Download presentation
Presentation is loading. Please wait.

1
“Stereotactic body radiotherapy (SBRT) for early stage lung cancer” 3rd Annual Atlantic Canada Thoracic Oncology Conference October 20-21, 2011 Pier 21, Halifax, NS Gregory M. M. Videtic, MD, CM, FRCPC Associate Professor, Cleveland Clinic Lerner College of Medicine; Section Head for Thoracic Malignancies, Dept. of Radiation Oncology, Taussig Cancer Institute The Cleveland Clinic

2
CONFLICTS OF INTEREST NONE

3
OBJECTIVES To review the nature and the problem of early stage lung cancer To review the standard of care with respect to managing early stage lung cancer To review the principles and practice of stereotactic body radiotherapy (SBRT) as they apply to early stage lung cancer To review SBRT experience at the Cleveland Clinic
 as they apply to early stage lung cancer To review SBRT experience at the Cleveland Clinic")
4
SBRT for Early Lung Cancer: The Cleveland Clinic program Program initiated in 6/04 ~500 medically inoperable early stage NSCLC pts treated to date Some oligometastatic cases (~50) 7 stage I SCLC cases (!)
 7 stage I SCLC cases (!)")
5
A little background first…

6
Epidemiology of Lung Cancer Leading cause of cancer-related deaths worldwide Most common malignancy worldwide over 1 million cases now being diagnosed yearly USA Cancer Statistics 2009 Estimated new cases: 219,440 15% of all new cancer diagnoses Estimated Deaths: 159,390 29% of all cancer deaths (#1 Cancer Killer of Men and Women) Jemal A et al. CA Cancer J Clin. 2009; 59:225

7
INTRODUCTION Definition of Early Stage Non-Small Cell Lung Cancer (NSCLC) Confined to lung, about 15-20% of total cases [30-40,000 cases annually] By TNM staging: IA or IB Thus, No LOCOREGIONAL lymph nodes Standard of care Surgery: 5-year survival 50-70%
![INTRODUCTION Definition of Early Stage Non-Small Cell Lung Cancer (NSCLC) Confined to lung, about 15-20% of total cases [30-40,000 cases annually] By TNM staging: IA or IB Thus, No LOCOREGIONAL lymph nodes Standard of care Surgery: 5-year survival 50-70%](http://images.slideplayer.com/14/4363429/slides/slide_7.jpg "INTRODUCTION Definition of Early Stage Non-Small Cell Lung Cancer (NSCLC) Confined to lung, about 15-20% of total cases [30-40,000 cases annually] By TNM staging: IA or IB Thus, No LOCOREGIONAL lymph nodes Standard of care Surgery: 5-year survival 50-70%")
8
EARLY STAGE Node Negative Lung Cancer Gold Standard Rx = Surgery Time honored position Patient selection - proper staging (pathologic node negative ) - adequate pulmonary reserve - absent or controlled medical problems Effective treatment - impressive local control (65-90%) - overall survival 60-80% at 5 years
 - adequate pulmonary reserve - absent or controlled medical problems Effective treatment - impressive local control (65-90%) - overall survival 60-80% at 5 years")
9
EARLY STAGE LUNG CANCER “Surgical resection remains the gold standard for treatment of patients with stage I and II NSCLC…” Ginsberg RJ & Pot JL. Surgical therapy of stage I and non-T3N0 stage II non-small cell lung cancer. In: “Lung Cancer-Principles and Practice”. Eds. Pass HI et al. Lippincott, Williams and Wilkins, Philadelphia, PA; 2000. p. 691. Mountain CF. Semin. Surg. Oncol. 18:106– 115, 2000. 5-year Overall Survival for stage I NSCLC clinical stage IA-61% vs. pathologic stage IA-67% clinical stage IB-38% vs. pathologic stage IB-57%

10
Randomized Trial of Lobectomy Versus Limited Resection for T1 N0 Non-Small Cell Lung Cancer. Ginsberg and Rubinstein Conclusions Compared with lobectomy, limited pulmonary resection does not confer improved perioperative morbidity, mortality, or late postoperative pulmonary function. Because of the higher death rate and locoregional recurrence rate associated with limited resection, lobectomy still must be considered the surgical procedure of choice for patients with peripheral T1 N0 non-small cell lung cancer.

11
Lung Cancer Study Group Ginsberg, et al. Ann Thorac Surg. 1995 Sep;60(3):615-22
:615-22")
12
How Good is “Gold”? Surgery is a very good but non-perfect treatment NB: path stage I 5- yr OS is “ONLY” 60- 70% Local failures, death from cancer (even controlling for pathological staging) Toxicity, pain and suffering Expense - hospitalization, recovery, lost work/income, etc. Surgery not appropriate for many!
 Toxicity, pain and suffering Expense - hospitalization, recovery, lost work/income, etc. Surgery not appropriate for many!.")
13
INTRODUCTION Many early stage pts [30-50%] potentially resectable but MAY have reasons for being medically inoperable Co-morbidities preventing surgical resection include COPD Cardio-vascular Disease Poor performance status Doing “nothing” is not good in med inop pts McGarry et al. (Chest 2002): Lung cancer cause of death in 53% of 75 stage I medically inoperable pts treated with observation alone
![INTRODUCTION Many early stage pts [30-50%] potentially resectable but MAY have reasons for being medically inoperable Co-morbidities preventing surgical resection include COPD Cardio-vascular Disease Poor performance status Doing nothing is not good in med inop pts McGarry et al.](http://images.slideplayer.com/14/4363429/slides/slide_13.jpg "(Chest 2002): Lung cancer cause of death in 53% of 75 stage I medically inoperable pts treated with observation alone.")
15
EARLY STAGE LUNG CANCER Management of the medically inoperable early lung cancer pt O.S. with primary conventional daily fractionated RT historically poor BUT O.S. with RT confounded by Patient co-morbidities (competing death causes) RT interacting with co-morbidities e.g. COPD exacerbation
 RT interacting with co-morbidities e.g. COPD exacerbation.")
16
3-5 Year Survival in Early Stage Lung Cancer Rx Modality% alive Stage ISurgery60-80% Stage I*Radiotherapy (RT)15-45% Stage IISurgery30-50% Stage II*RT10-30% *clinically staged and mostly medically inoperable *clinically staged and mostly medically inoperable RT generally 60 Gy delivered in 6 weeks
15-45% Stage IISurgery30-50% Stage II*RT10-30% *clinically staged and mostly medically inoperable *clinically staged and mostly medically inoperable RT generally 60 Gy delivered in 6 weeks")
17
“OLD-SCHOOL” RADIOTHERAPY ALONE CAN CURE LUNG CANCER! SELECTION LUCK? “The real reason we use conventionally fractionated RT is in fact because of the normal tissues, not the tumor.” Bob Timmerman, 2007

18
Local Progression-Free Survival Is a Function of Dose ~ 84 Gy would be needed for ~ 50% local progression - free survival in 30 months Mehta M, Manon R. Sem Oncol. 2005;(Suppl 3):s25–s34.
:s25–s34..")
19
87 yo WF, T2 lesion RUL, bx=adenoCA, PET SUV=16.92 at lesion, medically inoperable EBRT 70 Gy/35fx: per plan to the 97% isodose line using 10 MV photons via LAO/POST/RPO field set ups. Pre-RT CT 4/28/04 Post-RT scan of 4/7/10

20
RT and lung cancer The efficacy and safety of RT reflect the interplay between total dose delivered to the malignant tumor the rate of dose delivery (daily fractionation) the volume (and type) of tumor- bearing organ irradiated. The intrinsic tolerance of the tissue irradiated

21
Improving RT Results in the Inoperable Early Lung CA patient Examples of isodose coverage for a patient w/ peripheral stage I lung carcinoma comparing a simple parallel-opposed beam arrangement versus a conformal four-field-technique.. From: Principles and Practice of Radiation Oncology, 4 th edition, C. Perez, L. Brady, E. Halperin and R Schmidt-Ullrich, editors, 2004

24
Spread out the Entrance Dose/focus on the target

25
The origins of lung stereotactic body radiotherapy (SBRT) Modeled after brain radiosurgery principles Multiple convergent beams Rigid patient immobilization Precise localization via stereotactic coordinate system Single fraction treatment Size-restriction for target
 Modeled after brain radiosurgery principles Multiple convergent beams Rigid patient immobilization Precise localization via stereotactic coordinate system Single fraction treatment Size-restriction for target")
26
INTRODUCTION What is SBRT? Technical Multiple convergent beams of RT aimed at target Requires rigid patient immobilization MUST account OR compensate for organ motion Precise localization of target via stereotactic coordinate system Size-restriction for target

27
INTRODUCTION What is SBRT? Technical Typically few-fraction (1 to 5) RT using large individual fraction doses High dose conformality, i.e., “tight around target” Rapid dose fall-off from target to surrounding normal tissue.
 RT using large individual fraction doses High dose conformality, i.e., tight around target Rapid dose fall-off from target to surrounding normal tissue..")
28
Many ways to skin a cat…

29
Use of “Image Guidance”- Technology for frequent 2D and 3D imaging, during RT, to verify/direct radiation therapy checked against the “standard” : Imaging coordinates set by images set at simulation and used for planning INTRODUCTION

30
Treatment Verification Re-align to eliminate error between and during treatment

31
Compact Dose Deposition Pulmonary Vein Bronchus Esophagus Cord Skin Chestwall Lung

32
Lung tumors move with time

33
Lung tumors move in space

34
How do we deal with tumor motion? Solutions (is there just one??) Tumor factors Stop the tumor from moving..somehow Follow the tumor as it is moving and treat as it moves Patient factors Stop the patient from breathing (!) Control the patient’s breathing Machine factors Turn on machine only when it “sees” tumor
 Tumor factors Stop the tumor from moving..somehow Follow the tumor as it is moving and treat as it moves Patient factors Stop the patient from breathing (!) Control the patient’s breathing Machine factors Turn on machine only when it sees tumor.")
36
SBRT and Early Lung Cancer CLINICAL EXPERIENCE Numerous series document efficacy and safety of SBRT in early lung cancer Recent review of rationale, techniques, applications and optimization of SBRT for various extracranial sites (Song et al. Oncology, 2004) -Includes lung cancer (primary/metastatic)
 -Includes lung cancer (primary/metastatic).")
37
SBRT and Early Lung Cancer- Numerous studies report excellent local control.

38
SBRT and Early Lung Cancer- T he radiobiological dose matters, I.e., >100Gy equivalent

39
SBRT and Early Lung Cancer Treatment Toxicities Reported rates generally low > grade 3 pneumonitis, hypoxia: < 5% Related to tumor location RTOG SBRT eligibility Tumors must be at “2 cm or beyond the zone of the proximal bronchial tree” Restriction due to high bronchial injury rates Based on work of Timmerman et al at U Indiana

40
SBRT and Early Lung Cancer Interesting SBRT data from Japan in operable pts who declined surgery (Onishi et al) 5 year survivals for stage IA and IB comparable to surgery Stage IA=77% Stage IB=68%
 5 year survivals for stage IA and IB comparable to surgery Stage IA=77% Stage IB=68%")
41
SBRT for Early Lung Cancer: The Cleveland Clinic program

42
Program initiated in 6/04 ~500 medically inoperable early stage NSCLC pts treated to date Some oligometastatic cases (~50) 7 stage I SCLC cases (!)
 7 stage I SCLC cases (!)")
44
SBRT for Early Lung Cancer: The Cleveland Clinic program PATIENT SELECTION Defined as early stage AND medically inoperable following Review by the Thoracic Multidisciplinary Lung Team Surgeon Pulmonologist Radiation Oncologist Medical Oncologist (Cardiothoracic service/Cardiology) Staging (complete) to include PET +(/-) Mediastinoscopy +(/-) Biopsy- morbidity of procedure of importance
 Staging (complete) to include PET +(/-) Mediastinoscopy +(/-) Biopsy- morbidity of procedure of importance")
45
SBRT for Early Lung Cancer: The Cleveland Clinic program Treatment Regimen Model Uematsu et al. IJROBP 2001; 51:666-670 5 yr. reported experience with Stage I NSCLC 50 patients (medically inoperable / refused surgery) Dose 50-60 Gy / 5-10# /1-2 wks T size 0.8-5.0 cm Staged by CXR, CT chest, no PET, no mediastinoscopy Results: 3 yr o.s. 66% for 50 patients 3 yr o.s. 86% for the 29 medically inoperable patients 3 yr c.s.s. 80% for 50 patients
 Dose Gy / 5-10# /1-2 wks T size cm Staged by CXR, CT chest, no PET, no mediastinoscopy Results: 3 yr o.s. 66% for 50 patients 3 yr o.s. 86% for the 29 medically inoperable patients 3 yr c.s.s. 80% for 50 patients.")
46
SBRT for Early Lung Cancer: The Cleveland Clinic program Treatment Unit Novalis BrainLab System 6MV Linac Special characteristics “Automated image-guided radiation therapy system, utilizes high- resolution X-rays to pinpoint internal tumor sites seconds before treatment, robotically corrects patient set-up errors and tracks any patient movement throughout the treatment, all within a standard treatment time slot”

47
SBRT for Early Lung Cancer: The Cleveland Clinic program SBRT on NOVALIS By restriction (immobilization) By tumor motion studies By creating reference frame to provide real-time verification of patient positioning and set-up
 By tumor motion studies By creating reference frame to provide real-time verification of patient positioning and set-up")
48
SBRT for Early Lung Cancer: The Cleveland Clinic program Novalis patient immobilization BodyFix Stereotactic Immobilizer

49
SBRT for Early Lung Cancer: The Cleveland Clinic program Abdominal compression/breathing restriction

50
SBRT for Early Lung Cancer: The Cleveland Clinic program Abdominal compression/breathing restriction

52
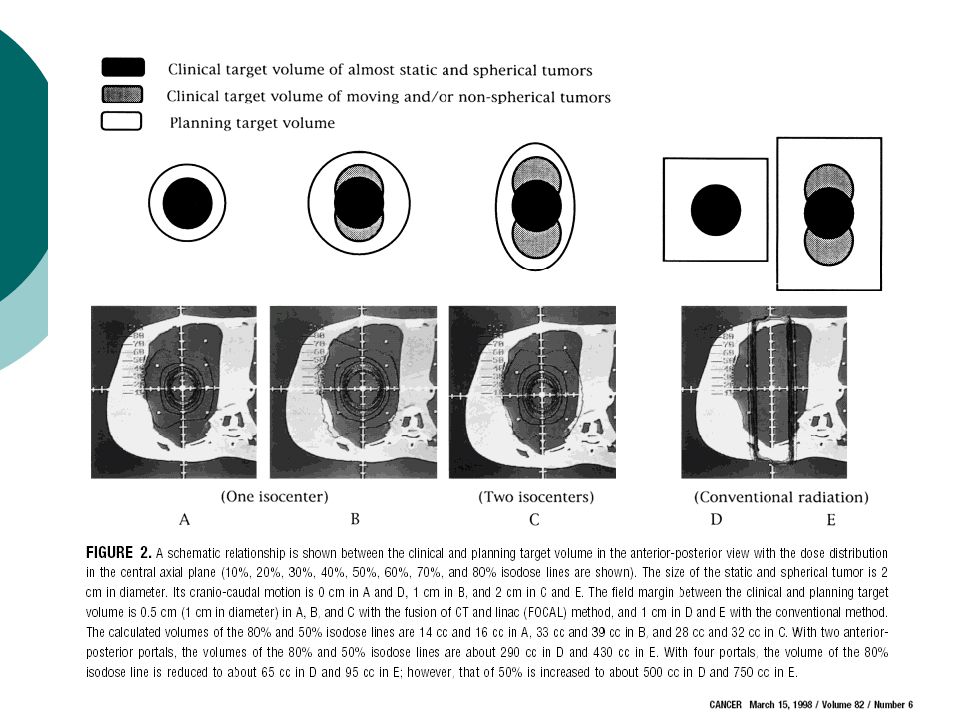
MATERIALS & METHODS CT simulation images acquired at rest, at full inhalation, and at full exhalation were fused to generate an internal gross tumor volume (ITV) that reflected residual motion after external compression CT Sim: Assessment of target motion free breathing, full inhale, and full exhale
 that reflected residual motion after external compression CT Sim: Assessment of target motion free breathing, full inhale, and full exhale")
54
TREATMENT PLANNING

60
SBRT for Lung Cancer: Sample cases from CCF 76 y.o AAF 1992 RUL for CA, 1998 R pneumonectomy with 2 nd CA On chronic O 2 F/U surveillance CT shows new LUL lesion, increasing in size and PET SUVs No biopsy (!) FEV1 32% predicted
 FEV1 32% predicted")
61
2004.10.26- Pre-treat 74 yo AAF RULobectomy 1992 R pneumonectomy 1998 LUL lesion 2004 SBRT 50 Gy/5fx Compl’n 11/19/2004 2009.03.09- 4.5 yrs post-SBRT 2005.10.28- 1 yr post-SBRT

62
SBRT for Early Lung Cancer: The Cleveland Clinic program SBRT administration “In-House” standard Central tumors: 50 Gy in 5 sequential fractions of 10 Gy [Monday through Friday] Peripheral tumors: 60 Gy in 3 fractions [over 8-14 days, min 40 hrs/max 7 days between fractions Selected cases 48 Gy in 4 fractions 60 Gy in 8 fractions 50 Gy in 10 fractions 30 Gy in one fraction
![SBRT for Early Lung Cancer: The Cleveland Clinic program SBRT administration In-House standard Central tumors: 50 Gy in 5 sequential fractions of 10 Gy [Monday through Friday] Peripheral tumors: 60 Gy in 3 fractions [over 8-14 days, min 40 hrs/max 7 days between fractions Selected cases 48 Gy in 4 fractions 60 Gy in 8 fractions 50 Gy in 10 fractions 30 Gy in one fraction](http://images.slideplayer.com/14/4363429/slides/slide_62.jpg "SBRT for Early Lung Cancer: The Cleveland Clinic program SBRT administration In-House standard Central tumors: 50 Gy in 5 sequential fractions of 10 Gy [Monday through Friday] Peripheral tumors: 60 Gy in 3 fractions [over 8-14 days, min 40 hrs/max 7 days between fractions Selected cases 48 Gy in 4 fractions 60 Gy in 8 fractions 50 Gy in 10 fractions 30 Gy in one fraction")
64
SBRT for Early Lung Cancer: The Cleveland Clinic program Follow-up schedule for control and assessment of toxicity 6 weeks,then Q3m for 2 yrs CT chest + contrast Q 3months PFTs/DLCO Q 6months

68
Overall Survival 0 20 40 60 80 100 0612182430364248 Overall Survival (%) Months since Treatment 5x10 3x20 93.9% 83.1%75.9% 90.5% 76.9% 55.5% p=0.68
 Months since Treatment 5x10 3x % 83.1%75.9% 90.5% 76.9% 55.5% p=0.68")
69
Distant Metastasis Free Survival

72
Developing Lung SBRT: An approach to Research Collaborative Group Support RTOG 0236-phase I/II of 60 Gy/3 fx CCF 3 rd highest accruer RTOG 0813-phase I/II- set MTD of SBRT for early-stage, centrally located NSCLC Ongoing, CCF accrual YTD 6 pts RTOG 0915-randomized phase II, peripheral tumors, 34 Gy/1 fraction vs.. 48 Gy/4 fractions, primary end point of toxicity CCF 3 rd highest accruer Roswell Park phase III study of 30 Gy/1 fx vs. 60 Gy/ 3 fx 15 pts accrued YTD

74
Developing Lung SBRT: An approach to Research 1. Establish IRB approved prospective data registry of all SBRT patients 2. Demonstrate efficacy Videtic GMM, Stephans K, Reddy CA, Gajdos S, Kolar M, Clouser E, Djemil T. IMRT-based Stereotactic Body Radiotherapy for Medically Inoperable Early Stage Lung Cancer: Excellent Local Control. Int J Radiat Oncol Biol Phys. 2010; 77:344-349. Stephans KL, Djemil T, Reddy CA, Gajdos SM, Kolar M, Mason D, Murthy S, Rice TW, Mazzone P, Machuzak M, Mekhail T, Videtic GM.A comparison of two stereotactic body radiation fractionation schedules for medically inoperable stage I non-small cell lung cancer: the ClevelandA comparison of two stereotactic body radiation fractionation schedules for medically inoperable stage I non-small cell lung cancer: the Cleveland Clinic experience. J Thorac Oncol. 2009; 4:976-982 Clinic experience.

75
Developing Lung SBRT: An approach to Research 3. Establish acute safety Stephans KL, Djemil T, Reddy CA, Gajdos SA, Kolar M, Mazzone P, Videtic GMM. Comprehensive assessment of Pulmonary Function Test (PFT) Changes after Stereotactic Body Radiotherapy (SBRT) for Stage I Lung Cancer in Medically Inoperable Patients. J Thorac Oncol. 2009; 4:838-844. 4. What about long-term safety? Woody NM, Djemil T, Adelstein DJ, Mason DP, Rice TW, Videtic GMM. Severe Local Toxicity after Lung Stereotactic Body Radiation Therapy (SBRT): Lesional abscess leading to bronchocutaneous fistula requiring surgical marsupialization. J Thorac Oncol. 2010; 5:1874-1875. Stephans KL, Djemil T, Tendulkar RD, Robinson CG, Reddy CA, Videtic GM. Prediction of Chest Wall Toxicity From Lung Stereotactic Body Radiotherapy (SBRT). Int J Radiat Oncol Biol Phys. 2011 Feb 5. [Epub ahead of print]Prediction of Chest Wall Toxicity From Lung Stereotactic Body Radiotherapy (SBRT).
 Changes after Stereotactic Body Radiotherapy (SBRT) for Stage I Lung Cancer in Medically Inoperable Patients. J Thorac Oncol. 2009; 4: 4. What about long-term safety. Woody NM, Djemil T, Adelstein DJ, Mason DP, Rice TW, Videtic GMM. Severe Local Toxicity after Lung Stereotactic Body Radiation Therapy (SBRT): Lesional abscess leading to bronchocutaneous fistula requiring surgical marsupialization. J Thorac Oncol. 2010; 5: Stephans KL, Djemil T, Tendulkar RD, Robinson CG, Reddy CA, Videtic GM. Prediction of Chest Wall Toxicity From Lung Stereotactic Body Radiotherapy (SBRT). Int J Radiat Oncol Biol Phys Feb 5. [Epub ahead of print]Prediction of Chest Wall Toxicity From Lung Stereotactic Body Radiotherapy (SBRT)..")
76
Developing Lung SBRT: An approach to Research 5. Advancing the discipline Burdick MJ, Stephans KL, Reddy CA, Djemil T, Srinivas SM, Videtic GMM. SUVmax from Staging FDG- PET/CT Does Not Predict Treatment Outcome for Early Stage NSCLC Treated with SBRT. Int J Radiat Oncol Biol Phys. 2010 Nov 15;78(4):1033-9. Videtic GM, Stephans K, Woody N, Pennell N, Shapiro M, Reddy C, Djemil T. A Stereotactic body radiotherapy- based treatment model for stage I medically inoperable small cell lung cancer. IASLC- 14th World Conference on Lung Cancer, July 3-7, 2011; Amsteram, The Netherlands. Videtic GM, Reddy C, Sorenson L. Prospective Study of Fatigue and Quality of Life after Stereotactic Body Radiotherapy for Medically Inoperable Early-Stage Lung Cancer. 52nd Annual meeting of ASTRO, October 31- November 4, 2010; San Diego, CA.
: Videtic GM, Stephans K, Woody N, Pennell N, Shapiro M, Reddy C, Djemil T. A Stereotactic body radiotherapy- based treatment model for stage I medically inoperable small cell lung cancer. IASLC- 14th World Conference on Lung Cancer, July 3-7, 2011; Amsteram, The Netherlands. Videtic GM, Reddy C, Sorenson L. Prospective Study of Fatigue and Quality of Life after Stereotactic Body Radiotherapy for Medically Inoperable Early-Stage Lung Cancer. 52nd Annual meeting of ASTRO, October 31- November 4, 2010; San Diego, CA..")
77
Developing Lung SBRT: An approach to Research 5. Advancing the discipline C. Robinson, K. Stephans, C. Reddy, T. Djemil, G. Videtic. Stereotactic Body Radiotherapy (SBRT) for Radiographically Diagnosed Primary Lung Cancer without Histologic Confirmation. 51st Annual Meeting of the American Society for Therapeutic Radiology and Oncology, November 3, 2009; Chicago, IL. Woody NM, Stephans KL, Videtic GMM, Djemil T, Xia P. Defining Target Volume for Lung Stereotactic Body Radiotherapy (SBRT): Fixed or Motion-derived Margins? IJROB. Provisionally accepted.
 for Radiographically Diagnosed Primary Lung Cancer without Histologic Confirmation. 51st Annual Meeting of the American Society for Therapeutic Radiology and Oncology, November 3, 2009; Chicago, IL. Woody NM, Stephans KL, Videtic GMM, Djemil T, Xia P. Defining Target Volume for Lung Stereotactic Body Radiotherapy (SBRT): Fixed or Motion-derived Margins. IJROB. Provisionally accepted..")
78
Developing Lung SBRT: An approach to Research 6. Setting standards Videtic GMM, Stephans KL. The role of stereotactic body radiotherapy in the management of non-small cell lung cancer: An emerging standard for the medically inoperable patient? Curr Oncol Rep. 2010; 12:235-241.

79
Developing Lung SBRT: An approach to Research ASTRO 2011 - Videtic: early experience with single fraction lung radiosurgery - Stephans: bronchial toxicity with SBRT:moving beyond RTOG 0813 parameters -Woody: SBRT outcomes for tumors >4cm - Haque: outcomes for SBRT pts with PET borderline abnormalities in the mediastinum

80
Horizons Single fraction dosing for peripheral tumors? Ideal dose for central tumors Enhanced staging (EBUS?) Slightly more operable patients Treatment of larger tumors Adjuvant chemo? Boost for stage III disease, or recurrence Very limited use for select oligometastatic patients.
 Slightly more operable patients Treatment of larger tumors Adjuvant chemo. Boost for stage III disease, or recurrence Very limited use for select oligometastatic patients..")
82
Conclusions SBRT powerful tool for treating early lung cancer safely and effectively in medically inoperable pts Cancer control rates impressive, likely comparable to surgery Distant control: an area for innovation and investigation, given the nature of the patient population

83
Conclusions Morbidity of treatment strikingly minimal in the acute phase LATE TO VERY LATE TOXICITY: Clearly highlights necessity of long term follow-up (years) Will be critical to define for operable patients
 Will be critical to define for operable patients")
84
Conclusions Current technique for treating pts at CCF with tumor motion control and coverage by SBRT of potential tumor volume safe, tolerable, feasible, rapid Further enhancements in delivery technique being explored Studies in medically operable pts warranted!

Similar presentations

















 is effective, but can be associated with debilitating side.>")



 and N+, chemotherapy should be added.>")





: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")






