Download presentation
Presentation is loading. Please wait.

1
CLEVELAND ACUTE STROKE EXPERIENCE Cleveland Health Quality Choice –stroke data collected by trained abstractors since 1991 –IV tPA datapoints added 1996 –disbanded 1998 Cuyahoga County Operation Stroke 1999 –data collection instrument designed by the Medical Committee and The Stroke Group (ETHOS R ) grants from Genentech/Astra Zeneca Cleveland Clinic Health System Stroke QI Program –presented to JCAHO 4/01
 grants from Genentech/Astra Zeneca Cleveland Clinic Health System Stroke QI Program –presented to JCAHO 4/01")
2
Cleveland Health Quality Choice IV tPA Utilization: Ischemic Strokes July 1997 - June 1998 n=4275 n=70 tPA 1.8% No tPA 98.2% Katzan IL etal. JAMA 2000;283:1151

3
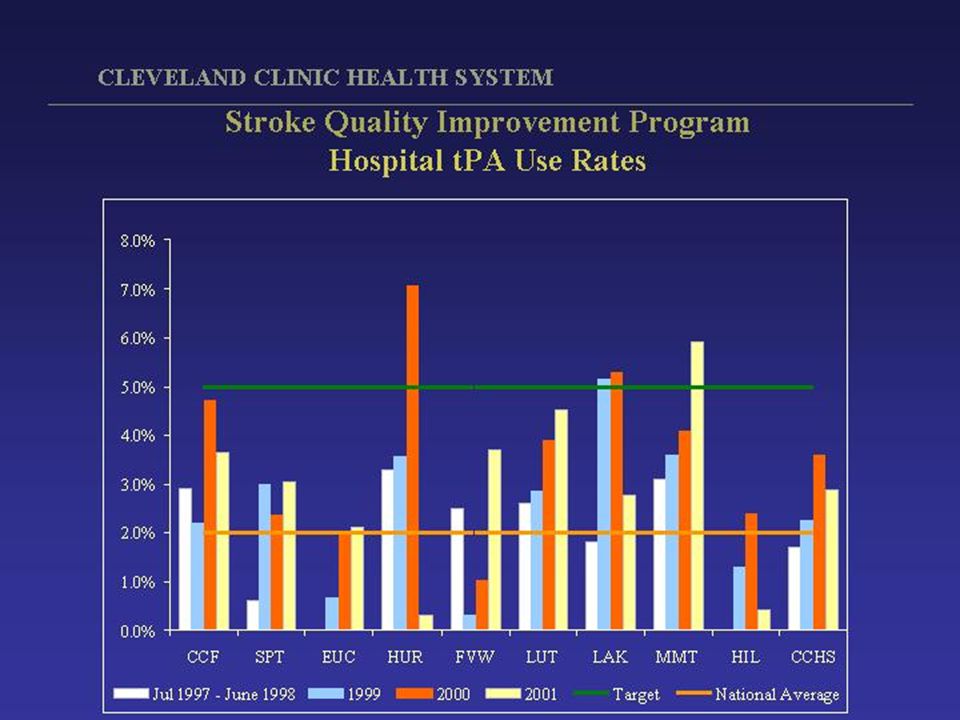
Cleveland Health Quality Choice IV tPA Utilization by Hospital July 1997 - June 1998 Katzan IL etal. JAMA 2000;283:1151 N = 27 (N = 70)
.")
4
Cleveland Health Quality Choice IV tPA Symptomatic Intracranial Hemorrhage (ICH) July 1997 - June 1998 n = 59 n = 11 Symptomatic ICH 15.7%* * 95% CI 8.1% - 26.4% Katzan IL etal. JAMA 2000;283:1151

5
Cleveland Health Quality Choice IV tPA: Identified Protocol Deviations July 1997 - June 1998 Antithrombotics < 24hr 65% Beyond Time Window 22.5% High Blood Pressure 12.5% Katzan IL etal. JAMA 2000;283:1151 Deviations in 50%

6
Intracranial Hemorrhage after IV tPA

7
Connecticut IV tPA experience (Bravata DM etal. Arch Intern Med 2002;162:1994) Retrospective cohort of 16 community based hospitals 5/96-12/98 67% (42/63) major protocol deviations –dosing errors –>3 hours –known increased bleeding risk (eg low platelets) Serious extracranial hemorrhage 17% (NINDS 2%) In-hospital mortality 31% (NINDS 13%)
 Retrospective cohort of 16 community based hospitals 5/96-12/98 67% (42/63) major protocol deviations –dosing errors –>3 hours –known increased bleeding risk (eg low platelets) Serious extracranial hemorrhage 17% (NINDS 2%) In-hospital mortality 31% (NINDS 13%).")
10
Cuyahoga County Operation Stroke Door to Doctor 1/00 - 3/01 (N=65)(N=224)(N=253)(N=65)(N=692)(N=101)(N=59) Katzan IL etal. Stroke 2003 in press

11
Cuyahoga County Operation Stroke Time to Initiation of CT 1/00 - 3/01 (N=56)(N=241)(N=262)(N=53)(N=671)(N=78)(N=58) Katzan IL etal. Stroke 2003 in press

12
Center line = median, box=25-75% quartiles, whiskers=1.5x interquartile range Katzan IL etal. Stroke 2003 in press Cuyahoga County Operation Stroke

14
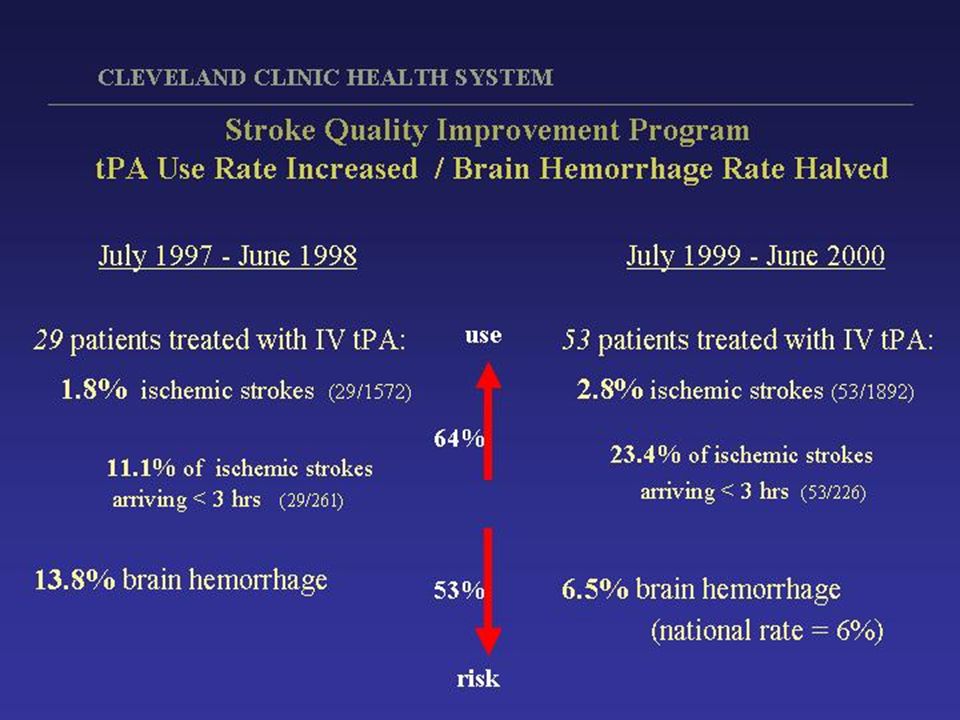
Cleveland Clinic Health System Stroke Quality Improvement Program Symptomatic Intracranial Hemorrhage Symptomatic ICH 13.8%* n=4 No symptomatic ICH 86.2% n=25 *95% CI = 5.5% - 30.6% 7/97-6/98 CHQC

18
CLEVELAND ACUTE STROKE EXPERIENCE Stroke QI requires data –quality of data varies (many hospitals = no data) –multiple barriers must be overcome (behavioral, political, resources) –team building through trust building Performance varies widely across hospitals –physicians and hospitals may not like their data –outliers may not mean bad care –community effectiveness may differ from NINDS efficacy Protocol deviations are very common – linked with bad outcomes Data can change behavior and improve stroke care –community performance improves over time with systematic QI Community hospitals can & should give IV tPA IF they are able to demonstrate they know how
 –multiple barriers must be overcome (behavioral, political, resources) –team building through trust building Performance varies widely across hospitals –physicians and hospitals may not like their data –outliers may not mean bad care –community effectiveness may differ from NINDS efficacy Protocol deviations are very common – linked with bad outcomes Data can change behavior and improve stroke care –community performance improves over time with systematic QI Community hospitals can & should give IV tPA IF they are able to demonstrate they know how")
Similar presentations



















>")



