Download presentation
Presentation is loading. Please wait.

1
“Exercise Safely: How Big Is The Risk James W. Ziccardi DO, FACC

2
Pheidippides delivers the news of the victory of the Athenians over the Persians

3
“The condition of the athlete is not natural.” --Hippocrates

4
Over the last several decades there has been a dramatic change in activity levels of the population in their 50’s and older participating in moderate and sometimes high levels of exercise, including marathons. Since cardiac disease risk increases with age, many of these participants will have underlying cardiovascular disease and be at risk for an acute event during or after performing exercise. Patients with known cardiac disease may also be on several medications, the side effects of which may be potentiated by exercise or inhibit obtaining reasonable levels of performance. The potential cardiovascular risk of exercise, especially in reference to endurance events, actions to reduce risk, the potential side effects of cardiac medications and choosing drug regimens hemodynamically favorable to exercise will be reviewed. Over the last several decades there has been a dramatic change in activity levels of the population in their 50’s and older participating in moderate and sometimes high levels of exercise, including marathons. Since cardiac disease risk increases with age, many of these participants will have underlying cardiovascular disease and be at risk for an acute event during or after performing exercise. Patients with known cardiac disease may also be on several medications, the side effects of which may be potentiated by exercise or inhibit obtaining reasonable levels of performance. The potential cardiovascular risk of exercise, especially in reference to endurance events, actions to reduce risk, the potential side effects of cardiac medications and choosing drug regimens hemodynamically favorable to exercise will be reviewed.

5
Cardiac Complications of Endurance Running 1. Acute Mydocardial Infarction 2. Arrhthmia: SVT, AFIB, PVC 3. Sudden Death: VT, V-FIB 4. Hypotension

6
Non-Cardiac Problems Complicating Cardiac Disease 1. Dehydration 1. Dehydration 2. Hyponatremia 2. Hyponatremia 3. Hyperthermia 3. Hyperthermia 4. Hypothermia 4. Hypothermia

7
Risk of Death – Distance Running 1. 10K to ½ Marathon 1. 10K to ½ Marathon Men 38 to 84 Y.O.A. Incidence: 1/327,344(Frere J. 2004) 2. Marathon 2. Marathon 1/50,000 Marine Corp, Twin Cities Marathon 1982 – 1994 4 deaths (3 during race, 15-24 mi.)(Maron B. 1996) 3. Joggers 3. Joggers Rhode Island, 1975-1980. 1 Death/Yr./7,620 Joggers Without known cad. 1/15,240(Thompson P. 1982) 4. Marathon – Post Infarction - Safety 4. Marathon – Post Infarction - Safety 8 Pt. Boston Marathon – No CV Events (4/73) Age 36 to 57(Kavanagh T. 1974)
 2. Marathon 2. Marathon 1/50,000 Marine Corp, Twin Cities Marathon 1982 – 1994 4 deaths (3 during race, mi.)(Maron B. 1996) 3. Joggers 3. Joggers Rhode Island, Death/Yr./7,620 Joggers Without known cad. 1/15,240(Thompson P. 1982) 4. Marathon – Post Infarction - Safety 4. Marathon – Post Infarction - Safety 8 Pt. Boston Marathon – No CV Events (4/73) Age 36 to 57(Kavanagh T. 1974).")
8
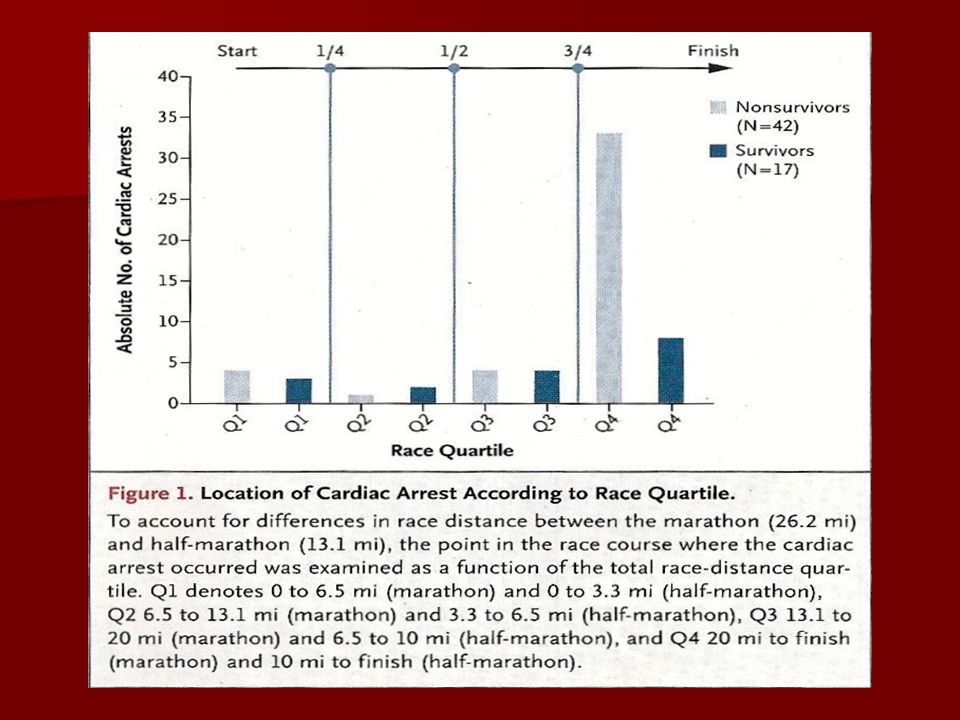
Cardiac Arrests in Long Distance Running Races 10.9 Million Runners, 59 arrests (51 men) 10.9 Million Runners, 59 arrests (51 men) –Ages 43 +/- 13 yrs –Incidence rate =.54/100k Majority Due to CAD 1.01 per 100k in the marathon Best Prognosis Best Prognosis –Bystander cardiopulmonary resuscitation –Dx other than HCM NEJM: Jan 12, 2012
 10.9 Million Runners, 59 arrests (51 men) –Ages 43 +/- 13 yrs –Incidence rate =.54/100k Majority Due to CAD 1.01 per 100k in the marathon Best Prognosis Best Prognosis –Bystander cardiopulmonary resuscitation –Dx other than HCM NEJM: Jan 12, 2012")
10
CV Risks in Cardiac Rehabilitation 30 programs: 1960-1977 30 programs: 1960-1977 –1 Non-Fatal MI in 346,733 Pt. Hrs –1 Fatal MI in 116,402 Pt. Hrs 142 Programs: 1980-1984 142 Programs: 1980-1984 –1 Non-Fatal MI in 294k Pt. Hrs –1 Cardiac Death in 780k in Pt. Hrs –21 Cardiac Sudden Death (17 resuscitated) Chest: 1998 167 Programs: 105 Centers, 51k Patients, 2,361,967 Hrs 167 Programs: 105 Centers, 51k Patients, 2,361,967 Hrs –1 Cardiac Death in 60k Pt. Hrs (Medicine and Science in Sports and Exercise July 1994)
 Chest: Programs: 105 Centers, 51k Patients, 2,361,967 Hrs 167 Programs: 105 Centers, 51k Patients, 2,361,967 Hrs –1 Cardiac Death in 60k Pt. Hrs (Medicine and Science in Sports and Exercise July 1994).")
11
Acute Coronary Thrombosis in Boston Marathon Runners (2011) 3 Myocardial infractions (Men) Post Completion 3 Myocardial infractions (Men) Post Completion All: All: –Had coronary thrombosis –Traveled more than 4 Hrs. by Plane Prior –Elevated Thrombin, Anti-Thrombin Complex –None on cardiac medications NEJM: Jan 12, 2012

14
Sudden Cardiac Death

19
Detrimental Effects of Prolonged Endurance Exercise Increased: Heart Rate, BP and prolonged periods of Anaerobic Exercise. Increased: Heart Rate, BP and prolonged periods of Anaerobic Exercise. Increased: Aortic Stiffness, documented by increased Pulse Wave Velocity. Increased: Aortic Stiffness, documented by increased Pulse Wave Velocity. Greater: Coronary Calcium and increased Calcified Plaque Volume- 274mm cubed in prolonged endurance exercise group vs 169mm cubed in the control group. Greater: Coronary Calcium and increased Calcified Plaque Volume- 274mm cubed in prolonged endurance exercise group vs 169mm cubed in the control group. Scwartz, Am. Coll. Card. Sc. Sess., 3/16/10 Scwartz, Am. Coll. Card. Sc. Sess., 3/16/10

21
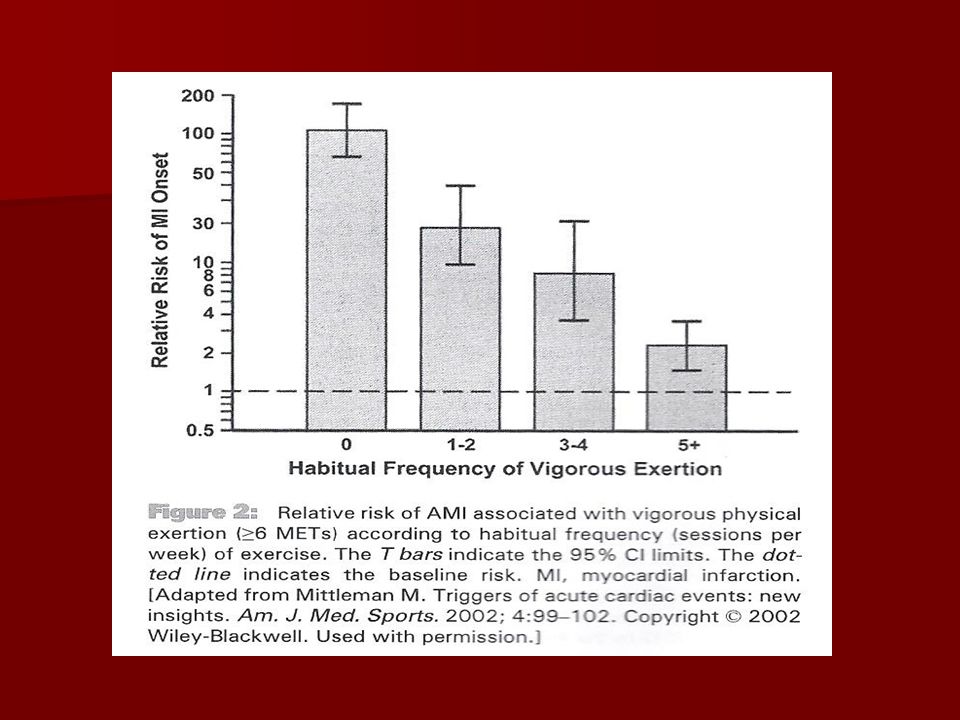
Timing of Infarction/Exercise (A) Increased: In First Hour Post Exercise (A) Increased: In First Hour Post Exercise 1. 218 Pts.: 4.4% Reported Heavy Exertion 1 Hr. Prior to MI 2. Fitness Level: Sedentary – 107 X Risk –Exercise: 1 – 2 X Week – 19.4 X Risk 3 – 4 X Week – 8.6 X Risk 3 – 4 X Week – 8.6 X Risk 4 – 5 X Week – 2.4 X Risk 4 – 5 X Week – 2.4 X Risk * Heavy physical exertion is much more likely to trigger infarction in the least fit. (Mittleman M. 1993) * Heavy physical exertion is much more likely to trigger infarction in the least fit. (Mittleman M. 1993)
 * Heavy physical exertion is much more likely to trigger infarction in the least fit. (Mittleman M. 1993).")
24
Mechanisms of MI/Exercise 1. Increased Inflammatory/Hemostatic Markers 1. Increased Inflammatory/Hemostatic Markers Increased: VWF : D-Dimer : D-Dimer : WBC : WBC : Platelet Aggregation : Platelet Aggregation : CRP(Siegel A. 2001) : CRP(Siegel A. 2001) 2. Changes in Cardiac Markers 2. Changes in Cardiac Markers Increased: Troponin I, Elevated 4 Hr. – 72 Hr. : CPK – MB – Peak 24 Hr. : CPK – MB – Peak 24 Hr. : Myoglobin – Peak 4 Hr. : Myoglobin – Peak 4 Hr. : BNP Peak 24 Hr. (Siegel A. 2001) : BNP Peak 24 Hr. (Siegel A. 2001) 3. Plaque Rupture 3. Plaque Rupture
 : CRP(Siegel A. 2001) 2. Changes in Cardiac Markers 2. Changes in Cardiac Markers Increased: Troponin I, Elevated 4 Hr. – 72 Hr. : CPK – MB – Peak 24 Hr. : CPK – MB – Peak 24 Hr. : Myoglobin – Peak 4 Hr. : Myoglobin – Peak 4 Hr. : BNP Peak 24 Hr. (Siegel A. 2001) : BNP Peak 24 Hr. (Siegel A. 2001) 3. Plaque Rupture 3. Plaque Rupture.")
25
Coagulation-Thrombolysis is in equilibrium during exercise Post-Exercise: A Hypercoagulable State is Present

26
Plaque Rupture/Thrombosis Atherosclerotic Heart Disease Atherosclerotic Heart Disease - Primary Cause of Death in Exercise Related Disease 81 Died suddenly, 75 Deaths – 2 nd to CAD (Ragosta M. 1984) Plaque Rupture/Intra-Coronary Clots Plaque Rupture/Intra-Coronary Clots - 640 Pts: (64) – Exercise VS. (576) – Rest - Clots 2MM Present in: 64% of Exercising Patients : 35% at Rest(Giri S. 1999) : 35% at Rest(Giri S. 1999)
 Plaque Rupture/Intra-Coronary Clots Plaque Rupture/Intra-Coronary Clots Pts: (64) – Exercise VS. (576) – Rest - Clots 2MM Present in: 64% of Exercising Patients : 35% at Rest(Giri S. 1999) : 35% at Rest(Giri S. 1999).")
32
Prodromal Symptoms (A). Chest Pain, Unexpected Dyspnea, Palpitations (A). Chest Pain, Unexpected Dyspnea, Palpitations (B). Seek Attention Immediately (B). Seek Attention Immediately (C). Denial (IE) Jim Fixx (Tragedy) (C). Denial (IE) Jim Fixx (Tragedy) 1. (6/13) Deaths during or immediately after exercise had prodromal symptoms before the event.(Thompson P. 1979) 1. (6/13) Deaths during or immediately after exercise had prodromal symptoms before the event.(Thompson P. 1979) 2. (36) Marathoners/Sudden Death: 71% had prodromal symptoms. 2. (36) Marathoners/Sudden Death: 71% had prodromal symptoms. (Noakes T. 1987) 3. (47%) prodromal symptoms at rest with ACS/Sedentary Men, 8% of athletes exercising. (Ciampricotti R. 1994 3. (47%) prodromal symptoms at rest with ACS/Sedentary Men, 8% of athletes exercising. (Ciampricotti R. 1994
. Seek Attention Immediately (B). Seek Attention Immediately (C). Denial (IE) Jim Fixx (Tragedy) (C). Denial (IE) Jim Fixx (Tragedy) 1. (6/13) Deaths during or immediately after exercise had prodromal symptoms before the event.(Thompson P. 1979) 1. (6/13) Deaths during or immediately after exercise had prodromal symptoms before the event.(Thompson P. 1979) 2. (36) Marathoners/Sudden Death: 71% had prodromal symptoms. 2. (36) Marathoners/Sudden Death: 71% had prodromal symptoms. (Noakes T. 1987) 3. (47%) prodromal symptoms at rest with ACS/Sedentary Men, 8% of athletes exercising. (Ciampricotti R (47%) prodromal symptoms at rest with ACS/Sedentary Men, 8% of athletes exercising. (Ciampricotti R")
33
CV Meds – No Significant Effect on Exercise Capacity 1. Alpha-blockers – prazosin, terazosin and doxazosin. 1. Alpha-blockers – prazosin, terazosin and doxazosin. 2. ACE Inhibitors/ARBS – captopril, lisinopril, quinapril, ramipril/losartan, valsartan 2. ACE Inhibitors/ARBS – captopril, lisinopril, quinapril, ramipril/losartan, valsartan 3. Venodilators – nitrates. 3. Venodilators – nitrates. Calcium Channel Blockers – the dihydropyridines, diltiazem and verapamil. Calcium Channel Blockers – the dihydropyridines, diltiazem and verapamil.

34
Cardiovascular Meds Having the Potential to Effect Exercise 1. Beta-blockers: inderal, metoprolol, atenolol and bisoprolol 1. Beta-blockers: inderal, metoprolol, atenolol and bisoprolol 2. Alpha beta-blockers: labetalol, carvedilol 2. Alpha beta-blockers: labetalol, carvedilol 3. Calcium channel blockers: verapamil 3. Calcium channel blockers: verapamil 4. Amiodarone – alpha beta-blocker 4. Amiodarone – alpha beta-blocker 5. Central alpha-blockers – clonidine 5. Central alpha-blockers – clonidine 6. Diuretics – thiazides, loop diuretics, potassium sparing 6. Diuretics – thiazides, loop diuretics, potassium sparing 7. Pure Vasodilators – hydralazine 7. Pure Vasodilators – hydralazine –(*1-5 have potential to limit heart rate response to exercise)
.")
35
Beta - Blockers 1. Decrease heart rate and cardiac output 1. Decrease heart rate and cardiac output 2. Decrease myocardial contractility 2. Decrease myocardial contractility 3. Decrease coronary blood flow 3. Decrease coronary blood flow 4. Decrease muscle blood flow 4. Decrease muscle blood flow 5. Cause premature fatigue during exercise 5. Cause premature fatigue during exercise A. Especially in non-selective beta-blockers B. Increased rating of perceived exertion (local) –a. Alters glycolytic metabolism –b. Decreased muscle blood flow
 –a. Alters glycolytic metabolism –b. Decreased muscle blood flow.")
36
Beta – Blockers, Continued 6. Decrease in VO2 max 6. Decrease in VO2 max 7. Decreased heart dissipation during exercise in hot weather. 7. Decreased heart dissipation during exercise in hot weather. 8. May cause hyperkalemia 8. May cause hyperkalemia 9. Beta-blockers are certainly necessary in many patients who have coronary artery disease, however, an attempt should be made to adjust the dosage of beta-blockers to attain at least 70% of predicted maximal heart rate or keep heart rate at levels below that causing ST depression, angina, adequate controlled ventricular response of atrial fibrillation or acceptable suppression of exercise induced arrhythmia. (Gullested L. 1996) 9. Beta-blockers are certainly necessary in many patients who have coronary artery disease, however, an attempt should be made to adjust the dosage of beta-blockers to attain at least 70% of predicted maximal heart rate or keep heart rate at levels below that causing ST depression, angina, adequate controlled ventricular response of atrial fibrillation or acceptable suppression of exercise induced arrhythmia. (Gullested L. 1996)
 9. Beta-blockers are certainly necessary in many patients who have coronary artery disease, however, an attempt should be made to adjust the dosage of beta-blockers to attain at least 70% of predicted maximal heart rate or keep heart rate at levels below that causing ST depression, angina, adequate controlled ventricular response of atrial fibrillation or acceptable suppression of exercise induced arrhythmia. (Gullested L. 1996).")
37
Diuretics 1. Will decrease plasma volume, which is the opposite effect of endurance training, which increases plasma volume, however cardiac output may not be appreciably affected. 1. Will decrease plasma volume, which is the opposite effect of endurance training, which increases plasma volume, however cardiac output may not be appreciably affected. 2. Hypokalemia may occur. Potassium regulates the maintenance of muscle blood flow. During exercise, marked hypokalemia may cause rhabdomyolysis and acute renal failure. 2. Hypokalemia may occur. Potassium regulates the maintenance of muscle blood flow. During exercise, marked hypokalemia may cause rhabdomyolysis and acute renal failure. 3. Diuretics may also cause low magnesium, which can precipitate tetani and may cause hypocalcemia and further aggravate hypokalemia. 3. Diuretics may also cause low magnesium, which can precipitate tetani and may cause hypocalcemia and further aggravate hypokalemia. 4. Potassium sparing diuretics may obviously spare potassium and magnesium, however, frequent monitoring of serum potassium should be performed to exclude hyperkalemia. 4. Potassium sparing diuretics may obviously spare potassium and magnesium, however, frequent monitoring of serum potassium should be performed to exclude hyperkalemia. 5. Hyponatremia, dehydration and hypovolemia. Certainly hyponatremia would also be more easily precipitated in excessive water drinkers who are “tanking up” for a long run. 5. Hyponatremia, dehydration and hypovolemia. Certainly hyponatremia would also be more easily precipitated in excessive water drinkers who are “tanking up” for a long run.

38
Vasodilators and Central Alpha Blockers 1. Vasodilators 1. Vasodilators –Hydralazine – may cause edema and reflex tachycardia. It is usually never used alone but in combination with a diuretic and/or beta-blocker and would be a poor choice for someone exercising. 2. Central Alpha Blockers 2. Central Alpha Blockers –Clonidine – may cause fatigue, bradycardia and/or heart block.

39
Miscellaneous 1. Amiodarone – will decrease heart rate and long term, may cause pulmonary complications leading to severe pulmonary insufficiency. 1. Amiodarone – will decrease heart rate and long term, may cause pulmonary complications leading to severe pulmonary insufficiency. 2. Pacemaker – should be activity modulated and programmed to react to appropriate levels of exercise to avoid pacer syndrome, allow an adequate heart rate to be attained at peak exercise. 2. Pacemaker – should be activity modulated and programmed to react to appropriate levels of exercise to avoid pacer syndrome, allow an adequate heart rate to be attained at peak exercise. 3. Post exercise hypotension – all anti hypertensive exaggerate the post exercise hypotensive response seen in normal subjects. 3. Post exercise hypotension – all anti hypertensive exaggerate the post exercise hypotensive response seen in normal subjects. 4. HMG – CoA reductase – inhibitors (statins) can cause muscle soreness. Rhabdomyolosis, increased skeletal muscle injury. 4. HMG – CoA reductase – inhibitors (statins) can cause muscle soreness. Rhabdomyolosis, increased skeletal muscle injury. (Thompson P. 1997)
 can cause muscle soreness. Rhabdomyolosis, increased skeletal muscle injury. 4. HMG – CoA reductase – inhibitors (statins) can cause muscle soreness. Rhabdomyolosis, increased skeletal muscle injury. (Thompson P. 1997).")
40
Cardiovascular Drugs The cardiovascular drugs that have the most favorable profile would be the class of alpha blockers, ACE inhibitors and ARB’s – venodilators, nitrates and slow calcium channel blockers with the exception of verapamil, which may cause a significant decrease in heart rate response at peak exercise. Also, of all the calcium channel blockers, it is more likely to cause muscle spasm or muscle fatigue.

42
Medications That May Prohibit Hyper-Coagulable State Post- Exercise ASA ASA Beta Blockers Beta Blockers Statins Statins ACE Inhibitors ACE Inhibitors

43
ASA Decreased platelet aggregation Decreased platelet aggregation Inhibit Cox-1 which produces Thromboxane A-2 Inhibit Cox-1 which produces Thromboxane A-2 –Necessary for platelet aggregation Decreased Tissue Factor in atherosclerotic plaques Decreased Tissue Factor in atherosclerotic plaques Lowers CRP Lowers CRP

44
Beta Blockers Blocks adrenaline increase in Factor VIII Blocks adrenaline increase in Factor VIII Reduces sympathetic response to exercise/arrhythmias Reduces sympathetic response to exercise/arrhythmias Reduces oxidative stress Reduces oxidative stress Reduces CRP Reduces CRP

45
Statins Down regulation of coagulation cascade Down regulation of coagulation cascade Beneficial effect on endothelial dependent vasodilation Beneficial effect on endothelial dependent vasodilation Reduced Thrombin production Reduced Thrombin production Anti-inflammatory properties Anti-inflammatory properties May stabilize plaques May stabilize plaques Lowers CRP Lowers CRP

46
Ace Inhibitors Anti-inflammatory and anti-fibrotic properties Anti-inflammatory and anti-fibrotic properties Reduces Tissue Factor in atherosclerotic plaques Reduces Tissue Factor in atherosclerotic plaques Reduces CRP Reduces CRP

48
Principles to Guide CV Therapy in Patients Who are Moderate to Competitive in their Levels of Exercise 1. Risk profile for all patients prior to starting exercise program. 1. Risk profile for all patients prior to starting exercise program. 2. Stress testing in patients who have multiple risk factors. 2. Stress testing in patients who have multiple risk factors. 3. Aggressively treat diabetes, hypertension, hyperlipidemia. 3. Aggressively treat diabetes, hypertension, hyperlipidemia. 4. Instruct patients not to ignore prodromal symptoms. 4. Instruct patients not to ignore prodromal symptoms. 5. Choose medications that are appropriate both for the patient’s diagnosis yet are least likely to limit their activity. 5. Choose medications that are appropriate both for the patient’s diagnosis yet are least likely to limit their activity. 6. Patient’s need to understand that they may need to readjust their exercise levels that are safe for them, i.e., keep heart rate response below angina or production of ST depression. Many times this is the difficult part of the equation (tell a runner that he or she needs to slow down.) 6. Patient’s need to understand that they may need to readjust their exercise levels that are safe for them, i.e., keep heart rate response below angina or production of ST depression. Many times this is the difficult part of the equation (tell a runner that he or she needs to slow down.) 7.Recommended heart rate monitors to all CV patients who exercise so that they can stay within their acceptable heart rate zone. 7.Recommended heart rate monitors to all CV patients who exercise so that they can stay within their acceptable heart rate zone.
 6. Patient’s need to understand that they may need to readjust their exercise levels that are safe for them, i.e., keep heart rate response below angina or production of ST depression. Many times this is the difficult part of the equation (tell a runner that he or she needs to slow down.) 7.Recommended heart rate monitors to all CV patients who exercise so that they can stay within their acceptable heart rate zone. 7.Recommended heart rate monitors to all CV patients who exercise so that they can stay within their acceptable heart rate zone..")
49
Principles to Guide CV Therapy in Patients Who are Moderate to Competitive in their Levels of Exercise 8. Recommend that each patient carry an ID card with as much medical 8. Recommend that each patient carry an ID card with as much medical information as possible. This may include lists of drugs, miniaturized copy of EKG, etc. 9. Stress the importance of warm up and cool down to avoid precipitation of angina and/or arrhythmia in the early stages of exercise and post exercise postural hypotension. 9. Stress the importance of warm up and cool down to avoid precipitation of angina and/or arrhythmia in the early stages of exercise and post exercise postural hypotension. 10. It may be wise for the patient to have their own blood pressure cuff and frequently check their blood pressure and weight prior to and after exercise as during long endurance runs, especially the morning of. It might also be wise to reduce the dosage of medications that are administered on a daily basis. 10. It may be wise for the patient to have their own blood pressure cuff and frequently check their blood pressure and weight prior to and after exercise as during long endurance runs, especially the morning of. It might also be wise to reduce the dosage of medications that are administered on a daily basis. 11. Balancing exercise levels and CV meds is at least time consuming and may require frequent visits for serial exercise testing to determine the dosage or choice of these medications. 11. Balancing exercise levels and CV meds is at least time consuming and may require frequent visits for serial exercise testing to determine the dosage or choice of these medications.

51
Summary Individuals participating in long distance running have a minimal risk for precipitation of acute cardiac events. This risk can probably be lowered by taking proper precautions and following prudent recommendations. Addressing treatable risk factors and risk profiling patients prior to participation is paramount. Patients on cardiac medications need to be made aware of potential side effects, which may be precipitated by exercise and the ability of these medications to limit performance. Following these principles, those with risk factors or known coronary artery disease, can reduce their risk for cardiac events during exercise and participate at levels of exercise promoting fitness and endurance.

52
Summary Physicians treating this group of patients should be able to recommend activity levels with hemodynamic parameters and prescribe cardiovascular medications both appropriate for the patient’s disease, yet preserving adequate hemodynamic response. Albeit a small cardiac risk will persist, especially in longer endurance events, which each participant needs to understand. Further data needs to be collected to increase understanding of these risks. Hopefully, future findings will assist in the reduction of acute cardiac events related to exercise.

53
Hypothesis Patients with known stable CAD who are receiving optimal medical treatment may be a lower risk for cardiovascular events than a similar age/gender groups during and in the one hour post-exercise period

55
Bibliography 1. Frere J, et al: The risk of death in running road races. The Physician and Sports Medicine 2004;32 (4): 33-40. 1. Frere J, et al: The risk of death in running road races. The Physician and Sports Medicine 2004;32 (4): 33-40. 2. Maron B, et al: Risk for sudden cardiac death associated with marathon running. AM J Cardiology 1996;28 (2): 428-431. 2. Maron B, et al: Risk for sudden cardiac death associated with marathon running. AM J Cardiology 1996;28 (2): 428-431. 3. Thompson P, et al: Incidence of death during jogging in Rhode Island from 1975 through 1980. JAMA 1982;247 (18): 2535-2538. 3. Thompson P, et al: Incidence of death during jogging in Rhode Island from 1975 through 1980. JAMA 1982;247 (18): 2535-2538. 4. Kavanagh T, et al: Marathon running after myocardial infarction. JAMA 1974;229 (12): 1602-1606. 4. Kavanagh T, et al: Marathon running after myocardial infarction. JAMA 1974;229 (12): 1602-1606. 5. Mittleman M, et al: Triggering of acute myocardial infarction by heavy exertion: protection against triggering by regular exercise. N Eng J Med 1993;329 (23): 1677-1683. 5. Mittleman M, et al: Triggering of acute myocardial infarction by heavy exertion: protection against triggering by regular exercise. N Eng J Med 1993;329 (23): 1677-1683. 6. Siegel A, et al: Effect of marathon running on inflammatory and hemostatic markers. AM J Cardiol 2001;88: 918-920. 6. Siegel A, et al: Effect of marathon running on inflammatory and hemostatic markers. AM J Cardiol 2001;88: 918-920.
: Frere J, et al: The risk of death in running road races. The Physician and Sports Medicine 2004;32 (4): Maron B, et al: Risk for sudden cardiac death associated with marathon running. AM J Cardiology 1996;28 (2): Maron B, et al: Risk for sudden cardiac death associated with marathon running. AM J Cardiology 1996;28 (2): Thompson P, et al: Incidence of death during jogging in Rhode Island from 1975 through JAMA 1982;247 (18): Thompson P, et al: Incidence of death during jogging in Rhode Island from 1975 through JAMA 1982;247 (18): Kavanagh T, et al: Marathon running after myocardial infarction. JAMA 1974;229 (12): Kavanagh T, et al: Marathon running after myocardial infarction. JAMA 1974;229 (12): Mittleman M, et al: Triggering of acute myocardial infarction by heavy exertion: protection against triggering by regular exercise. N Eng J Med 1993;329 (23): Mittleman M, et al: Triggering of acute myocardial infarction by heavy exertion: protection against triggering by regular exercise. N Eng J Med 1993;329 (23): Siegel A, et al: Effect of marathon running on inflammatory and hemostatic markers. AM J Cardiol 2001;88: Siegel A, et al: Effect of marathon running on inflammatory and hemostatic markers. AM J Cardiol 2001;88:")
56
Bibliography 7. Siegel A, et al: Changes in cardiac markers including B-Natriuretic Peptide in runners after the Boston Marathon. AM J of Cardiol 2001;88: 920-923. 7. Siegel A, et al: Changes in cardiac markers including B-Natriuretic Peptide in runners after the Boston Marathon. AM J of Cardiol 2001;88: 920-923. 8. Rogosta M, et al: Death during recreational exercise in the state of Rhode Island. Med Sci Sports Exer 1984;16 (4): 339-342. 8. Rogosta M, et al: Death during recreational exercise in the state of Rhode Island. Med Sci Sports Exer 1984;16 (4): 339-342. 9. Giri S, et al: Clinical and angiographic characteristics of exertion related acute myocardial infarction. JAMA 1999;228 (18): 1731-1736. 9. Giri S, et al: Clinical and angiographic characteristics of exertion related acute myocardial infarction. JAMA 1999;228 (18): 1731-1736. 10. Thompson PD, et al: Death during jogging or running: a study of 18 cases. JAMA 1979;242 (12): 1265-1267. 10. Thompson PD, et al: Death during jogging or running: a study of 18 cases. JAMA 1979;242 (12): 1265-1267. 11. Noakes TD: Heart disease in marathon runners: a review. Med Sci Sports Exer 1987;19 (3): 187-194. 11. Noakes TD: Heart disease in marathon runners: a review. Med Sci Sports Exer 1987;19 (3): 187-194. 12. Ciampricotti R, et al: Characteristics of conditioned and sedentiary men with acute coronary syndromes. Am J Cardiol 1994;74 (4): 219-222. 12. Ciampricotti R, et al: Characteristics of conditioned and sedentiary men with acute coronary syndromes. Am J Cardiol 1994;74 (4): 219-222.
: Rogosta M, et al: Death during recreational exercise in the state of Rhode Island. Med Sci Sports Exer 1984;16 (4): Giri S, et al: Clinical and angiographic characteristics of exertion related acute myocardial infarction. JAMA 1999;228 (18): Giri S, et al: Clinical and angiographic characteristics of exertion related acute myocardial infarction. JAMA 1999;228 (18): Thompson PD, et al: Death during jogging or running: a study of 18 cases. JAMA 1979;242 (12): Thompson PD, et al: Death during jogging or running: a study of 18 cases. JAMA 1979;242 (12): Noakes TD: Heart disease in marathon runners: a review. Med Sci Sports Exer 1987;19 (3): Noakes TD: Heart disease in marathon runners: a review. Med Sci Sports Exer 1987;19 (3): Ciampricotti R, et al: Characteristics of conditioned and sedentiary men with acute coronary syndromes. Am J Cardiol 1994;74 (4): Ciampricotti R, et al: Characteristics of conditioned and sedentiary men with acute coronary syndromes. Am J Cardiol 1994;74 (4):")
57
Bibliography 13. Gullested L, et al: The effect of acute vs. chronic treatment with B-adrenoceptor blockade on exercise performance, haemodynamics and metabolic parameters in healthy men and women. Br J Clin Pharmacal 1996;41: 57-67. 13. Gullested L, et al: The effect of acute vs. chronic treatment with B-adrenoceptor blockade on exercise performance, haemodynamics and metabolic parameters in healthy men and women. Br J Clin Pharmacal 1996;41: 57-67. 14. Thompson P, et al: Lovastatin increased exercise induced skeletal muscle injury. Metabolism 1997;46 (10): 1206-1210. 14. Thompson P, et al: Lovastatin increased exercise induced skeletal muscle injury. Metabolism 1997;46 (10): 1206-1210.
: Thompson P, et al: Lovastatin increased exercise induced skeletal muscle injury. Metabolism 1997;46 (10):")
58
Suggested Reading 1. ACSM’s Guide for Exercise Testing and Prescription— Eighth Edition. 2010. Lippincott Williams and Wilkins. 1. ACSM’s Guide for Exercise Testing and Prescription— Eighth Edition. 2010. Lippincott Williams and Wilkins. 2. Thompson PD: Exercise and Sports Cardiology. 2001. McGraw Hill. 2. Thompson PD: Exercise and Sports Cardiology. 2001. McGraw Hill.

Similar presentations

























 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")







