Download presentation
Presentation is loading. Please wait.

1
Palliative Potpourri Edward (Ted) St. Godard MA MD CCFP
Robert Pope. “Visitors” Edward (Ted) St. Godard MA MD CCFP Consulting Physician WRHA Palliative Care 1
 St. Godard MA MD CCFP. Consulting Physician. WRHA Palliative Care. 1.")
2
Disclosure I am funded as an independent contractor by the WRHA

3
I. Delirium at end-of-life Name it, claim it, tame it
3

4
objectives At the end of session, participants will
Be able to identify the medical condition known as delirium; Appreciate the importance of this recognition; Have an approach to delirium management

7
Delirium and nurses Nurses are in an optimal position to detect fluctuating symptoms of delirium Agar et al. Palliative Medicine. September, 2011.

8
Delirium and nurses Silent, unspoken piece of nursing practice, impacting on workload Nurses deal with the unpredictable and fluctuating condition of delirious patients, which may be a signal of impending ‘chaos’ Agar et al. Palliative Medicine. September, 2011.

9
Delirium and nurses Under-detection of delirium relates to a lack of knowledge of the criteria for identifying delirium… failure to relay or communicate detected symptoms at onset… Agar et al. Palliative Medicine. September, 2011.

10
What is delirium ? Global cerebral dysfunction “Brain Failure”
Early signs often mistaken as anger, anxiety, depression, psychosis 10

11
Dsm-iv criteria A) Change in consciousness with reduced ability to focus, sustain or shift attention B) Change in cognition (e.g., memory, disorientation, change in language, perceptual disturbance) that is not dementia 11
 Change in cognition (e.g., memory, disorientation, change in language, perceptual disturbance) that is not dementia. 11.")
12
Dsm-iv criteria C) Abrupt onset (hours to days) with fluctuation
D) Evidence of medical condition judged to be etiologically related to disturbance 12
 Evidence of medical condition judged to be etiologically related to disturbance. 12.")
13
Dsm-iv criteria …a disturbance in consciousness with inattention and problems in cognition and/or a disturbance in perception that develop over hours to days with organic causes. 13

14
Delirium vs dementia Delirium Impaired memory Impaired judgement
Impaired thinking Disorientation Dementia Impaired memory Impaired judgement Impaired thinking Disorientation

15
Delirium vs dementia Delirium Abrupt onset Decreased LOC
Sleep/wake cycle Dementia Insidious, progressive Alert, LOC intact Minimal

16
Delirium vs dementia Reversible? PREVENTABLE? Delirium Dementia
Irreversible

17
Delirium is reversible
In up to 50 % of patients with advanced cancer, delirium can be reversed Kang JH et al. “Comprehensive approaches to managing delirium in patients with advanced cancer.” Cancer Treat Rev (2012)
")
18
Reversed vs non-reversed
Lawlor P, Gagnon B, Mancini I, Pereira J, et al. Arch Intern Med 2000 19

19
Delirium sub-types Hypoactive confusion, somnolence, alertness
Hyperactive agitation, hallucinations, aggression Mixed (>60%) features of both
 features of both.")
20
Delirium sub-types Lawlor P, Gagnon B, Mancini I, Pereira J, et al. Arch Intern Med 2000

21
Prevalence/incidence
80 % in medical intensive care units (ICU) 28 % in patients following hip fracture 22 % in general medical inpatients Partridge et al. “The delirium experience: what is the effect on patients, relatives and staff and what can be done to modify this?” Int J Ger Psych. October 2012 (online) 21
 28 % in patients following hip fracture. 22 % in general medical inpatients. Partridge et al. The delirium experience: what is the effect on patients, relatives and staff and what can be done to modify this Int J Ger Psych. October 2012 (online) 21.")
22
Incidence/prevalence
Most frequent neuropsychiatric complication in patients with advanced CA Up to 85 % of patients delirious prior to death Bruera et al. JPSM 2010; 39;2:

23
Incidence/prevalence
~ 42% patients in PC program delirious on admission 50% of episodes reversible “Terminal delirium” in 88 % Lawlor et al. Arch Intern Med 2000; 160:786

24
Impact Palliative sedation requests
Delirium/terminal restlessness (55%) Dyspnea (27%) Pain (18%) Nausea/vomiting (4%) Eisenchlas. Current Opinion in Supportive and Palliative Care 2007, 1:207–212
 Dyspnea (27%) Pain (18%) Nausea/vomiting (4%) Eisenchlas. Current Opinion in Supportive and Palliative Care 2007, 1:207–212.")
25
Impact Palliative sedation requests
Delirium number one reason for requests Fainsinger RL et al. “A multicentre international study of sedation for uncontrolled symptoms in terminally ill patients.” Palliat Med 2000;14:257–65.

26
Impact “We’d rather see dad dead than like this.”
“S/he would be horrified by this.”

27
impact 73/99 patients (74%) remembered delirious episode
Of these, 81 % recalled experience as distressing Family stress > patients’ recalled stress Bruera et al. JPSM 2010; 39;2:

28
impact Interferes with Sx assessment and Tx
Increases morbidity and mortality Hinders communication within families Bruera et al. JPSM 2010; 39;2:

29
Sx difficulty and distress
Pain Dyspnea Delirium 29

30
Sx difficulty and distress
Ax/Tx Challenges Worsening Delirium 30

31
pathophysiology Delirium mediated by failure in central cholinergic transmission? Acetylcholine final common neurotransmitter pathway leading to delirium? White et. al. “First Do no Harm…” JPM. 10 (2); 2007:
; 2007:")
32
pathophysiology Relative acetylcholine deficiency and dopamine excess could mediate the characteristic symptoms of delirium Delirium can be evoked by dopamine agonists and anticholinergic medications Moyer. American Journal of Hospice and Palliative Medicine 28(1), Kang JH et al. Comprehensive approaches to managing delirium in patients with advanced cancer. Cancer Treat Rev (2012)
, Kang JH et al. Comprehensive approaches to managing delirium in patients with advanced cancer. Cancer Treat Rev. (2012)")
33
pathophysiology Dopamine/acetylcholine inverse relationship
Haloperidol first line treatment for delirium Haloperidol D2 antagonist: ? Haloperidol increase levels acetylcholine? White et. al. “First Do no Harm…” JPM. 10 (2); 2007: Kang JH et al. Comprehensive approaches to managing delirium in patients with advanced cancer. Cancer Treat Rev (2012)
; 2007: Kang JH et al. Comprehensive approaches to managing delirium in patients with advanced cancer. Cancer Treat Rev. (2012)")
34
pathophysiology Sometimes successfully treated with dopamine receptor antagonists and possibly by cholinesterase inhibitors High serum anticholinergic activity in patients with delirium Moyer. American Journal of Hospice and Palliative Medicine 28(1),
,")
35
pathophysiology Υ-aminobutyric acid (GABA)-ergic benzodiazepines seem to cause delirium Neuroinflammatory processes drives up-regulation of GABA receptors GABA receptor versus microglial activation versus apoptosis C.G. Hughes et al. “Future Directions in Delirium Management and Research.” Best Practice & Research Clinical Anaesthesiology. 26 (2012) 395–405
 395–405.")
36
causes Precipitating Predisposing

37
causes Predisposing factors: Prevalence increases with age
Male > female Visual impairment Depression White et. al. “First Do no Harm…” JPM. 10 (2); 2007:
; 2007:")
38
causes Predisposing factors: Functional dependence Immobility
Hip fracture Dehydration Alcoholism Stroke Severity of physical illness White et. al. “First Do no Harm…” JPM. 10 (2); 2007:
; 2007:")
39
Who’s predisposed? All of our patients!

40
Fragile? Frail?

41
Fragile? Frail? HANDLE WITH CARE

42
Fragile patients Inverse relationship between the preexisting vulnerability of the patient, and the severity of the insult necessary to precipitate delirium “Knock me over with a feather”

43
Fragile patients Most patients nearing EOL have multiple predisposing factors Most of these are beyond our control

44
causes Precipitating Predisposing

45
Decrease predisposition?
Impractical, given our patient population (frail, usually old) Imperative to minimize precipitating factors
 Imperative to minimize precipitating factors.")
46
precipitators ‘lyte derangements (dehyd’n, hypo/hypernatremia)
Infx (UTI, resp., skin/soft tissue [sacral ulcers]) Metabolic (hyper/hypoglycemia, hypercalcemia, uremia) Low perfusion, hypoxia Withdrawal But what’s missing?
 Metabolic (hyper/hypoglycemia, hypercalcemia, uremia) Low perfusion, hypoxia. Withdrawal. But what’s missing")
47
drugs Anti-cholinergics (Gravol, TCAs, anti-secretories); BZDs Opioids
Steroids Cipro, lasix (?) ranitidine, and on and on…. The list is longer, but are we recognizing any?
 ranitidine, and on and on…. The list is longer, but are we recognizing any")
48
drugs Drug withdrawal: EtOH, Bzd, opioid, “street drugs”

49
Prevention? Prophylactic haldol Prophylactic olanzepine
Prohylactic cholinesterase inhib.s No conclusive literature on meds prophylactically, especially in palliative care, but certain basic “no-brainers.” Gagnon et al. Psycho‐Oncology 21: 187–194 (2012)
")
50
Prevention? Maintain sensorium: hearing aids, eye glasses
Orientation (clocks, calendars, conversation) No conclusive literature on meds prophylactically, especially in palliative care, but certain basic “no-brainers.” Gagnon et al. Psycho‐Oncology 21: 187–194 (2012)
 No conclusive literature on meds prophylactically, especially in palliative care, but certain basic no-brainers. Gagnon et al. Psycho‐Oncology 21: 187–194 (2012)")
51
Prevention? No good evidence for benefit from screening hospitalized patients No conclusive literature on meds prophylactically, especially in palliative care, but certain basic “no-brainers.” Greer N et al. Delirium: screening, prevention, and diagnosis – a systematic review of the evidence 2011 Internet.

52
Prevention? “Cured yesterday of her disease, she died last night of her doctor.” paraphrasing Jonathon Swift (you know, Gulliver’s Travels) No conclusive literature on meds prophylactically, especially in palliative care, but certain basic “no-brainers.”
 No conclusive literature on meds prophylactically, especially in palliative care, but certain basic no-brainers.")
53
Dr. Dr. Drugs drugs Medication sole precipitant of delirium in 12 – 39 % healthy patients Alagiakrishnan et al. Postgrad Med J, 2004; 88: 53

54
Drugs Drugs drugs Drug toxicity, drug withdrawal Start low, go slow
Very often, less is more

55
Prevention? Analgesics: Uncontrolled pain is risk factor for delirium
“Rome wasn’t built in a day” Balance pain against dose Titrate gently

56
Prevention? Analgesics: Titrate gently Don’t be afraid to decrease

57
Sx difficulty and distress
Ax/Tx Challenges Worsening Delirium 57

58
Prevention? Sedatives:
“A benzodiazepine will never help your thinking.” Dr. Mike Harlos

59
Prevention? Lorazepam is an independent risk factor for delirium, increasing risk by ~ 20 % (not to mention falls, etc.) Hold the benzos! Panpharpande et al. Anesthesiology. 2006; 104:21 Kang JH et al. Comprehensive approaches to managing delirium in patients with advanced cancer. Cancer Treat Rev (2012)
")
60
Prevention? Sedatives:
Try not to be the one who starts bzd, but don’t be the one who abruptly stops it Better a tired patient in AM than a delirious patient in AM

61
Prevention? “Anxiety,” “restlessness?” -- how about company? Going for a walk-about? More staff, fewer sedatives, less delirium? Drugs cheap, one-on-one expensive Value?

62
hydration? Does vigorous hydration decrease delirium incidence?
Hyd’n reversed or improved 30 – 70 % delirium cases Thomson et al. Current Op Supp Pal Care. 2009; 3:72-78

63
niciti Name it Claim it Tame it

64
DELIRIUM Name it! “A little fluffy” “Loopy” “A little off”
“Not quite right” “Fruit-cake” DELIRIUM

65
Name it MMSE? CAM? Intuition? Do something; Name it….
When we hear about fluffy patients, assess concentration. Can they name the months of the year backwards? Can they attend to a short conversation? If not, consider them, if not delirious, at high risk of becoming so, and do something…..

66
Name it Change in consciousness with reduced ability to focus, sustain or shift attention Disturbance of consciousness with reduced ability to focus, sustain, or shift attention.

67
Concentrate, focus? Engage in conversation? Months of year backward?
Clinical suspicion Disturbance of consciousness with reduced ability to focus, sustain, or shift attention.

68
Claim it Drs. cause delirium?
Can Drs/nurses prevent it, reverse it, or reduce its impact? Who better?

69
Tame it Two simultaneous pathways Seek and treat cause (thus reverse?)
Manage behaviours (“supportive care”) Human intervention better than pharmacological
 Human intervention better than pharmacological.")
70
Tame it Supportive measures Investigations Hydrate? Avoid restraints
Mobilize Reduce noise, etc. Orient Reassure One-on-one MEDICATION REVIEW Bloodwork U/A Imaging

71
Tame it Meds: Eliminate any psychoactive med possible:
Metoclopramide, cipro? Baclofen? Ranitidine? Lasix? others?

72
Tame it Meds: Analgesia: Good pain control? Consider dose reduction?
Sub-optimal pain control? Opioid rotation

73
Tame it If investigations reveal pathology that can reasonably be thought to be causing delirium; and if the pathology can be treated; and if it is in keeping with goals of care; trial treatment

74
Tame it Does patient behaviour compromise care, or put patient, staff, or others at risk? If “yes,” can a bedside sitter safely help? If “no,” low-dose neuroleptic and/or low-dose bzd

75
Medical management Haloperidol remains standard of care Powerful
Oral and parenteral Limited anti-cholinergic, sedative properties White et. al. “First Do no Harm…” JPM. 10 (2); 2007:
; 2007:")
76
Medical management No significant differences in response in double-blind RCT comparing risperidone and haloperidol Similar evidence finding minimal differences in efficacy between olanzapine and risperidone Bourne et. al. “Drug Treatment of Delirium.” Journal Psychosomatic Research. 65; 2008: Kang JH et al. “Comprehensive approaches to managing delirium in patients with advanced cancer.” Cancer Treat Rev (2012)
")
77
hypoactive Methylphenidate can improve cognitive and psychomotor function in hypoactive delirium Methylphenidate can cause agitation, aggravation, psychosis Bourne et. al. “Drug Treatment of Delirium.” Journal Psychosomatic Research. 65; 2008:

78
Recap Delirium is bad Hard on patients, families, staff
Often preventable, often iatrogenic Nurses optimally located Occasionally reversible

79
Questions/ comments

80
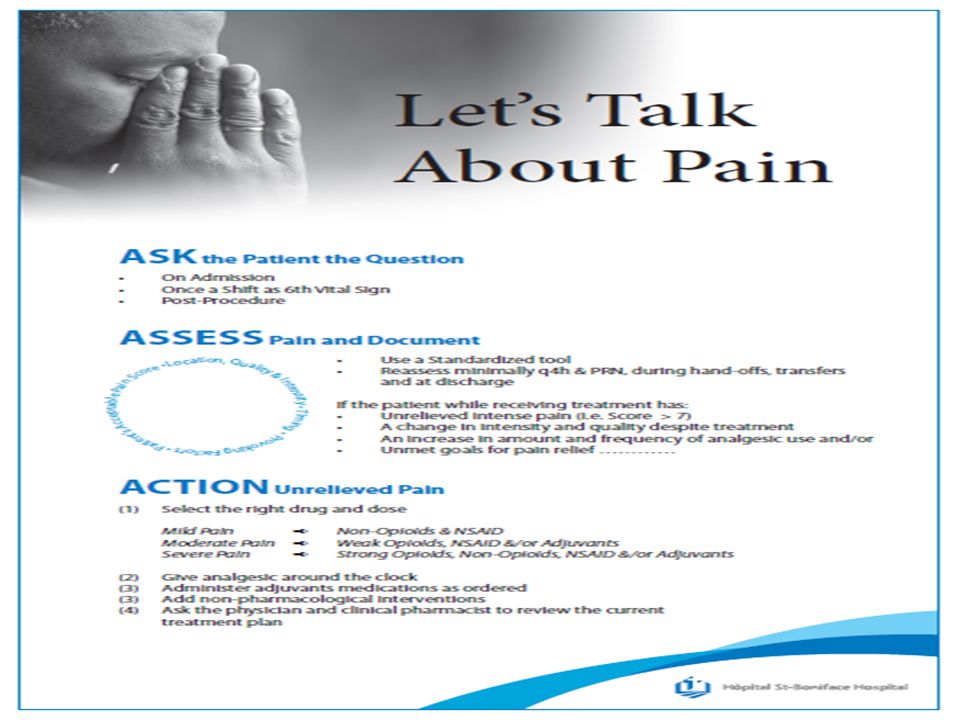
II. Pain

81
objectives At the end of this session, you will
Understand the importance of context in the interpretation of pain Appreciate at a basic level the physiology of pain and some principles of analgesia Have an approach to pain management that always bears in mind the above points

83
11/ % 12/ %

84
Think about pain….

85
Who definition Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.

86
Who the prevention and relief of suffering…..
…by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.

87
Loeser, JD. “Perspectives on Pain
Loeser, JD. “Perspectives on Pain.” Clinical Pharmacology and Therapeutics. Padgham, ed. Baltimore: University Park Press p 314

88
Loeser, JD. “Perspectives on Pain
Loeser, JD. “Perspectives on Pain.” Clinical Pharmacology and Therapeutics. Padgham, ed. Baltimore: University Park Press p 314

89
Multi-disciplinary Team?

91
Pain or Suffering? Both? Neither?

93
What is pain? “…an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.” Merskey H, Bogduk N. 2nd ed Seattle, WA: IASP Press; 1994.

94
What is pain? “…what ever the experiencing person says it is, existing whenever s/he says it does.” Merskey H, Bogduk N. 2nd ed Seattle, WA: IASP Press; 1994. Pain is subjective. It’s what the person experiencing it says it is. Pain confers a survival benefit; we are “hard-wired” to experience it

95
Symptoms in Advanced Cancer
Bruera 1992 “Why Do We Care?” Conference; Memorial Sloan-Kettering

96
Seow H et al. “Trajectory of performance status and symptom scores for patients with cancer during the last six months of life.” J Clin Oncol 2011; 29:1151.

97
Pain is not a diagnosis Pain Classification Nociceptive Neuropathic
visceral somatic neuralgic dysesthetic superficial deep hyperalgesia bony Adapted from Jovey R, 2002

98
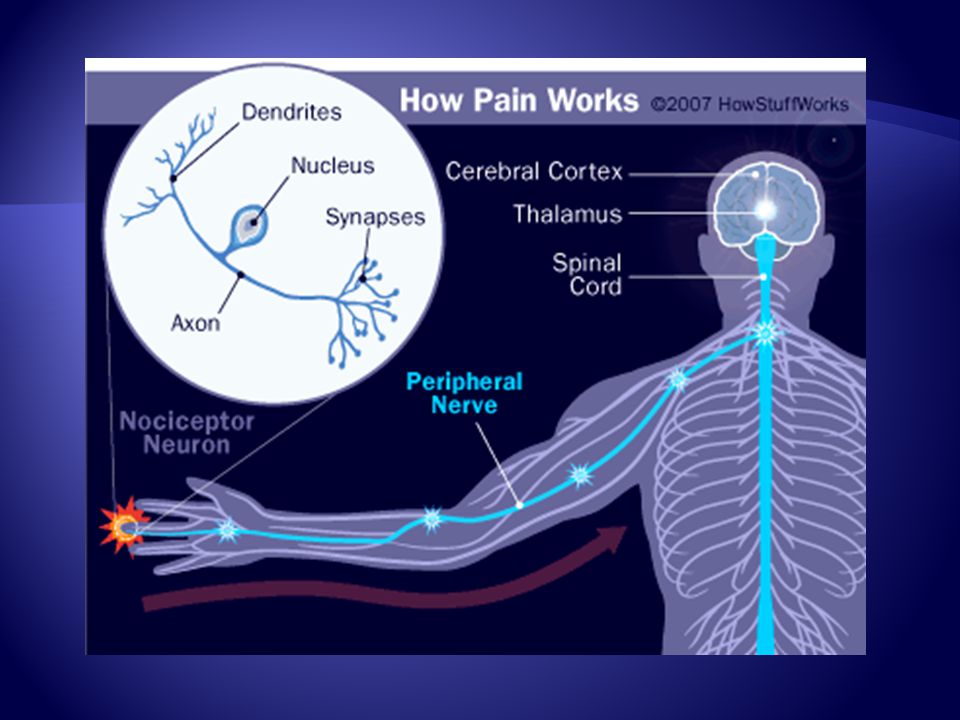
Nociceptors Sensory receptors
Preferentially sensitive to noxious stimuli (tissue damaging/threatening) Chemical, thermal, mechanical
 Chemical, thermal, mechanical.")
99
Somatic Pain Nociceptive Aching, often constant Often worse with mvt
Well localized Tender bone & soft tissue chest wall post-surgery incision

100
Visceral Pain Constant or crampy Dull, aching Poorly localized
Often referred CA pancreas Bowel obstruction Infiltration/compression/distension

101
Neuropathic Pain Pain initiated or caused by primary lesion or dysfunction in the nervous system International Association for the Study of Pain

102
NP Descriptors Burning, Itching, Shooting, Shock-like, Electric, Lancinating “Pins and needles,” tingling, numb

103
NP Descriptors “Pins and needles,” tingling, numb

104
Tx of Neuropathic Pain Pharmacologic treatment
Anticonvulsants – gabapentin, pregabalin TCAs (esp. if depression) NMDA receptor antagonists: ketamine, dextromethorphan, methadone Steroids Opioids
 NMDA receptor antagonists: ketamine, dextromethorphan, methadone. Steroids. Opioids.")
105
Up to 90% of patients with cancer pain could have their pain alleviated by following the treatment guidelines of the WHO analgesic ladder Fitzgibbon et al. “Parenteral Ketamine as an Analgesic Adjuvant for Severe Pain.” J Pall. Med. 8(1) 2005
")
106
Adjuvant Rx may be added at any step
WHO Analgesic Ladder Strong opioid + Step 2 Weak opioid + Step 1 Severe (7-10) Acetaminophen & NSAIDs Moderate (4-6) Mild pain (0-3) By the clock By the ladder
 Acetaminophen. & NSAIDs. Moderate. (4-6) Mild pain. (0-3) By the clock. By the ladder.")
107
Adjuvant Rx may be added at any step
WHO Analgesic Ladder Strong opioid + Step 2 Weak opioid + Step 1 Severe (7-10) Acetaminophen & NSAIDs Moderate (4-6) Mild pain (0-3) By the clock By the ladder
 Acetaminophen. & NSAIDs. Moderate. (4-6) Mild pain. (0-3) By the clock. By the ladder.")
108
Pharmacology Review TOXIC Serum [ drug ] Therapeutic Sub-therapeutic
Single dose, prn usage Sub-therapeutic Time
![Pharmacology Review TOXIC Serum [ drug ] Therapeutic Sub-therapeutic](http://slideplayer.com/slide/4341643/14/images/108/Pharmacology+Review+TOXIC+Serum+%5B+drug+%5D+Therapeutic+Sub-therapeutic.jpg "Single dose, prn usage. Sub-therapeutic. Time.")
109
Pharmacology Review TOXIC Serum [ drug ] Therapeutic Sub-therapeutic
multiple dose, prn usage Sub-therapeutic Time
![Pharmacology Review TOXIC Serum [ drug ] Therapeutic Sub-therapeutic](http://slideplayer.com/slide/4341643/14/images/109/Pharmacology+Review+TOXIC+Serum+%5B+drug+%5D+Therapeutic+Sub-therapeutic.jpg "multiple dose, prn usage. Sub-therapeutic. Time.")
110
Pharmacology Review TOXIC Serum [ drug ] Therapeutic Sub-therapeutic
Idealized “by-the-clock” results Sub-therapeutic 4 hours 4 hours 110
![Pharmacology Review TOXIC Serum [ drug ] Therapeutic Sub-therapeutic](http://slideplayer.com/slide/4341643/14/images/110/Pharmacology+Review+TOXIC+Serum+%5B+drug+%5D+Therapeutic+Sub-therapeutic.jpg "Idealized by-the-clock results. Sub-therapeutic. 4 hours. 4 hours")
111
PRN alone rarely adequate; Long-acting formulations usually not appropriate until symptoms well-managed Continuous source of pain requires continuous analgesia

113
Life in the Bloodstream

118
Poor pain control? Think about drug, dose, route

119
Deteriorating condition
Steady decline at home Accelerated deterioration begins, pain worsening, pt. admitted, medications changed Rapid decline due to illness progression with diminished reserves What’s the best approach? Proactive, tell them that of course you wondered about the meds, of course you’ve reviewed med changes, med usage. HOPEFULLY, you’ve pre-emptively given them a bit of warning that the meds may precipitate somnolence, and, more importantly, that there likely will be fairly significant deterioration to come. Then they’re not so surprised, ambushed. But don’t be defensive. Consider adjusting meds further? Family thinking what?

120
Every family is the Addams family

122
??????? Too much medication Not enough….

123
“It’s all the morphine you’re giving her…..”

124
“it’s the drugs” Popular misconception held by families, lay public, and professionals They’re grasping at straws.

125
“it’s the drugs” “’By the way, palliative care shortens your life,’ [xxxx] suggested.” They’re grasping at straws.
![it’s the drugs ’By the way, palliative care shortens your life,’ [xxxx] suggested. They’re grasping at straws.](http://slideplayer.com/slide/4341643/14/images/125/it%E2%80%99s+the+drugs+%E2%80%99By+the+way%2C+palliative+care+shortens+your+life%2C%E2%80%99+%5Bxxxx%5D+suggested.+They%E2%80%99re+grasping+at+straws..jpg "it’s the drugs ’By the way, palliative care shortens your life,’ [xxxx] suggested. They’re grasping at straws.")
126
“it’s the drugs” “Increasing overall opioid dosage was associated with improved survival compared with no change or decreasing overall dosage (mean survival days versus versus , days respectively, P 5 .01).” They’re grasping at straws. Azoulay et al. “Opioids, Survival, and Advanced Cancer in the Hospice Setting.” J Am Med Dir Assoc. Feb. 2011; 12:
. They’re grasping at straws. Azoulay et al. Opioids, Survival, and Advanced Cancer. in the Hospice Setting. J Am Med Dir Assoc. Feb. 2011; 12:")
127
“it’s the drugs” “Opioid usage, even at high dosages, had no effect on survival among advanced cancer patients in a hospice setting.” They’re grasping at straws. Azoulay et al. “Opioids, Survival, and Advanced Cancer in the Hospice Setting.” J Am Med Dir Assoc. Feb. 2011; 12:

128
“it’s the drugs” “Among patients with metastatic non–small-cell lung cancer…, As compared with patients receiving standard care, patients receiving early palliative care had less aggressive care at the end of life but longer survival.” They’re grasping at straws. Temel et al. “Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer.” N Engl J Med. 2010; 363:

129
Bruera et al. J Pain Symptom Manage. 1990; 5:341-344
Sub-Q Morphine Bruera et al. J Pain Symptom Manage. 1990; 5:

130
A Patient 64 woman resents to ED with “severe” pain;
Hydromorph Contin 24 mg PO bid; Hydromorphone IR 6 mg Q1H prn, taking “several” times daily; “Confused” per family

131
A Patient Pain “everywhere”;
Poor historian, “muddled,” family report fairly rapid escalation of opioids past 3-4/7; O/E: vitals unremarkable, dry MM, decreased BS R>L, no adventitia, normal HS. Very tender over R rib cage (without compressing), abdo benign, DTR unremarkable, no tremors or twitches;
, abdo benign, DTR unremarkable, no tremors or twitches;")
132
A patient ACP “M”; B/W shows creatinine increased from previous, at 195, dry, corrected Calcium 2.5; U/A benign; CXR no obvious rib fractures; AXR abundant stool, no a/f levels, no free air

133
A few red flags…. Pain “everywhere” (pathophysiology?);
Family report fairly rapid escalation of opioids past 3-4/7; Poor historian, “muddled”; Creatinine up

134
Opioid-Induced Neurotoxicity (OIN)
Potentially fatal neuropsychiatric syndrome of: Cognitive dysfunction Delirium Hallucinations Myoclonus/seizures Hyperalgesia / allodynia Early recognition is critical

135
pathophysiology

136
Normal Renal Fcn Renal Insufficiency
Osborne et al. “The Pharmacokinetics of morphine and morphine glucuronides in Kidney Failure.” Clin Pharmacol Ther 54: , 1993

137
Misinterpreted as Pain Misinterpreted as Disease-Related Pain
Opioid-Induced Neurotoxicity (OIN) Opioid tolerance Mild myoclonus (eg. with sleeping) Severe myoclonus Seizures, Death Delirium Agitation Misinterpreted as Pain Opioids Increased Hyperalgesia Misinterpreted as Disease-Related Pain Opioids Increased We should be more clear with our definitions.
 Opioid tolerance. Mild myoclonus (eg. with sleeping) Severe myoclonus. Seizures, Death. Delirium. Agitation. Misinterpreted as Pain. Opioids Increased. Hyperalgesia. Misinterpreted as Disease-Related Pain. Opioids Increased. We should be more clear with our definitions.")
138
Oin: Treatment Switch opioid (rotation) and/or reduce dose Hydrate
Bzd prn?

139
Short Re-cap Not everyone has pain ;
Treating pain with scheduled opioids is appropriate and safe; Avoid long-acting formulations;

140
Short Re-cap Watch out for pain that “doesn’t make sense,” as it might be warning you of OIN Pain and suffering are distinct, and not always related as closely as we think 140

141
PAIN

142
POSSIBLE

143
Suffering?

144
III. Dyspnea

145
Objectives At the end of the session, you will
Have a basic understanding of respiration Be aware of the complex mechanisms underlying dyspnea Have an approach to the management of dyspneic patients 145

146
Dyspnea “Subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity.” Under normal circumstances, we are not aware of our breathing American Thoracic Society. “Dyspnea: Mechanisms, Assessment, and Management, a Consensus Statement.” Am J Respir Crit Care Med. 1999; 159: 146

147
Dyspnea Tachypnea ≠ dyspnea
Physical and emotional components (anxiety, panic, chronic fear) Often no measurable physical correlates (RR ? SaO2 ? ABG) Tachypnea ≠ dyspnea
 Often no measurable physical correlates (RR SaO2 ABG) Tachypnea ≠ dyspnea.")
148
Dyspnea Universal response is to decrease activity to whatever degree necessary Dudgeon, D. “Managing Dyspnea and Cough.” Hematology/Oncology Clinics of North America. 2002; 16:

149
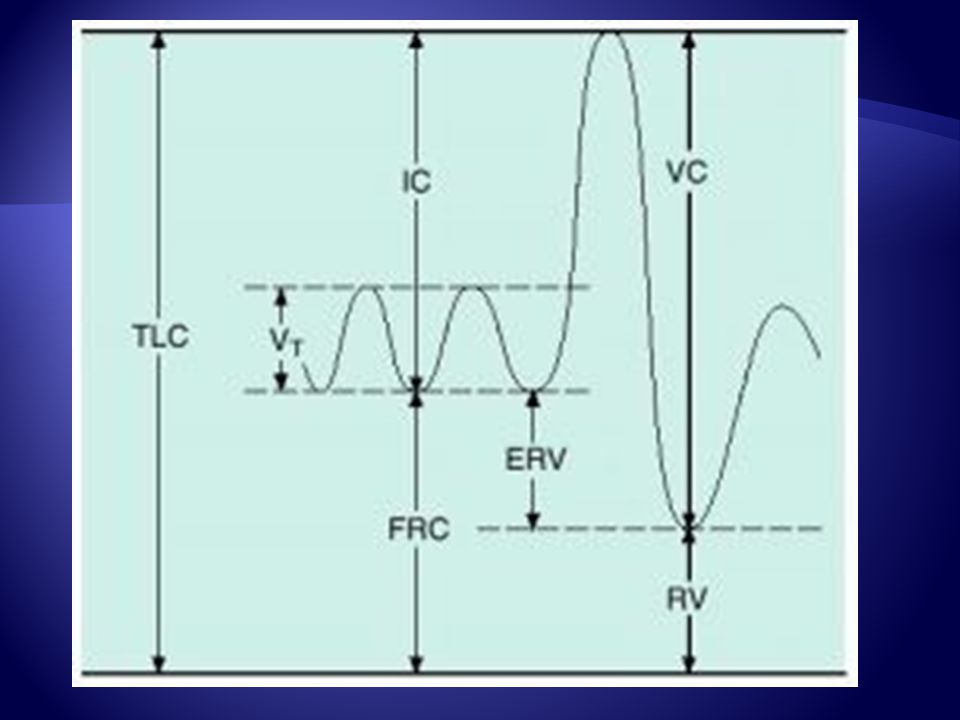
Which pattern shows dyspnea?
B C D

150
Dyspnea “Subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity.” Under normal circumstances, we are not aware of our breathing American Thoracic Society. “Dyspnea: Mechanisms, Assessment, and Management, a Consensus Statement.” Am J Respir Crit Care Med. 1999; 159: 150

151
Time till death Without eating Months Without drinking Days
Without breathing Months Days Minutes We can go a long time without eating, a fairly long time without drinking, but a very short time without breathing. Therefore, if our bodies perceive threats in any of these domains, there will be a proportional response. Deranged blood gases, and/or perceptions that the current respiratory status is unsustainable, will lead to very significant “concern” on the part of the organism. 151

152
Dyspnea Dyspnea, like pain, is protective. As pain alerts us to actual or impending tissue damage, dyspnea alerts us to threat. “Hardwired” to protect 152

153
Dyspnea 60 % lung Ca patients Nearly 90 % once near death
50 % described dyspnea as severe Muers MF, Round CE. “Palliation of symptoms in non-small cell lung cancer: a study by the Yorkshire Regional Cancer Organization thoracic group.” Thorax 1993;48:339– 43.

154
Dyspnea Reuben DB, Mor V. “Dyspnea in terminally ill cancer patients.” Chest. 1986; 89(2):
:")
155
Dyspnea Abnormality of blood gases, especially hypercapnia (PaCO2 > 50 mmHg) and, to a lesser extent, hypoxia (PaO2 < 60 mmHg); Amount of work that must be performed by respiratory muscles to provide adequate ventilation; State of mind. Guyton and Hall. Textbook of Medical Physiology. 491

156
Dyspnea Under normal circumstances, we are not aware of our breathing

157
Mahler. “Understanding Mechanisms …Dyspnea
Mahler. “Understanding Mechanisms …Dyspnea.” Current Opinion in Supportive and Palliative Care .2011, 5:71–76

158
CNS Integrates information about: Degree of effort required
Mechanical response achieved O2/CO2 pH status In order to answer two questions:

159
CNS Is the mechanical response normal relative to the degree of effort expended? Is the current effort sustainable? If not, dyspnea

160
Dyspnea Dyspnea occurs when there is a mismatch between ventilation and the demand set by chemical drive Under normal circumstances, we are not aware of our breathing Buchanan and Richerson. “Role of Chemoreceptors in Mediating Dyspnea.” Respiratory Physiology and Neurobiology. 2009; 167: 9 – 19

168
Oxygen Carbon Dioxide CO2 + H2O HCO3- + H+

169
Complex monitoring With each heartbeat the blood passes through the medulla, where molecular watchmen pay attention to the various gases.

170
Complex monitoring If O2 drops, or CO2 rises, the watchmen hit the alarm bell, telling the organism to breathe harder, deeper, and to be afraid, to panic

171
A dyspneic patient Tachypneic? Hypoxic? Anxious/afraid? Diaphoretic?
Unconscious?

172
Dyspnea “Subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity.” Under normal circumstances, we are not aware of our breathing American Thoracic Society. “Dyspnea: Mechanisms, Assessment, and Management, a Consensus Statement.” Am J Respir Crit Care Med. 1999; 159: 172

173
Approach to Dyspnea Assess the symptom Determine the cause
Treat the cause Treat the symptom

174
As is the case with all sx, here is an algorithm

175
Assess the symptom Remember: Tachypnea is not dyspnea;
Assess distress, not just apparent intensity

176
Determine the cause Thoracic Extra-thoracic Non-malignant Malignant
Paramalignant Extra-thoracic Cachexia; Anemia; Ascites; Hepatomegaly ‘Lyte derangement

177
Treat the cause Anti-tumour: chemo/RT, etc. Infection CHF SVCO
Pleural effusion Pulmonary embolism Airway obstruction

178
Treat the Symptom Goal of interventions:
Minimize production of symptom (pre-medicate, energy mgmt., breathing techniques) Diminish perception of symptom (meds, fan, distraction)
 Diminish perception of symptom (meds, fan, distraction)")
179
Treat the Symptom Goal of interventions:
Modify the experience of the symptom (address meaning, help with mood/fear/anxiety)
")
180
Dyspnea Therapy Non-pharmacological Open window?
Cool facial stimulation (fan) Positioning Pulmonary rehab?
 Positioning. Pulmonary rehab")
181
Dyspnea Therapy Pharmacological Oxygen Opioids Nebulized furosemide
Anti-inflammatory tx Benzodiazepines?

182
Oxygen? Bruera 1993 14 dyspneic, hypoxic (SaO2 < 90%) cancer inpatients RCT, 2 x blind, placebo, crossover 5 L/min air by NP vs O2 no ∆ in VAS from baseline with air, significant improvement with O2 Bruera et al. Lancet. 1993; 342:

183
Oxygen? Bruera 1993 Conclusion: O2 substantial benefit in hypoxic dyspneic cancer patients Bruera et al. Lancet. 1993; 342:

184
Oxygen? Bruera 2003 33 dyspneic, non-hypoxic cancer pts
RCT, single blind, placebo, cross-over 5 l/min air vs O2 for 6 MW test No difference in dyspnea, fatigue, or distance walked Bruera et al. Pall Med. 2003; 17:

185
Oxygen? Bruera 2003 Conclusion: O2 of no benefit over air to exercising non-hypoxic cancer pts Bruera et al. Pall Med. 2003; 17:

186
Oxygen? O2 no better than air in non-hypoxic patient
O2 better than air if hypoxic

187
Oxygen in COPD? Normal COPD O2 CO2 Resp. Drive O2 CO2 Resp. Drive
Under normal circumstances, our respiratory drive is controlled by CO2. As CO2 rises, so does our drive to breathe, O CO2 Resp. Drive O CO2 Resp. Drive

188
Oxygen in COPD? COPD O2 CO2 Resp. Drive
In a certain percentage of COPD patients, their CO2 is chronically high, so their respiratory drive is controlled by dropping O2. That is, as O2 drops, resp. drive increases. In these patients, giving O2 can decrease resp. drive. O CO Resp. Drive

189
Oxygen in COPD? Giving pts. with COPD supplementary O2 can actually suppress their resp. drive (and kill them with kindness)
 .")
190
Anxiolytics? Anxiety is significantly correlated with intensity of dyspnea Limited evidence supporting BZD role Bruera, E. et al. “The Frequency and Correlates of Dyspnea in patients with Advanced Cancer.” J Pain Symptom Mgmt. 2000; 19:

191
“Milk of the poppy…”

192
Opioids? Used for analgesia for centuries
Used since at least 19th century for breathlessness Now a degree of reticence

193
Opioids? Naloxone versus saline in exercising COPD patients;
Naloxone group more dyspnea; Endogenous opioids blunt dyspnea Mahler DA, Murray JA, Waterman LA, Ward J, Kraemer WJ, Zhang X, Baird JC: “Endogenous opioids modify dyspnoea during treadmill exercise in patients with COPD.” Eur Respir J 2009; 33:771.

194
Opioids? Cochrane: 18 RDBPC crossover trials 9 nebulized, 9 systemic, 14 single dose Primarily COPD Conclusion: significant benefit for systemic, but not for nebulized opioids Jennings et al. “Opioids for the Palliation of Breathlessness in Terminal Illness.” Cochrane. Database of Systemic Reviews. 2001

195
Opioids? Early use of opioids may prolong survival, by reducing physical and psychological distress Twycross, R. “Morphine and Dyspnea.” Pain Relief in Advanced Cancer. New York: Churchill Livingston,

196
Opioid mechanism? ↓ Medullary sensitivity/response to hypercarbia/hypoxia ↓ Cortical resp. awareness ↓ Metabolic rate/ventilatory demand Vasodilation (improved cardiac fcn) Analgesia: ↓ pain-induced resp. drive Anxiolysis
 Analgesia: ↓ pain-induced resp. drive. Anxiolysis.")
197
Opioid mechanism? With each heartbeat the blood passes through the medulla, where molecular watchmen pay attention to the various gases.

198
Opioid mechanism? If O2 drops, or CO2 rises, the watchmen hit the alarm bell, telling the organism to breathe harder, deeper, and to be afraid, to panic

199
Opioid mechanism? Opioids tell the watchmen to allow for broader derangements in the blood gases, and to hit the alarm bell with less force when they need to hit it

200
Opioids? Narrow therapeutic index Watch: Rate of dose change
Previous exposure? Bruera, E. “Effects of Morphine on Dyspnea.” J Pain Symptom Mgmt. 1990; 5: 341-4

201
Excessive opioids Pinpoint pupils
Gradual slowing of the respiratory rate Breathing is deep (though may be shallow) and regular
 and regular.")
202
“it’s the drugs” “…fear has been shown to be largely unfounded. Examining changes in respiratory parameters…in dyspneic palliative care patients…demonstrated significant decrease in respiratory rate and improvement in dyspnea with titration with morphine or hydromorphone but no significant changes in other respiratory parameters, indicating no opioid-induced respiratory depression.” They’re grasping at straws. Kamal et al. “Dyspnea Review for the Palliative Care Professional.” J Pall Med. 2012; 15 (1):
:")
203
“it’s the drugs” “…demonstrated benefits, and the lack of edvidence of accelerated death, have led the American College of Chest Physicians…to recommend that physicians titrate oral and/or parenteral opioids” They’re grasping at straws. Kamal et al. “Dyspnea Review for the Palliative Care Professional.” J Pall Med. 2012; 15 (1):
:")
204
Bruera et al. J Pain Symptom Manage. 1990; 5:341-344
Sub-q morphine Bruera et al. J Pain Symptom Manage. 1990; 5:

205
Recap Dyspnea can’t be measured, and often can’t be observed
Oxygen is a drug; balance benefit vs cost ($ and other) Opioids work
 Opioids work.")
206
If you want a wise answer, ask
a reasonable question Goethe Who questions much, shall learn much, and retain much Francis Bacon

207
Our solar system consists of one star, and some debris….
Carl Sagan

Similar presentations
























 January 21, 2014 Delirium and Dementia.>")







