Download presentation
Presentation is loading. Please wait.

1
Polypharmacy in the Elderly
Marc Evans M. Abat, M.D., FPCP, FPSGM Internal Medicine-Geriatric Medicine

2
Objectives Definition of polypharmacy Prevalence Consequences
Pharmacology and Aging Specific Examples Interventions

3
Definitions Polypharmacy
The use of more than 5 medications, some of which may be clinically inappropriate The number may not be as indicative of its presence-all may be appropriate; however the more drugs are taken, the higher are the chances for its occurrence Leads to profound consequences in the elderly population Not enough attention paid to pharmacodynamic principles Regardless of semantics, polypharmacy is widely practiced, often unnecessary and yet sometimes required with the usual multiple medical conditions in the elderly!

4
Prevalence As much as 25% of the overall population (Chumney et al., 2006) For those >65 years old, prevalence increases to 50% 44% males, 56% females 12% of both sexes > 10 drugs per day Prevalence may also be dependent on comorbidity More drugs among diabetics than age or sex matched non-diabetics (Good, 2002) Other predictors include number of starting drugs, CAD, diabetes, and use of medications without indications (Veehof et al. 2000)
 Other predictors include number of starting drugs, CAD, diabetes, and use of medications without indications (Veehof et al. 2000)")
5
Consequences Adverse Drug Reactions (ADRs) which may include:
Drug-drug interactions Drug-disease interactions Drug-food interactions Drug side effects Drug toxicity May increase from 7% in those using 2 drugs to 50% in those using 5 and 100% in those using > 10 (Lin 2003; Brazeau 2001) Drugs that interfere with warfarin and cause increases in INR and bleeding risk! Not appropriately adjusting dosing for renal dysfunction Diet interfering with warfarin levels Drug toxicity especially in drugs with low therapeutic index These are the basic mechanisms by which ADRs occur but the truth is that they Have serious consequences to the elders’ quality of life and society’s pocketbook!
 Drugs that interfere with warfarin and cause increases in INR and bleeding risk! Not appropriately adjusting dosing for renal dysfunction. Diet interfering with warfarin levels. Drug toxicity especially in drugs with low therapeutic index. These are the basic mechanisms by which ADRs occur but the truth is that they. Have serious consequences to the elders’ quality of life and society’s pocketbook!")
6
Up to 30% of elderly hospital admissions involve ADRs
Quality of Life In ambulatory elderly: 35% of experience ADRs and 29% require medical intervention In nursing facilities: 2/3 of residents experience ADRs and 1in 7 of there require hospitalization Up to 30% of elderly hospital admissions involve ADRs Linked to preventable geriatric syndromes This is most common form of iatrogenic illness! Of course ADRs are linked to depression, constipation, falls, morbility, confusion, hip fractures And therefore significantly impaired quality of life! Fick Arch Int Med.

7
Annual cost of $85 billion $76.6 billion in ambulatory care
Economic In 2000: ADRs caused 10,600 deaths Annual cost of $85 billion $76.6 billion in ambulatory care $20 billion in hospitals $4 billion in SNF Fick Arch Int Med.

8
Pharmacokinetics and Aging
characterization and mathematical description of the absorption, distribution, metabolism, and excretion of drugs, their by-products, and other substances of biologic interest as affected by the elderly body Absorption Distribution Metabolism Excretion Absorption: Decreased gastric acid alters absorption of some medications Decreased gastric mobility can increase absorption Distribution: 10-15% decrease in Total Body Water and lean body mass: water soluble drugs have poor distribution in adipose cause increasing serum concentrations Increased body fat: lipid soluble drugs accumulate and prolong duration of action Decreased serum albumin: increases free serum concentrations which makes lab levels more challenging to interrupt Metabolism: Reduced metabolism within the liver and diminished enzyme activity increases serum drug effects Excretion: Diminished kidney function (GFR): calculate creatinine clearance (((140-age) x weight in kg)/72 x serum creatinine) x 0.85 (for women)
: calculate creatinine clearance. (((140-age) x weight in kg)/72 x serum creatinine) x (for women)")
9
Absorption Age-related gastrointestinal tract and skin changes seem to be of minor clinical significance for medication usage Decrease in small intestine surface area Increase in gastric pH Medical conditions (e.g. achlorhydria), other medications or feedings may modify absorption vitamin B12 in atrophic gastritis PPIs with sucralfate Amoxicillin with food
, other medications or feedings may modify absorption. vitamin B12 in atrophic gastritis. PPIs with sucralfate. Amoxicillin with food.")
10
Distribution Age-related changes
Decrease in lean body weight Decrease in total body water(10-15%) Increased percentage body fat (~15-30%) Increased fat:water ratio Decreased plasma proteins, especially albumin Occurrence of heart failure, kidney disease with resulting water retention
 Increased percentage body fat (~15-30%) Increased fat:water ratio. Decreased plasma proteins, especially albumin. Occurrence of heart failure, kidney disease with resulting water retention.")
11
Increase in volume of distribution for lipophilic drugs
sedatives that penetrate CNS Leads to longer half-lives (Linjakumpu 2003) Metabolic capacity of phase I reactions decrease Phase II reactions are largely unaffected Greater, active, free concentration in highly protein-bound drugs
 Metabolic capacity of phase I reactions decrease. Phase II reactions are largely unaffected. Greater, active, free concentration in highly protein-bound drugs.")
12
Concurrent drug use may affect metabolism in both directions
some overall decline in liver metabolic capacity due to decreased liver mass and hepatic blood flow Highly variable, no good estimation algorithm Minimal clinical manifestations Concurrent drug use may affect metabolism in both directions No formula to estimate this effect

13
Age-related decrease in renal blood flow
Renal Elimination Age-related decrease in renal blood flow GFR decreases by 8 mL/min/1.73 m2/decade Decreased lean body mass leads to decreased creatinine production Serum creatinine not reliable Need to estimate creatinine clearance and adjust medications accordingly (i.e. use Cockroft-Gault or MDRD)
")
14
Pharmacodynamics and Aging
Effect of the drug on the body with regard to aging Generally, lower drug doses are required to achieve the same effect with advancing age. Receptor numbers, affinity, or post-receptor cellular effects may change. Changes in homeostatic mechanisms can increase or decrease drug sensitivity.

15
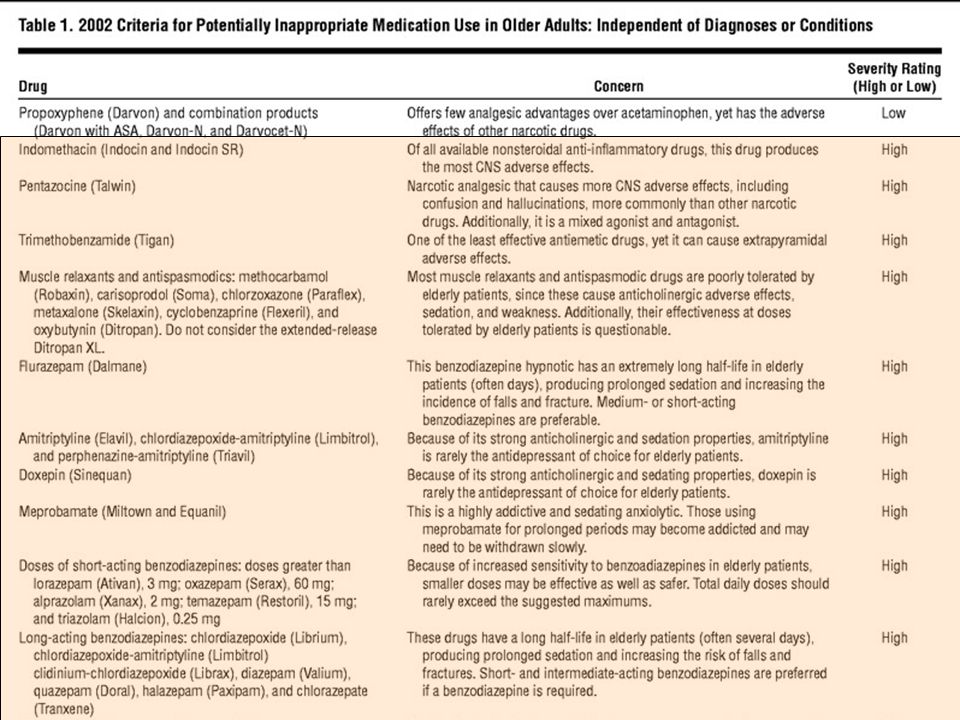
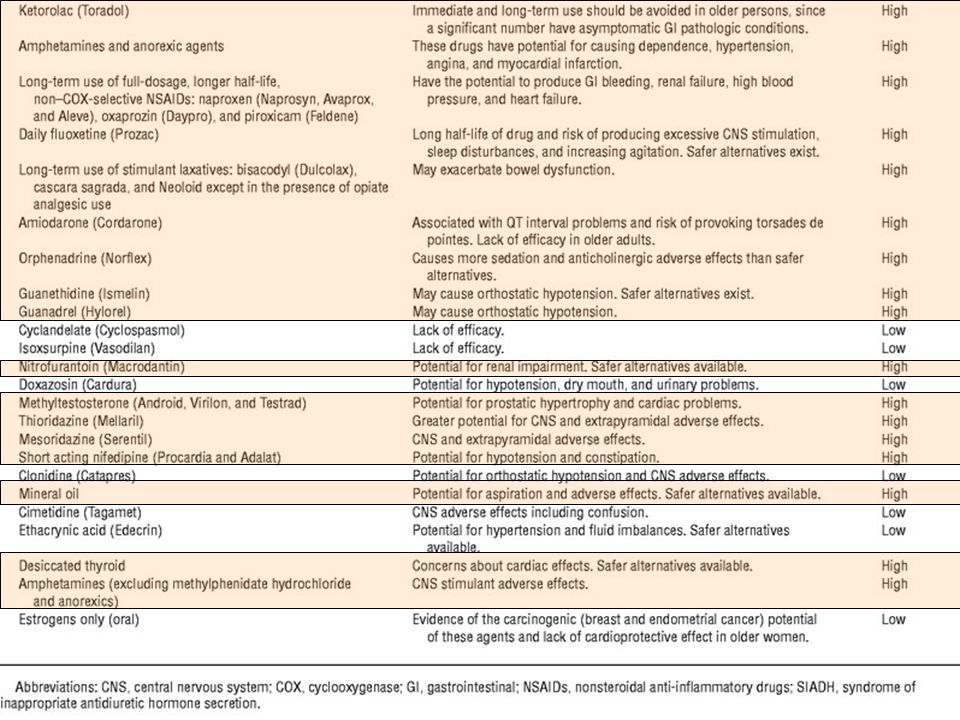
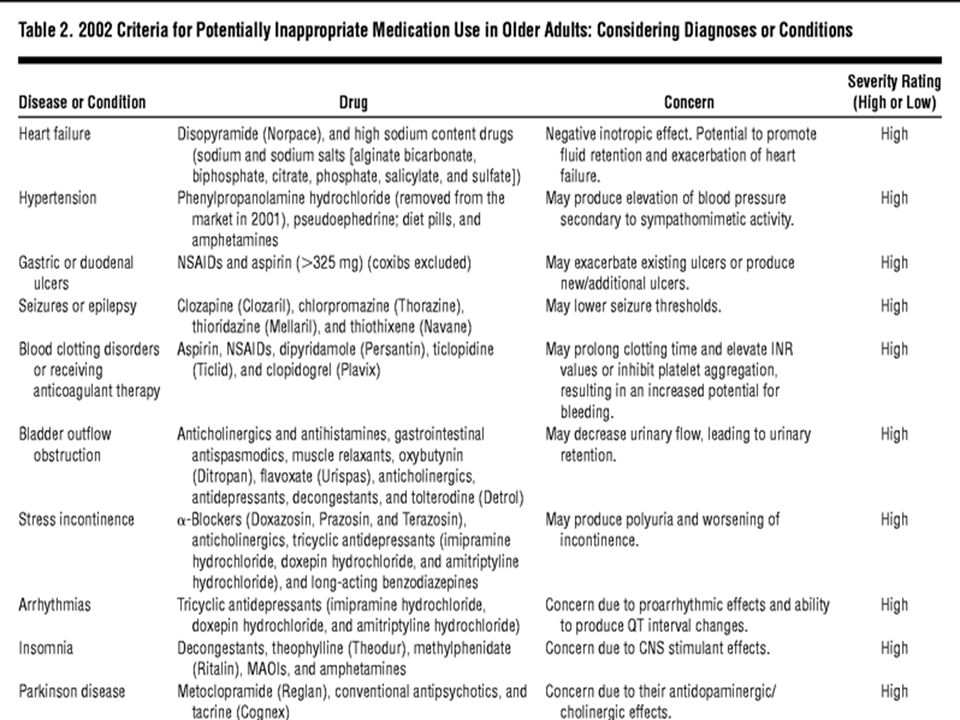
Inappropriate Medications: Beers Criteria
One of the most, if not the widely used consensus data for inappropriate medication use in the elderly Latest revision in 2003 Covers 2 statements regarding drug use in elderly: Those inappropriate for the elderly in general Those inappropriate for the elderly with regard to specific conditions Organized in tables of potentially inappropriate medications both independent of diagnoses and as they are related to certain medical problems. However thinking about this as four main high risk drug categories is easier to remember!

21
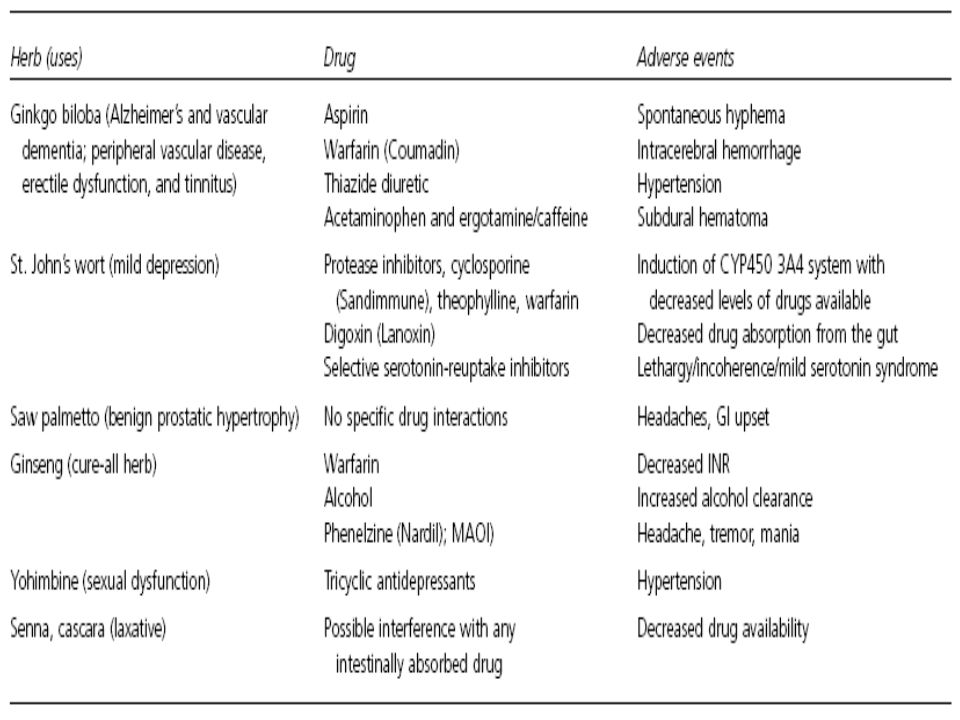
Vitamin and Herbal Use in Older Adults
Highly prevalent among older adults 77% in Johnson and Wyandotte county community dwelling elderly Generally not reported to the physician serious drug interactions possible: Warfarin, gingko biloba, vitamin E

23
Non-adherence to Medication Regimens
related to both physician and patient factors Large number of medications Expensive medications Complex or frequently changing schedule Adverse reactions Confusion about brand name/trade name Difficult-to-open containers Rectal, vaginal, SQ modes of administration Limited patient understanding

24
Geriatric Prescribing Principles
First consider non-drug therapies Match drugs to specific diagnoses Try to give medications that will treat more than condition Reduce meds when ever possible Avoid using a drug to treat side effects of another Review meds regularly (at least q3 months) Avoid drugs with similar actions / same class Clearly communicate with pt and caregivers Consider cost of meds Use these principles to initiate and re-evaluate medications Inherent challenge: the elderly often have very complicated medical conditions which require the use of multiple medications- otherwise the provider feels they are not appropriately treating their patient…. I know hope difficult this challenge can be but If you are aware of the problems with polypharmacy, have a high degree of suspicion for ADRs, and Consider ADRs as a possible etiology of functional decline in elderly patients Then you will improving your pts quality of life! To start doing this, you should be aware of certain high risk medications!
 Avoid drugs with similar actions / same class. Clearly communicate with pt and caregivers. Consider cost of meds. Use these principles to initiate and re-evaluate medications. Inherent challenge: the elderly often have very complicated medical conditions which require the use of multiple medications- otherwise the provider feels they are not appropriately treating their patient…. I know hope difficult this challenge can be but. If you are aware of the problems with polypharmacy, have a high degree of suspicion for ADRs, and Consider ADRs as a possible etiology of functional decline in elderly patients. Then you will improving your pts quality of life! To start doing this, you should be aware of certain high risk medications!")
25
CARE: Avoiding Polypharmamcy
Caution and Compliance Understand side effect profiles Identify risk factors for an ADR Consider a risk to benefit ratio Keep dosing simple- QD or BID Ask about compliance

26
CARE: Avoiding Polypharmamcy
Adjust the Dose Start low and go slow- titrate Consider the pharmacokinetics and pharmacodynamics of the medication

27
CARE: Avoiding Polypharmamcy
Review Regimen Regularly Avoid automatic refills Look for other sources of medications- OTC Caution with multiple providers Don’t use medications to treat side effects of other meds Choose drugs discontinue or substitute safer medications

28
CARE: Avoiding Polypharmamcy
Educate All medicines, even over-the-counter, have adverse effects-report all products used Talk to your patient about potential ADRs Warn them for potential side effects and report symptoms Educate the family and caregiver Ask pharmacist for help identifying interactions Assist your patient in making and updating a medication list- personal medical record Avoid seeing multiple physicians Do not use medications from others This is a simple and obvious idea which is not currently being utilized!

29
Personal Health Record
It will reduce polypharmacy and ADRs Multiple specialist involved in care Transitions in care from independent living, hospitals, nursing homes and assisted living facilities Great aid in emergency care Provides the patient with more piece of mind…

30
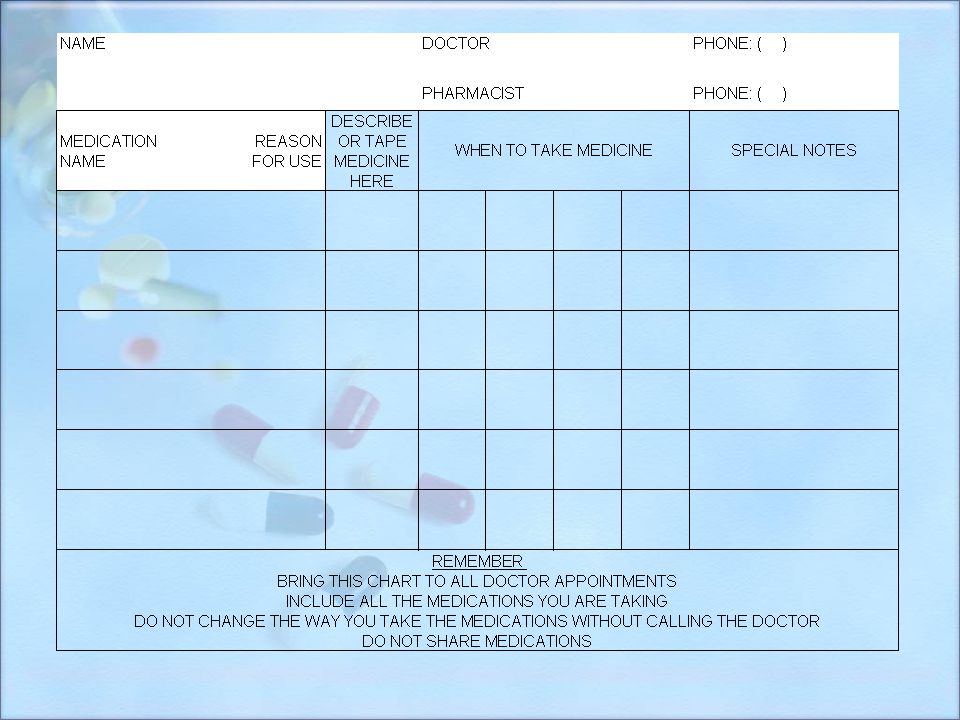
Personal Health Record Includes:
Patient identifying information Doctors contacts Caregiver contacts Past Medical History and Allergies List of all medications, dose, reason they are taking it and whether it is new Now- lets review some key points …

32
Dami pa dapat gawin….

Similar presentations







>")









 : The extent to which the patient adheres to medical advice Patient compliance.>")



