a delirium rate of 20%: –7% of all persons ≥ 65 years will develop delirium annually –Delirium will complicate hospital stay for > 2.2 million persons/year, involving > 17.5 million in-patient days/year Estimated costs: > $8 billion/year

5
IMPACT OF DELIRIUM Beyond hospital costs Post-hospital costs Institutionalization Rehabilitation Home care Caregiver burden Aging of U.S. population

6
RECOGNITION OF DELIRIUM Previous studies: 32-66% cases unrecognized by physicians Yale-New Haven Hospital study (1988-1989): –65% (15/23) unrecognized by physicians –43% (10/23) unrecognized by nurses
: –65% (15/23) unrecognized by physicians –43% (10/23) unrecognized by nurses")
7
DEVELOPMENT OF A DELIRIUM INSTRUMENT Ref: Inouye SK, et al. Ann Intern Med. 1990, 113: 941-8.

8
CONFUSION ASSESSMENT METHOD (CAM) Developed to provide a quick, accurate method for detection of delirium For non-psychiatrically trained clinicians Both clinical and research settings
 Developed to provide a quick, accurate method for detection of delirium For non-psychiatrically trained clinicians Both clinical and research settings")
9
KEY FEATURES OF DELIRIUM 1)Acute onset and fluctuating course 2)Inattention 3)Disorganized thinking 4)Altered level of consciousness Note: disorientation and inappropriate behavior not useful diagnostically
Acute onset and fluctuating course 2)Inattention 3)Disorganized thinking 4)Altered level of consciousness Note: disorientation and inappropriate behavior not useful diagnostically")
10
CAM ACUTE ONSET “Is there evidence of an acute change in mental status from the patient’s baseline?”

11
CAM FLUCTUATING COURSE “Did this behavior fluctuate during the past day, that is, tend to come and go or increase and decrease in severity?”

12
CAM INATTENTION “Did the patient have difficulty focusing attention, for example, being easily distractible, or having difficulty keeping track of what was being said?”

13
CAM DISORGANIZED SPEECH “ Was the patient’s speech disorganized or incoherent, such as, rambling or irrelevant conversation, unclear or illogical flow of ideas, or unpredictable switching from subject to subject?”

14
CAM ALTERED LEVEL OF CONSCIOUSNESS “ Overall how would you rate this patient’s level of consciousness?” Alert (normal) Vigilant (hyperalert) Lethargic (drowsy, easily aroused) Stupor (difficult to arouse) Coma (unarousable)
 Vigilant (hyperalert) Lethargic (drowsy, easily aroused) Stupor (difficult to arouse) Coma (unarousable)")
15
SIMPLIFIED DIAGNOSTIC CRITERIA -- Uses 4 criteria assessed by CAM: (1) acute onset and fluctuating course (2) inattention (3) disorganized thinking (4) altered level of consciousness -- The diagnosis of delirium requires the presence of criteria: (1), (2) and (3) or (4)
 acute onset and fluctuating course (2) inattention (3) disorganized thinking (4) altered level of consciousness -- The diagnosis of delirium requires the presence of criteria: (1), (2) and (3) or (4)")
16
VALIDATION OF CAM Site I Site II (n=30) (n=26) Sensitivity10/10 (100%)15/16 (94%) Specificity19/20 (95%) 9/10 (90%) Positive predictive accuracy10/11 (91%)15/16 (94%) Negative predictive accuracy19/19 (100%) 9/10 (90%) Likelihood ratio 20.0 9.4 (positive test)
 (n=26) Sensitivity10/10 (100%)15/16 (94%) Specificity19/20 (95%) 9/10 (90%) Positive predictive accuracy10/11 (91%)15/16 (94%) Negative predictive accuracy19/19 (100%) 9/10 (90%) Likelihood ratio (positive test)")
17
CAM SIGNIFICANCE Helped to improve recognition of delirium Widely used standard tool for clinical and research purposes nationally and internationally Translated into five languages Used in over 100 original published studies to date

18
MULTIFACTORIAL MODEL OF DISEASE IN OLDER PERSONS

19
BASELINE VULNERABILITY Development and Validation of a Predictive Model for Delirium based on Admission Characteristics Ref: Inouye SK, et al. Ann Intern Med 1993;119:474-81.

20
SPECIFIC AIMS 1.To identify risk factors for the development of delirium. 2.To develop and validate a predictive model for development of delirium based on admission characteristics.

21
METHODS Patients: 2 prospective cohorts of consecutive patients age ≥ 70 years on the medicine service, done in tandem, with 107 and 174 patients Assessments: Daily patient and nurse interviews, with CAM ratings

22
DEVELOPMENT OF THE PREDICTIVE MODEL 13 variables with RR ≥ 1.5 entered into a stepwise multivariable model 4 risk factors selected for the final predictive model

23
INDEPENDENT RISK FACTORS FOR DELIRIUM (N=107) Risk Factor Adjusted Relative Risk (95% CI) Vision Impairment 3.5 (1.2, 10.7) Severe Illness 3.5 (1.5, 8.2) Cognitive Impairment 2.8 (1.2, 6.7) BUN/Cr Ratio ≥ 18 2.0 (0.9, 4.6)
 Risk Factor Adjusted Relative Risk (95% CI) Vision Impairment 3.5 (1.2, 10.7) Severe Illness 3.5 (1.5, 8.2) Cognitive Impairment 2.8 (1.2, 6.7) BUN/Cr Ratio ≥ (0.9, 4.6)")
24
PERFORMANCE OF THE PREDICTIVE MODEL Development of Delirium No. of Risk Factors Initial Cohort n/N (%) RR Validation Cohort n/N (%) RR 0 3/33 (9)1.0 1/30 (3)1.0 1-214/61(23)2.516/103(16)4.7 3-410/12(83)9.2 12/38(32)9.5
 RR Validation Cohort n/N (%) RR 0 3/33 (9)1.0 1/30 (3) /61(23)2.516/103(16) /12(83)9.2 12/38(32)9.5.")
25
PRECIPITATING FACTORS Development and Validation of a Predictive Model for Delirium based on Hospitalization – Related Factors Ref: Inouye SK, et al. JAMA 1996;275:852-7.

26
SPECIFIC AIMS 1.To identify potential precipitating factors for delirium 2.To develop a predictive model for delirium based on precipitating factors, then to validate this model in an independent sample 3.To study the inter-relationship of baseline and precipitating factors for delirium

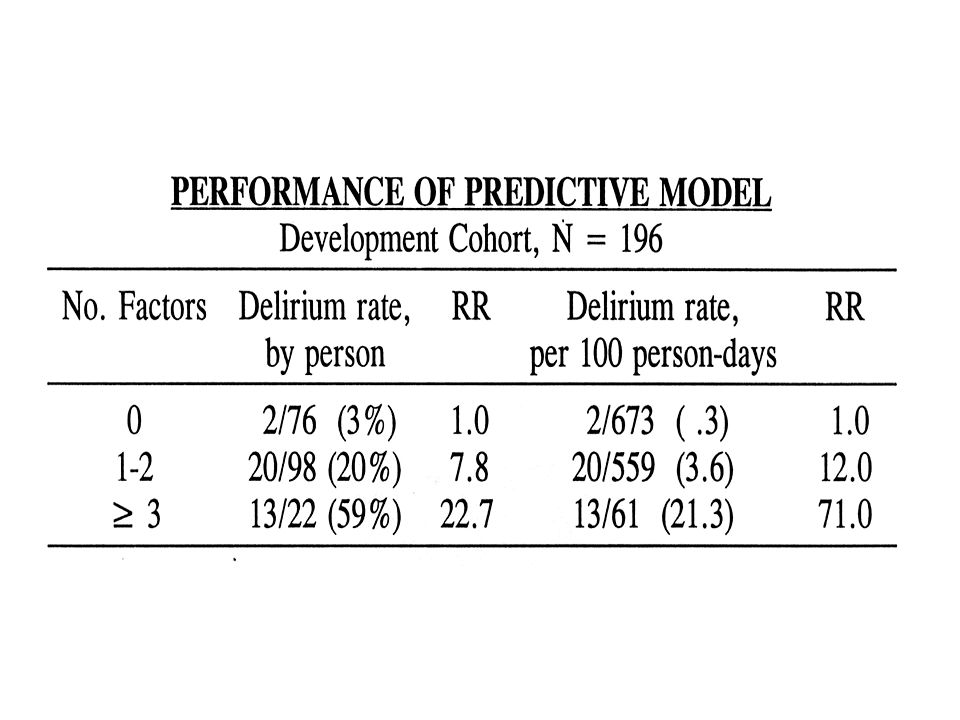
27
METHODS Two prospective cohort studies, in tandem Development Cohort: 11/6/89 – 6/22/90 Validation Cohort: 7/9/90 – 7/31/91 Eligibility: Consecutive patients admitted to the medicine service at Yale-New Haven Hospital Exclusion: Delirium on admission Inability to be interviewed (e.g. intubation, coma) Discharge in < 48 hours Daily patient and nurse interviews
 Discharge in < 48 hours Daily patient and nurse interviews.")
28
DEVELOPMENT OF THE PREDICTIVE MODEL 11 variables entered into stepwise multivariable model 5 independent factors selected for final model

32
IDENTIFICATION OF RISK FACTORS: SIGNIFICANCE Helped determine which risk factors to address Identified patients at high risk for delirium—to target for future preventive efforts Provided groundwork needed for clinical programs and intervention trials

33
MULTIFACTORIAL ETIOLOGY OF COMMON GERIATRICS SYNDROMES Falls Dizziness Incontinence Pressure ulcers Malnutrition Functional decline

34
THE YALE DELIRIUM PREVENTION TRIAL Inouye SK. N Engl J Med. 1999;340:669-76.

35
RISK FACTORS FOR DELIRIUM Cognitive Impairment Sleep Deprivation Immobilization Vision impairment Hearing Impairment Dehydration

36
YALE DELIRIUM PREVENTION PROGRAM Designed to counteract iatrogenic influences leading to delirium in the hospital Multicomponent intervention strategy targeted at 6 delirium risk factors Risk FactorIntervention Cognitive Impairment………………………………..Reality orientation Therapeutic activities protocol Sleep Deprivation……………………………………..Nonpharmacological sleep protocol Sleep enhancement protocol Immobilization………………………………………..Early mobilization protocol Minimizing immobilizing equipment Vision Impairment…………………………………….Vision aids Adaptive equipment Hearing Impairment………………………………….Amplifying devices Adaptive equipment and techniques Dehydration……………………………………………Early recognition and volume repletion

37
RATIONALE FOR MULTICOMPONENT APPROACH Multifactorial etiology Targeted risk factor approach Most effective approach Most clinically relevant approach

38
YALE DELIRIUM PREVENTION TRIAL METHODS Design:controlled clinical trial with individual matching from 3/25/95 – 3/28/98 Subjects:patients ≥ 70 years old without evidence of delirium, but at moderate to high risk for developing delirium. Sample size = 852 (426 intervention, 426 controls) Units:one intervention and 2 control (usual care) units Procedures:baseline, daily, and 1 mo, 6 mo, 12 mo follow-up interviews by trained clinical research staff, blinded to study hypotheses and interventional nature
 Units:one intervention and 2 control (usual care) units Procedures:baseline, daily, and 1 mo, 6 mo, 12 mo follow-up interviews by trained clinical research staff, blinded to study hypotheses and interventional nature.")
40
YALE DELIRIUM PREVENTION TRIAL RESULTS OutcomeIntervention Group (N=426) Usual Care Group (N=426) Matched OR (CI) or p-value Incident delirium, n (%)42 (9.9%)64 (15.0 %).60 (.39-.92) p=.02 Total delirium days No. delirium episodes 105 62 161 90 p=.02 p=.03 Delirium severity score3.93.5p=.25 Recurrence rate13 (31.0%)17 (26.6%)p=.62
17 (26.6%)p=.62.")
41
DELIRIUM PREVENTION TRIAL: SIGNIFICANCE Practical, real-world intervention strategy targeted towards evidence-based risk factors Significant reduction in risk of delirium and total delirium days, without significant effect on delirium severity or recurrence Primary prevention of delirium likely to be most effective treatment strategy Targeted, multicomponent strategy works

42
DELIRIUM HEALTH POLICY IMPLICATIONS Delirium serves as a marker for quality of hospital care for the elderly Often iatrogenic Linked to processes of care Common, bad outcomes Delirium serves as a window for identifying quality – improving changes. Inouye SK. Am J Med. 1999;106:565-73

43
PATHWAYS LEADING TO DELIRIUM Iatrogenesis Failure to recognize delirium Attitudes towards care of the elderly Rapid pace and technologic focus of health care Reduction in skilled nursing staff

44
RECOMMENDED INTERVENTIONS TO REDUCE DELIRIUM LOCAL Cognitive assessment of all older patients Monitoring mental status as a vital sign Strategies to change practice patterns leading to delirium Clinical guidelines/pathways for care of high-risk geriatric patients and delirium Enhanced geriatric nursing and physician expertise at bedside Case management to enhance coordination of care NATIONAL Provider education and continuing education requirements Improved quality monitoring systems; delirium as sentinel event Create environments that facilitate high-quality geriatric care

45
CONCLUSIONS 1.Delirium is a common, serious problem for hospitalized older patients. 2.Recognition may be improved by use of simplified diagnostic criteria. 3.The etiology of delirium is multifactorial, involving vulnerability and precipitating factors. 4.Many cases may be preventable through a targeted risk factor approach. 5.Delirium serves as a quality marker for hospital care.

Similar presentations







: 780–791. 2 Shared risk factors – older age, cognitive.>")



 January 21, 2014 Delirium and Dementia.>")



 Purpose: Provide initial and ongoing screening of patients for identification of signs and symptoms of delirium. Initiate.>")




>")

 Helping to Maintain Cognitive, Physical, and Emotional Well- being in Hospitalized Older Patients.>")